 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Ziyad S. Haidar | + 1430 word(s) | 1430 | 2022-03-10 04:33:26 | | | |
| 2 | Yvaine Wei | -10 word(s) | 1420 | 2022-03-11 02:40:49 | | |
Video Upload Options
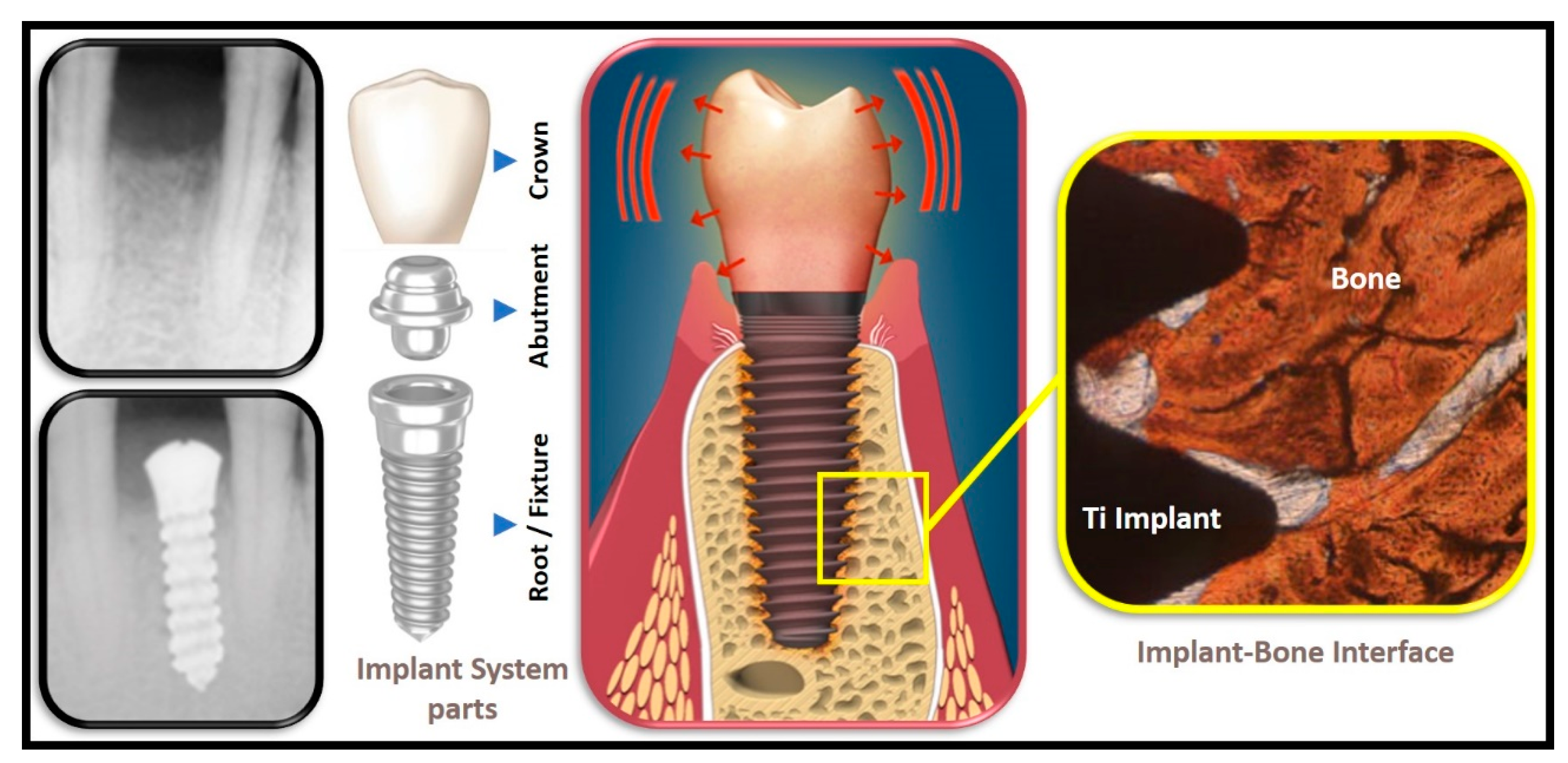
Heat is a kinetic process whereby energy flows from between two systems, hot-to-cold objects. In oro-dental implantology, conductive heat transfer/(or thermal stress) is a complex physical phenomenon to analyze and consider in treatment planning. Hence, ample research has attempted to measure heat-production to avoid over-heating during bone-cutting and drilling for titanium (Ti) implant-site preparation and insertion, thereby preventing/minimizing early (as well as delayed) implant-related complications and failure. The goal is two-fold: (A) the standard heat equation is proposed to be solved, modifying the imposed boundary conditions without any additional source term, and on the other hand, (B) a gap is filled in the literature via obtaining an exact analytical solution of a somewhat simplified problem, which nevertheless, encapsulates the physics and reproduces the results already found in previous works via numerical analyses. In addition, for the first time, the intrinsic time is introduced and involved herein, a “proper” time that characterizes the geometry of the dental implant fixture and overall system, and how the interplay between that time and the exposure time influences temperature changes, and subsequent implant survival, are shown. Thus, this work aims to complement the overall clinical diagnostic and treatment plan for enhanced biological one–implant interface and mechanical implant stability and success rates, whether for immediate or delayed implant loading strategies.
1. Introduction
2. Thermal Load and Heat Transfer
Formulation of the Physical Problem
3. Conclusions
References
- Aida, J.; Ando, Y.; Akhter, R.; Aoyama, H.; Masui, M.; Morita, M. Reasons for permanent tooth extractions in Japan. J. Epidemiol. 2006, 16, 214–219.
- Abnet, C.C.; Qiao, Y.L.; Dawsey, S.M.; Dong, Z.W.; Taylor, P.R.; Mark, S.D. Tooth loss is associated with increased risk of total death and death from upper gastrointestinal cancer, heart disease, and stroke in a Chinese population-based cohort. Int. J. Epidemiol. 2005, 34, 467–474.
- Holm-Pedersen, P.; Schultz-Larsen, K.; Christiansen, N. Tooth Loss and Subsequent Disability and Mortality in Old Age. J. Am. Geriatr. Soc. 2008, 56, 429–435.
- Holmlund, A.; Holm, G.; Lind, L. Number of Teeth as a Predictor of Cardiovascular Mortality in a Cohort of 7674 Subjects Followed for 12 Years. J. Periodontol. 2010, 81, 870–876.
- Scheid, R.C.; Woelfel, J.B. Woelfel’s Dental Anatomy: Its Relevance to Dentistry, 7th ed.; Lippincote Williams & Wilkins: Baltimore, MD, USA, 2007.
- Marenzi, G.; Sammartino, J.C.; Quaremba, G.; Graziano, V.; El Hassanin, A.; Qorri, M.E.; Sammartino, G.; Iorio-Siciliano, V. Clinical Influence of Micromorphological Structure of Dental Implant Bone Drills. Biomed. Res. Int. 2018, 2018, 8143962.
- Kalidindi, V. Optimization of Drill Design and Coolant Systems during Dental Implant Surgery. Master’s Theses, University of Kentucky, Lexington, KY, USA, 2004.
- Linsuwanont, P.; Versluis, A.; Palamara, J.E.; Messera, H.H. Thermal stimulation causes tooth deformation: A possible alternative to the hydrodynamic theory? Arch. Oral Biol. 2008, 53, 261–272.
- McCullagh, P.; Setchell, D.J.; Nesbit, M.; Biagioni, P.A.; Lamey, P.J. Infrared thermographic analysis of temperature rise on implant surfaces: A pilot study on abutment preparation. Pract. Periodontics Aesthet. Dent. 1998, 10, 1163–1167.
- Gross, M.; Lanfer, B.Z.; Ormianer, Z. An investigation on heat transfer to the implant-bone interface due to abutment preparation with high-speed cutting instruments. Int. J. Oral Maxillofac. Implant. 1995, 10, 207–212.
- Bragger, U.; Wermuth, W.; Torok, E. Heat generated during preparation of titanium implants of the ITI® Dental Implant System: An in vitro study. Clin. Oral Implant. Res. 1995, 6, 254–259.
- Ormianer, Z.; Lanfer, B.-Z.; Nissan, J.; Gross, M. An Investigation of Heat Transfer to the Implant-Bone Interface Related to Exothermic Heat Generation during Setting of Autopolymerizing Acrylic Resins Applied Directly to an Implant Abutment. Int. J. Oral Maxillofac. Implant. 2000, 15, 837–842.
- Feuerstein, O.; Zeichner, K.; Imbari, C.; Ormianer, Z.; Samet, N.; Weiss, E.I. Temperature changes in dental implants following exposure to hot substances in an ex vivo model. Clin. Oral Implant. Res. 2008, 19, 629–633.
- Nissan, J.; Gross, M.; Ormianer, Z.; Barnea, E.; Assif, D. Heat Transfer of Impression Plasters to an Implant-Bone Interface. Implant Dent. 2006, 15, 83–88.
- Oskui, I.Z.; Ashtiani, M.N.; Hashemi, A.; Jafarzadeh, H. Effect of thermal stresses on the mechanism of tooth pain. J. Endod. 2014, 40, 1835–1839.
- Wood, M.R.; Vermilyea, S.G.; Committee on Research in Fixed Prosthodontics of the Academy of Fixed Prosthodontics. A review of selected dental literature on evidence-based treatment planning for dental implants: Report of the Committee on Research in Fixed Prosthodontics of the Academy of Fixed Prosthodontics. J. Prosthet. Dent. 2004, 92, 447–462.
- Li, S.; Chien, S.; Brånemark, P.I. Heat shock-induced necrosis and apoptosis in osteoblasts. J. Orthop. Res. 1999, 17, 891–899.
- Patel, Z.; Geerts, G.A. Temperature changes along a dental implant. Int. J. Prosthodont. 2011, 24, 58–63.
- Eriksson, A.R.; Albrektsson, T. Temperature threshold levels for heat-induced bone tissue injury: A vital-microscopic study in the rabbit. J. Prosthet. Dent. 1983, 50, 101–107.
- Eriksson, R.A.; Albrektsson, T. The effect of heat on bone regeneration: An experimental study in the rabbit using the bone growth chamber. J. Oral Maxillofac. Surg. 1984, 42, 705–711.
- Ormianer, Z.; Feuerstein, O.; Assad, R.; Samet, N.; Weiss, E.I. In vivo changes in dental implant temperatures during hot beverage intake: A pilot study. Implant Dent. 2009, 18, 38–45.
- Palmer, D.S.; Barco, M.T.; Billy, E.J. Temperature extremes produced orally by hot and cold liquids. J. Prosthet. Dent. 1992, 67, 325–327.
- Barclay, C.W.; Spence, D.; Laird, W.R. Intra-oral temperatures during function. J. Oral Rehabil. 2005, 32, 886–894.
- Wong, K.; Boyde, A.; Howell, P.G. A model of temperature transients in dental implants. Biomaterials 2001, 22, 2795–2797.
- Rabbani Arshad, S.; Zoljanahi Oskui, I.; Hashemi, A. Thermal Analysis of Dental Implants in Mandibular Premolar Region: 3D FEM Study. J. Prosthodont. 2018, 27, 284–289.
- Yeo, I.S.; Lee, J.H.; Kang, T.J.; Kim, S.K.; Heo, S.J.; Koak, J.Y.; Park, J.M.; Lee, S.Y. The effect of abutment screw length on screw loosening in dental implants with external abutment connections after thermocycling. Int. J. Oral Maxillofac. Implant. 2014, 29, 59–62.
- Çelik Köycü, B.; İmirzalıoğlu, P. Heat Transfer and Thermal Stress Analysis of a Mandibular Molar Tooth Restored by Different Indirect Restorations Using a Three-Dimensional Finite Element Method. J. Prosthodont. 2017, 26, 460–473.
- Oskui, I.Z.; Ashtiani, M.N.; Hashemi, A.; Jafarzadeh, H. Thermal analysis of the intact mandibular premolar: A finite element analysis. Int. Endod. J. 2013, 46, 841–846.
- Ma, W.; Liu, W.; Li, M. Modeling heat transfer from warm water to foot: Analytical solution and experimental validation. Int. J. Therm. Sci. 2015, 98, 364–373.
- Turkyilmazoglu, M. Heat trasfer from warm water to a moving foot in a footbath. Appl. Therm. Eng. 2016, 98, 280–287.
- Wang, F.; Lee, H.P.; Lu, C. Thermal-mechanical study of functionally graded dental implants with the finite element method. J. Biomed. Mater. Res. A 2007, 80, 146–158.
- Rosentritt, M.; Raab, P.; Hahnel, S.; Stöckle, M.; Preis, V. In-vitro performance of CAD/CAM-fabricated implant-supported temporary crowns. Clin. Oral Investig. 2017, 21, 2581–2587.
- Rayyan, M.M.; Abdallah, J.; Segaan, L.G.; Bonfante, E.A.; Osman, E. Static and Fatigue Loading of Veneered Implant-Supported Fixed Dental Prostheses. J. Prosthodont. 2020, 29, 679–685.
- Davó, R.; Felice, P.; Pistilli, R.; Barausse, C.; Marti-Pages, C.; Ferrer-Fuertes, A.; Ippolito, D.R.; Esposito, M. Immediately loaded zygomatic implants vs conventional dental implants in augmented atrophic maxillae: 1-year post-loading results from a multicentre randomised controlled trial. Eur. J. Oral Implantol. 2018, 11, 145–161.
- Felice, P.; Checchi, L.; Barausse, C.; Pistilli, R.; Sammartino, G.; Masi, I.; Ippolito, D.R.; Esposito, M. Posterior jaws rehabilitated with partial prostheses supported by 4.0 × 4.0 mm or by longer implants: One-year post-loading results from a multicenter randomised controlled trial. Eur. J. Oral Implantol. 2016, 9, 35–45.


