 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Ana Fonseca | + 1566 word(s) | 1566 | 2022-01-17 04:49:27 | | | |
| 2 | Maria Guerreiro | -11 word(s) | 1555 | 2022-01-19 20:58:59 | | | | |
| 3 | Nelson Azevedo Barros | -6 word(s) | 1560 | 2022-01-20 00:23:21 | | | | |
| 4 | Yvaine Wei | Meta information modification | 1560 | 2022-01-20 05:11:27 | | |
Video Upload Options
Indoor air quality (IAQ) in Healthcare Units is a complex and dynamic issue of utmost importance for patient safety and occupational health purposes, since healthcare providers, medical practitioners, staff and patients spend long hours in the facilities subject to their inherent air quality. IAQ is affected by outdoor air quality, indoor activities, indoor occupant density, ventilation practices, indoor intrinsic emissions (e.g., equipment/furniture/coatings).
The presence of vulnerable individuals and the characteristics of the ongoing activities highlight the importance of adequately managing IAQ in healthcare facilities. Headaches, fatigue, dryness and irritation of the eyes and skin are common complaints of healthcare professionals, which have often been associated with poor IAQ. In addition, hospitals operate on a full-time basis (24 h per day, seven days a week), with no idle time to recover from activities’ emissions and consequent impact on IAQ.
1. Introduction
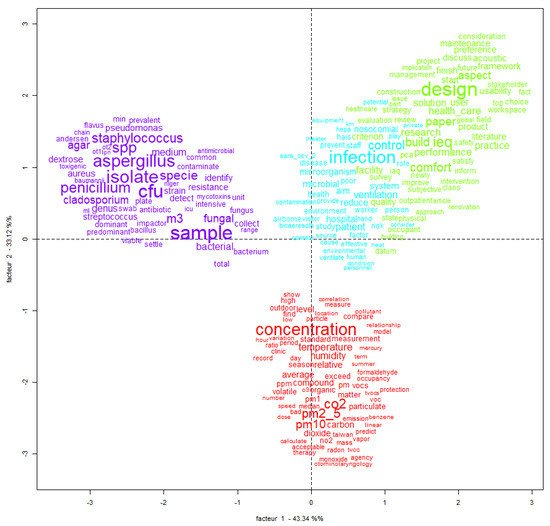
2. Textometric Analysis
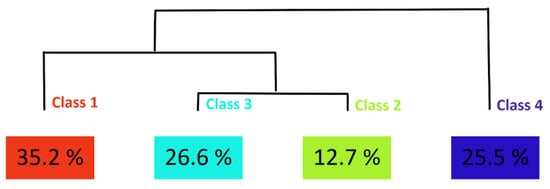
The analysis of the semantic fields in each cluster identified in the dendrogram suggests the following categorization of the studies developed in the sample papers:
- Cluster 1 is related to studies focusing on physicochemical parameters. The most impacted words (higher Chi-squared values) are: concentration (120.2), CO2 (89.6), PM2.5 (79.6), PM10 (64.7), temperature (53.2) and humidity (49.7). The analysis of the studies categorized in this cluster highlights the following issues: outdoor pollution sources should be addressed when evaluating indoor air quality [14], as should meteorological conditions [15]; isolated parameters—Radon gas [15] and CO2 [7]—could be used to assess health risks in healthcare facilities; mercury vapors and VOCs in dental clinics are important issues which are still underexplored [16]; particles and VOCs released through surgical smoke in operating rooms are a concern for IAQ [17]; anatomopathological activities are associated with the significant release of organic contaminants to indoor air [18].Studies were found with no significant association with only one cluster. Articles frequently focus on environmental control measures considering both physicochemical and microbiological contaminants [24]. Ventilation management and control is of the utmost importance to reduce microbiological and physicochemical contamination in healthcare facilities [7][21][22][23].
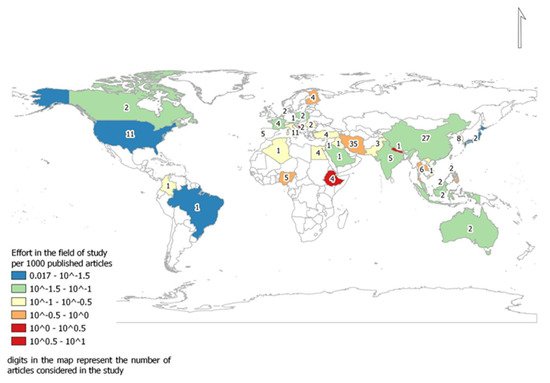
3. Contributions per Country
4. Parameters under Study
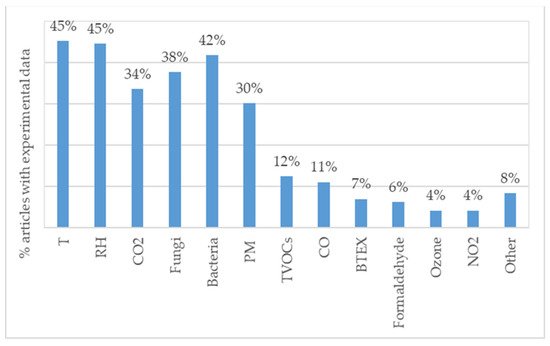
Situations of non-compliance with the WHO guidelines for indoor air quality are frequently reported, evidencing the need for further research investments leading to improvements in this area.
There are research opportunities for studies focusing on other important pollutants (e.g., ultrafine particles and PAH compounds). Moreover, research gaps exist regarding the formation of secondary pollutants from interactions between chemical contaminants, including those from outdoor air, and risk assessments on the synergistic interactions between chemical contaminants and microbiological loads.
It is well established that the design of facilities, the choice of adequate materials for construction and renovation, and the adequacy of management procedures towards IAQ improvement should be based on scientific research and data analysis. Therefore, these topics are promising lines of research that may lead to improvements in the indoor air quality in healthcare facilities, with potentially relevant impacts on patient safety and occupational health.
References
- World Heath Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; World Heath Organization: Geneva, Switzerland, 2021; pp. ISBN 9789240034228.
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Under-5 Mortality and Adult Mortality 1950–2019; Institute for Health Metrics and Evaluation (IHME) : Seatle, USA, 2020; pp. 1.
- World Health Organization. Combined or Multiple Exposure to Health Stressors in Indoor Built Environments: An Evidence-BasedReview Prepared for the WHO Training Workshop “Multiple Environmental Exposures and Risks”: 16–18 October 2013, Bonn, Germany;World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2013.
- Estelle Baurès; Olivier Blanchard; Fabien Mercier; Emilie Surget; Pierre LE Cann; Alexandre Rivier; Jean-Pierre Gangneux; Arnaud Florentin; Indoor air quality in two French hospitals: Measurement of chemical and microbiological contaminants. Science of The Total Environment 2018, 642, 168-179, 10.1016/j.scitotenv.2018.06.047.
- Marco Gola; Gaetano Settimo; Stefano Capolongo; Indoor Air Quality in Inpatient Environments: A Systematic Review on Factors that Influence Chemical Pollution in Inpatient Wards. Journal of Healthcare Engineering 2019, 2019, 1-20, 10.1155/2019/8358306.
- Clive B Beggs; Luke Knibbs; Graham Johnson; Lidia Morawska; Environmental contamination and hospital-acquired infection: factors that are easily overlooked. Indoor Air 2014, 25, 462-474, 10.1111/ina.12170.
- Ana Fonseca; Isabel Abreu; Maria João Guerreiro; Cristina Abreu; Ricardo Silva; Nelson Barros; Indoor Air Quality and Sustainability Management—Case Study in Three Portuguese Healthcare Units. Sustainability 2018, 11, 101, 10.3390/su11010101.
- Sarah H. Widder; Liv Haselbach; Relationship among Concentrations of Indoor Air Contaminants, Their Sources, and Different Mitigation Strategies on Indoor Air Quality. Sustainability 2017, 9, 1149, 10.3390/su9071149.
- Magdalena Kruza; Alastair Lewis; G. C. Morrison; N. Carslaw; Impact of surface ozone interactions on indoor air chemistry: A modeling study. Indoor Air 2017, 27, 1001-1011, 10.1111/ina.12381.
- Mauro Cannistraro; Ernesto Bernardo; Monitoring of the indoor microclimate in hospital environments a case study the Papardo hospital in Messina. International Journal of Heat and Technology 2017, 35, 456-465, 10.18280/ijht.35Sp0162.
- Manish K. Dixit; Shashank Singh; Sarel Lavy; Wei Yan; Floor finish selection in health-care facilities: a systematic literature review. Facilities 2019, 37, 897-918, 10.1108/f-03-2018-0042.
- Matthew J. Page; Joanne E. McKenzie; Patrick M. Bossuyt; Isabelle Boutron; Tammy C. Hoffmann; Cynthia D. Mulrow; Larissa Shamseer; Jennifer M. Tetzlaff; Elie A. Akl; Sue E. Brennan; et al.Roger ChouJulie GlanvilleJeremy M. GrimshawAsbjørn HróbjartssonManoj M. LaluTianjing LiElizabeth W. LoderEvan Mayo-WilsonSteve McDonaldLuke A. McGuinnessLesley A. StewartJames ThomasAndrea C. TriccoVivian A. WelchPenny WhitingDavid Moher The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. International Journal of Surgery 2021, 88, 105906, 10.1016/j.ijsu.2021.105906.
- IRaMuTeQ Software . iramuteq. Retrieved 2022-1-17
- Ashraf Chamseddine; Ibrahim Alameddine; M. Hatzopoulou; M. El-Fadel; Seasonal variation of air quality in hospitals with indoor–outdoor correlations. Building and Environment 2018, 148, 689-700, 10.1016/j.buildenv.2018.11.034.
- Kazemi, K. V; Mansouri, N.; Moattar, F.; Khezri, S.M.; Characterization of indoor/outdoor PM10, PM2.5, PM1 and radon concentrations in Imam Khomeini hospital. Bulgarian Chemical Communications 2016, 48, 345–350.
- Afolabi Oyapero; Adolphous Odofin Loto; Adenike Ololade Awotile; A Olugbenga Adenuga-Taiwo; Lillian Lami Enone; Ifeoma Nkiruka Menakaya; Managing amalgam phase down: An evaluation of mercury vapor levels in a dental center in Lagos, Nigeria. Journal of Dental Research and Review 2017, 4, 4-8, 10.4103/jdrr.jdrr_20_17.
- Mark H. Ereth; Donald H. Hess; Abigail Driscoll; Mark Hernandez; Frank Stamatatos; Particle control reduces fine and ultrafine particles greater than HEPA filtration in live operating rooms and kills biologic warfare surrogate. American Journal of Infection Control 2020, 48, 777-780, 10.1016/j.ajic.2019.11.017.
- Massimo Cipolla; Alberto Izzotti; Filippo Ansaldi; Paolo Durando; Maria Teresa Piccardo; Volatile Organic Compounds in Anatomical Pathology Wards: Comparative and Qualitative Assessment of Indoor Airborne Pollution. International Journal of Environmental Research and Public Health 2017, 14, 609, 10.3390/ijerph14060609.
- Marco Gola; Gaetano Settimo; Stefano Capolongo; Chemical Pollution in Healing Spaces: The Decalogue of the Best Practices for Adequate Indoor Air Quality in Inpatient Rooms. International Journal of Environmental Research and Public Health 2019, 16, 4388, 10.3390/ijerph16224388.
- So Fujiyoshi; Daisuke Tanaka; Fumito Maruyama; Transmission of Airborne Bacteria across Built Environments and Its Measurement Standards: A Review. Frontiers in Microbiology 2017, 8, 2336-2336, 10.3389/fmicb.2017.02336.
- Gola, M.; Caggiano, G.; De Giglio, O.; Napoli, C.; Diella, G.; Carlucci, M.; Carpagnano, L.F.; D’Alessandro, D.; Joppolo, C.M.; Capolongo, S.; et al.et al. SARS-CoV-2 indoor contamination: considerations on anti-COVID-19 management of ventilation systems, and finishing materials in healthcare facilities. Annali di igiene : medicina preventiva e di comunita 2020, 33(4), 381-392, 10.7416/ai.2020.2396.
- Ling Fu Shaw; Ian Horng Chen; Chii Shya Chen; Hui Hsin Wu; Li Shing Lai; Yin Yin Chen; Fu Der Wang; Factors influencing microbial colonies in the air of operating rooms. BMC Infectious Diseases 2018, 18, 1-8, 10.1186/s12879-017-2928-1.
- Rebecca E. Stockwell; Emma L. Ballard; Peter O’Rourke; Luke D. Knibbs; Lidia Morawska; Scott C. Bell; Indoor hospital air and the impact of ventilation on bioaerosols: a systematic review. Journal of Hospital Infection 2019, 103, 175-184, 10.1016/j.jhin.2019.06.016.
- Wendy Beatriz Morgado-Gamero; Martha Mendoza Hernandez; Margarita Castillo Ramirez; Jhorma Medina-Altahona; Stephanie De La Hoz; Heidy Posso Mendoza; Alexander Parody; Elba C. Teixeira; Dayana Milena Agudelo-Castañeda; Antibiotic Resistance of Airborne Viable Bacteria and Size Distribution in Neonatal Intensive Care Units. International Journal of Environmental Research and Public Health 2019, 16, 3340, 10.3390/ijerph16183340.
- Carla Viegas; Beatriz Almeida; Ana Monteiro; Liliana Aranha Caetano; Elisabete Carolino; Anita Quintal Gomes; Magdalena Twarużek; Robert Kosicki; Geneviéve Marchand; Susana Viegas; et al. Bioburden in health care centers: Is the compliance with Portuguese legislation enough to prevent and control infection?. Building and Environment 2019, 160, 106226, 10.1016/j.buildenv.2019.106226.
- The World Bank . Scientific and technical journal articles. Retrieved 2022-1-19

