Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Javier Díaz Castro | + 1934 word(s) | 1934 | 2021-12-29 09:36:18 | | | |
| 2 | Jason Zhu | Meta information modification | 1934 | 2021-12-30 02:30:18 | | | | |
| 3 | Jorge Moreno-Fernandez | Meta information modification | 1934 | 2022-01-10 08:40:56 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Díaz Castro, J.; Moreno-Fernandez, J. Vitamin C against COVID-19. Encyclopedia. Available online: https://encyclopedia.pub/entry/17635 (accessed on 24 July 2026).
Díaz Castro J, Moreno-Fernandez J. Vitamin C against COVID-19. Encyclopedia. Available at: https://encyclopedia.pub/entry/17635. Accessed July 24, 2026.
Díaz Castro, Javier, Jorge Moreno-Fernandez. "Vitamin C against COVID-19" Encyclopedia, https://encyclopedia.pub/entry/17635 (accessed July 24, 2026).
Díaz Castro, J., & Moreno-Fernandez, J. (2021, December 29). Vitamin C against COVID-19. In Encyclopedia. https://encyclopedia.pub/entry/17635
Díaz Castro, Javier and Jorge Moreno-Fernandez. "Vitamin C against COVID-19." Encyclopedia. Web. 29 December, 2021.
Copy Citation
Vitamin C is a nutrient required as a cofactor for multiple enzymatic reactions, such us norepinephrine biosynthesis, collagen hydroxylation, or amidation of peptide hormones. Additionally, it exerts a wide range of properties that could come in handy for the prevention and treatment of infections, including antioxidant, immunomodulating, as well as antiviral and antithrombotic functions.
COVID-19
Vitamin C
ROS
antioxidant
1. Vitamin C Mechanisms of Action
Vitamin C is mostly renowned for being a classical and potent antioxidant, quenching free radicals while being transformed into its oxidized form (dehydro-ascorbic acid). It also helps to restore other antioxidant molecules, such as vitamin E and tetrahydrobiopterin. Furthermore, it may potentiate the pharmacological effects carried out by flavonoids (for example quercetin), so an association between them could possibly exert a valuable synergistic antioxidant activity through a combination of the scavenging mechanisms performed by flavonoids and the transcription-modulating and scavenging mechanisms performed by ascorbic acid. However, this is only theoretical, so further investigation would be needed to clarify the usefulness of this combination in vivo [1]. The mainvitamin C mechanisms of action are summarized in Figure 1.
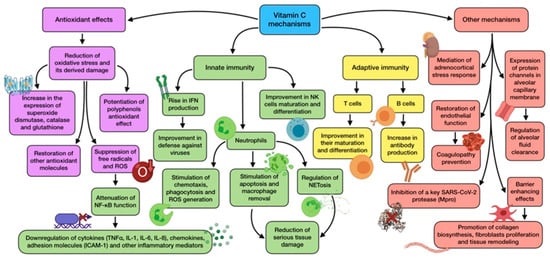
Figure 1. Summary of the main vitamin C mechanisms of action.
Oxidative stress is a frequent feature during infection and inflammation, owing to the release of ROS from activated phagocytes as part of the host response to pathogens. As for COVID-19, neutrophil-derived oxidative stress is thought to produce tissue damage [2]. Vitamin C optimal status is associated with less oxidative stress, has been reported to repair oxidative damage in bronchial epithelium, and is also able to prevent ROS-induced lung damage [3]. Ascorbic acid antioxidant role interacts with its immunomodulatory activity through nuclear transcription factor NF-κB. The reduction in ROS promoted by vitamin C attenuates NF-κB function, thus avoiding transcription of pro-inflammatory genes regulated by it. This includes the ones that encode TNFα, IL-1, IL-6, and IL-8; some chemokines; adhesion molecules (ICAM-1); and other inflammatory mediators. This leads to a downregulation of inflammatory cytokine production and, as a consequence, a mitigation in the severity of cytokine storm triggered by ARDS [4]. In addition, epigenetic regulation of genes by vitamin C also affects human natural antioxidant mechanisms, such as superoxide dismutase, catalase, and glutathione, whose expression seems to be increased by this nutrient [4][5].
A proper vitamin C status plays a role in immunity (both innate and adaptive) and host susceptibility to infection, as it accumulates in leukocytes and maintains their normal functioning, especially in neutrophils [6]. It has not only proved to stimulate neutrophil chemotaxis and migration to the site of infection, but also their phagocytic function and ROS generation [4]. Moreover, vitamin C is able to support neutrophil apoptosis and enhance macrophage removal, avoiding serious damage in host tissue [7]. This vitamin has also been reported to have a role in regulation of neutrophil extracellular traps (NETosis). This is a cell death pathway, distinct from apoptosis and necrosis, whose objective is the inactivation of pathogens. However, an excess in this response is considered a maladaptive feature which contributes to tissue damage and organ failure, as implicated in COVID-19 thrombotic complications. Ascorbic acid deficiency in septic animals has shown to increase plasma cell-free DNA generated from NETosis, so administration could attenuate this detrimental process [8][9].
Vitamin C is also related to other immune cells, including T and NK cells, whose maturation and differentiation is promoted by this nutrient [10]. Ascorbic acid-deficient diet has been reported to decrease vitamin C cell content, reducing T cell activity and ability to recall antigens [11]. It is also involved in antibody production by peripheral blood B cells. Age-related vitamin deficiency is associated with low serum levels of IgM and IgG, thus presenting a situation that would be reverted with supplementation [11][6].
One of the most important antiviral effects that vitamin C exerts is related to its ability to rise IFN production. While SARS-CoV-2 downregulates IFN expression and release, ascorbic acid is able to enhance it, thus allowing this antiviral cytokine to carry out its key defensive role against viruses [9]. Vitamin C also shows several barrier-enhancing effects that cooperate in maintaining epithelial integrity. Collagen biosynthesis requires participation, and is only negatively affected by severe vitamin C deficiency. This vitamin can also modify gene expression in dermal fibroblasts, promoting their proliferation and, therefore, tissue remodeling [12].
There is also increasing evidence which points out that vitamin C might play a critical role in mediating the adrenocortical stress response. Adrenal glands have three times more vitamin C concentration than any other organ, and are released from the adrenal cortex during physiological stress situations, such as viral exposure. The increased vitamin levels enhance cortisol production and potentiates anti-inflammatory and endothelial-protective effects carried out by glucocorticoids [13]. Furthermore, vitamin C may also be beneficial with regard to another common issue in COVID-19, known as coagulopathy. As vitamin C is able to restore endothelial function, it would help decrease the risk of these complications. Early injection has shown to prevent microtrombi formation and capillary plugging [8]. Likewise, lower concentrations of tissue plasminogen activator (tPA) and C reactive protein have been related to an increased dietary vitamin intake [12].
On account of all these mechanisms and functions, and through many in vitro studies, animal experiments, and clinical trials, vitamin C has been reported to exhibit antiviral properties against a wide range of microbes involved in several diseases, including influenza, common cold, and even coronavirus [14]. Pre-clinical data show that ascorbic acid may have a direct antiviral effect against both RNA and DNA viruses. Nevertheless, if vitamin C also has this effect against viral replication in vivo is yet to be confirmed [6]. With regard to SARS-CoV-2, the possible relationship between a key virus protease (M-pro) and vitamin C has become noteworthy, as an in-silico study revealed that the active site of this enzyme has the strongest binding with magnesium ascorbate, out of 106 nutraceuticals. Therefore, this evidence suggests that ascorbate may be a powerful enzyme inhibitor [15]. Despite the acknowledged properties of vitamin C, whether or not they are translated into a real beneficial effect in the response to COVID-19 remain to be elucidated, even though findings point to a significant potential to ameliorate negative consequences of SARS-CoV-2 infection and possibly become a feasible treatment option [16].
2. Evidence about Vitamin C Regarding Respiratory Infections and COVID-19
There is a belief that vitamin C helps to prevent and treat upper respiratory tract infections (URT). However, the dose needed (1–2 g/d) is unattainable from diet, so supplementation might be recommended [6].
Vitamin C consumption has been a common practice during cold or flu for decades, partly owing to research published by Linus Pauling in 1970 about RCTs regarding this subject [17]. More recent meta-analysis of several studies concluded that vitamin C low-dose supplementation does not decrease the risk of contracting a cold, but high doses exhibit other benefits, including a reduction in cold severity and symptoms, just as a reduction in duration and recovery time [18]. This vitamin also seems to provide a greater resistance to viral infections during exposure to physical and physiological stress, halving their incidence and conferring a prophylactic benefit [16][18]. The similarity of symptoms and the positive effect of ascorbic acid across a number of cold-related viruses has led to hypothesize that vitamin C’s activity is not virus-specific, and would, therefore, alleviate COVID-19 symptoms [4].
Vitamin C deficiency and its related disease scurvy have long been associated with increased susceptibility to pneumonia, which can be reversed by supplementation, with a particular benefit for individuals with lower dietary intakes [14]. This has been reported by different RCTs whose subjects significantly reduced pneumonia incidence when oral vitamin C was administered [19]. A decrease in the duration of hospital stay for those receiving earlier and higher doses of vitamin C has been reported [6].
Low oral bioavailability and downregulation of sodium-dependent vitamin C transporter 2 (SVCT2) by inflammatory cytokines led to the hypothesis that vitamin C therapeutic levels needed to mitigate oxidative stress in critically ill patients cannot be attainable through oral administration [8]. As for these individuals (suffering from burns, ARDS, sepsis, and septic shock), intravenous administration of ascorbic acid has been tested, and results highlight lower mortality according to meta-analysis [20]. These patients have higher vitamin C requirements than general population in order to normalize their blood levels, which have been seriously reduced by their pathology [9]. In the largest trial related to this research, the CITRIS-ALI trial, patients receiving a high dose of intravenous vitamin C did not appreciably ameliorate organ dysfunction scores, markers of inflammation, or vascular damage, though mortality rate was dramatically reduced. In addition, a reduction in intensive care unit (ICU) stay and mechanical ventilation was reported. This will conceivably improve long-term outcomes, especially if they keep on taking the vitamin orally after ICU discharge [8][21]. In spite of these positive results, the intravenous use of vitamin C should be performed cautiously, as in some cases and depending on dosage, it might exert a pro-oxidant effect rather than antioxidant [22].
Even though the evidence gathered so far about the specific utility of vitamin C against SARS-CoV-2 infection is limited, some related findings deserve to be highlighted. For instance, despite ascorbic acid, suboptimal intake poorly correlates with the disease incidence and correlates in an appreciable way with deaths [23]. Studies carried out in the USA and Spain showed a state of hypovitaminosis among COVID-19 patients with ARDS, which was even lower between non-survivors. It is also interesting that many risk factors for vitamin C deficiency overlap with those for COVID-19 (male; older; darker skin; patients suffering from hypertension, diabetes, or chronic obstructive pulmonary disease (COPD)) [4]. Vitamin C has been included in the treatment of some COVID-19 ICUs patients, which have shown to improve mortality rate. Intravenous administration of high doses in China and USA exhibited promising results in patients with moderate to severe disease, as it attenuated cytokine storm during the late stage of the infection, just as lung inflammation and injury [6][24]. In addition, there are some case reports of COVID-19 patients that described less mortality, mechanical ventilation need, and a decrease in inflammatory markers when using intravenous vitamin C [25].
Low ascorbic acid levels are frequent in COVID-19 critically ill patients (its body store is depleted due to oxidative stress, which leads to an increased physiological demand). This fact, along with all the findings presented before, suggest that vitamin C supplementation would be advisable to restore regular levels, in order to both prevent and treat these condition, as adequate status cannot be attainable through dietary sources [26][6]. The RDA of vitamin C for healthy adults is 75–90 mg/d. Owing to the lack of evidence on COVID-19, recommendations for vitamin C intake are limited. Doses of 1–2 g/d have previously been effective in preventing upper respiratory infections or reducing their duration. However, this does not apply when the patient is suffering the infection, as they need bigger doses in order to restore depleted levels. As mentioned before, individuals with serious disease would require even higher intravenous doses, about 50 mg/kg/6 h administered for 4 days. Association with polyphenols, flavonoids, and anthocyanins should be taken into consideration, as they could have an important role [16][26].
The potential benefits of this vitamin, including its low cost and safety profile, make it an attractive candidate and warrant its use. Some adverse effects have been reported in high dose administration cases, although they are of little consequence and related to patients with underlying conditions [16][9]. Patients at higher risk of COVID-19 mortality and vitamin C deficiency should take this recommendation more seriously, as they are the ones who can experiment the most severe outcomes, and at the same time, the ones who can benefit the most [4]. However, carefully designed RCTs are still needed in order to accurately assess the role of the vitamin in this disease before supplementation can be considered as a standard of care [16].
References
- Colunga Biancatelli, R.M.L.; Berrill, M.; Catravas, J.D.; Marik, P.E. Quercetin and Vitamin C: An Experimental, Synergistic Therapy for the Prevention and Treatment of SARS-CoV-2 Related Disease (COVID-19). Front. Immunol. 2020, 11, 1451.
- Laforge, M.; Elbim, C.; Frère, C.; Hémadi, M.; Massaad, C.; Nuss, P.; Benoliel, J.; Becker, C. Tissue damage from neutrophil-induced oxidative stress in COVID-19. Nat. Rev. Immunol. Nat. Res. 2020, 20, 515–516.
- Hemilä, H. Vitamin C and infections. Nutrients 2017, 9, 339.
- Holford, P.; Carr, A.C.; Jovic, T.H.; Ali, S.R.; Whitaker, I.S.; Marik, P.E.; Smith, D. Vitamin C—An adjunctive therapy for respiratory infection, sepsis and COVID-19. Nutrients 2020, 12, 3760.
- Erol, N.; Saglam, L.; Saglam, Y.S.; Erol, H.S.; Altun, S.; Aktas, M.S.; Halici, M. The Protection Potential of Antioxidant Vitamins against Acute Respiratory Distress Syndrome: A Rat Trial. Inflammation 2019, 42, 1585–1594.
- Abobaker, A.; Alzwi, A.; Alraied, A.H.A. Overview of the possible role of vitamin C in management of COVID-19. Pharmacol. Rep. 2020, 72, 1517–1528.
- Carr, A.C.; Maggini, S. Vitamin C and immune function. Nutrients 2017, 9, 1211.
- Kashiouris, M.G.; L’heureux, M.; Cable, C.A.; Fisher, B.J.; Leichtle, S.W.; Fowler, A.A. The emerging role of vitamin C as a treatment for sepsis. Nutrients 2020, 12, 292.
- Carr, A.C.; Rowe, S. The emerging role of vitamin c in the prevention and treatment of COVID-19. Nutrients 2020, 12, 3286.
- Mousavi, S.; Bereswill, S.; Heimesaat, M.M. Immunomodulatory and antimicrobial effects of vitamin C. Eur. J. Microbiol. Immunol. 2019, 9, 73–79.
- Calder, P.C. Nutrition, immunity and COVID-19. BMJ Nutr. Prev. Health 2020, 3, 74–92.
- Iddir, M.; Brito, A.; Dingeo, G.; Del Campo, S.S.F.; Samouda, H.; La Frano, M.R.; Bohn, T. Strengthening the immune system and reducing inflammation and oxidative stress through diet and nutrition: Considerations during the COVID-19 crisis. Nutrients 2020, 12, 1562.
- Barabutis, N.; Khangoora, V.; Marik, P.E.; Catravas, J.D. Hydrocortisone and Ascorbic Acid Synergistically Prevent and Repair Lipopolysaccharide-Induced Pulmonary Endothelial Barrier Dysfunction. Chest 2017, 152, 954–962.
- Allegra, A.; Tonacci, A.; Pioggia, G.; Musolino, C.; Gangemi, S. Vitamin deficiency as risk factor for SARS-CoV-2 infection: Correlation with susceptibility and prognosis. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 9721–9738.
- Kumar, V.; Kancharla, S.; Jena, M.K. In silico virtual screening-based study of nutraceuticals predicts the therapeutic potentials of folic acid and its derivatives against COVID-19. VirusDisease 2021, 32, 29–37.
- Jovic, T.H.; Ali, S.R.; Ibrahim, N.; Jessop, Z.M.; Tarassoli, S.P.; Dobbs, T.D.; Holford, P.; Holdford, P.; Thorton, C.; Whitaker, I. Could vitamins help in the fight against COVID-19? Nutrients 2020, 12, 2550.
- Pauling, L. Vitamin C and Common Cold. JAMA J. Am. Med Assoc. 1971, 216, 332.
- Hemilä, H.; Chalker, E. Vitamin C for preventing and treating the common cold. Cochrane Database Syst. Rev. 2013, 2013, CD000980.
- Hemilä, H.; Louhiala, P. Vitamin C for preventing and treating pneumonia. Cochrane Database Syst. Rev. 2013, 2013, CD005532.
- Carr, A.C. Vitamin C administration in the critically ill: A summary of recent meta-analyses. Crit. Care 2019, 23, 265.
- Fowler, A.A.; Truwit, J.D.; Hite, R.D.; Morris, P.E.; Dewilde, C.; Priday, A.; Fisher, B.; Thacker, L.; Natarajan, R.; Brophy, F.; et al. Effect of Vitamin C Infusion on Organ Failure and Biomarkers of Inflammation and Vascular Injury in Patients with Sepsis and Severe Acute Respiratory Failure: The CITRIS-ALI Randomized Clinical Trial. JAMA J. Am. Med Assoc. 2019, 322, 1261–1270.
- Oudemans-van Straaten, H.M.; Spoelstra-de Man, A.M.; de Waard, M.C. Vitamin C revisited. Crit. Care. 2014, 18, 460.
- Galmés, S.; Serra, F.; Palou, A. Current state of evidence: Influence of nutritional and nutrigenetic factors on immunity in the COVID-19 pandemic framework. Nutrients 2020, 12, 2738.
- Boretti, A.; Banik, B.K. Intravenous vitamin C for reduction of cytokines storm in acute respiratory distress syndrome. PharmaNutrition 2020, 18, 100190.
- Hiedra, R.; Lo, K.B.; Elbashabsheh, M.; Gul, F.; Wright, R.M.; Albano, J.; Azmaiparashvili, Z.; Aponte, G. The Use of IV vitamin C for patients with COVID-19: A single center observational study. Expert Rev. Anti Infect. Ther. 2020, 18, 1259–1261.
- Zabetakis, I.; Lordan, R.; Norton, C.; Tsoupras, A. COVID-19: The inflammation link and the role of nutrition in potential mitigation. Nutrients 2020, 12, 1466.
More
Information
Subjects:
Physiology
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
928
Entry Collection:
COVID-19
Revisions:
3 times
(View History)
Update Date:
10 Jan 2022
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No