 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | María Teresa Nestares | + 2668 word(s) | 2668 | 2021-08-11 05:08:26 | | | |
| 2 | Peter Tang | Meta information modification | 2668 | 2021-11-12 10:42:21 | | |
Video Upload Options
Celiac disease (CD) is a multisystemic disorder with different clinical expressions, from malabsorption with diarrhea, anemia, and nutritional compromise to extraintestinal manifestations. Anemia might be the only clinical expression of the disease, and iron deficiency anemia is considered one of the most frequent extraintestinal clinical manifestations of CD. Therefore, CD should be suspected in the presence of anemia without a known etiology. Assessment of tissue anti-transglutaminase and anti-endomysial antibodies are indicated in these cases and, if positive, digestive endoscopy and intestinal biopsy should be performed. Anemia in CD has a multifactorial pathogenesis and, although it is frequently a consequence of iron deficiency, it can be caused by deficiencies of folate or vitamin B12, or by blood loss or by its association with inflammatory bowel disease (IBD) or other associated diseases.
1. Introduction
|
Cause |
Incidence |
|---|---|
|
Iron deficiency |
12–69% (adults) 10–20% (children) |
|
Folic acid deficiency |
20–30% |
|
Vitamin B12 deficiency |
8–41% |
|
Copper deficiency |
Very low |
|
Zinc deficiency |
Very low * |
|
Bad response to the gluten-free diet |
23% |
|
Medullary aplasia |
Very low (12 cases) |
|
Chronic disease |
4–17% |
2. Micronutrient Deficiencies and Celiac Disease
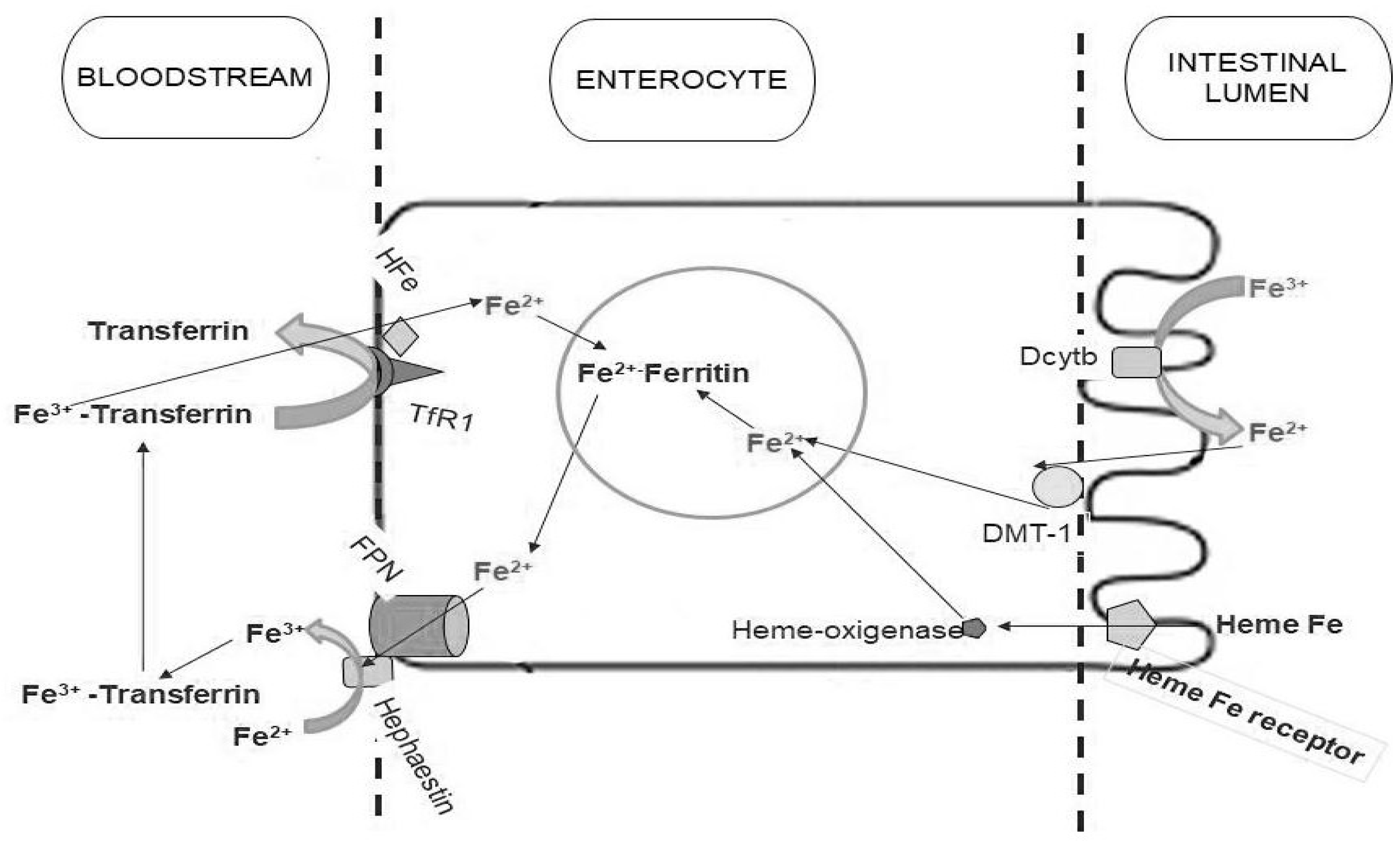
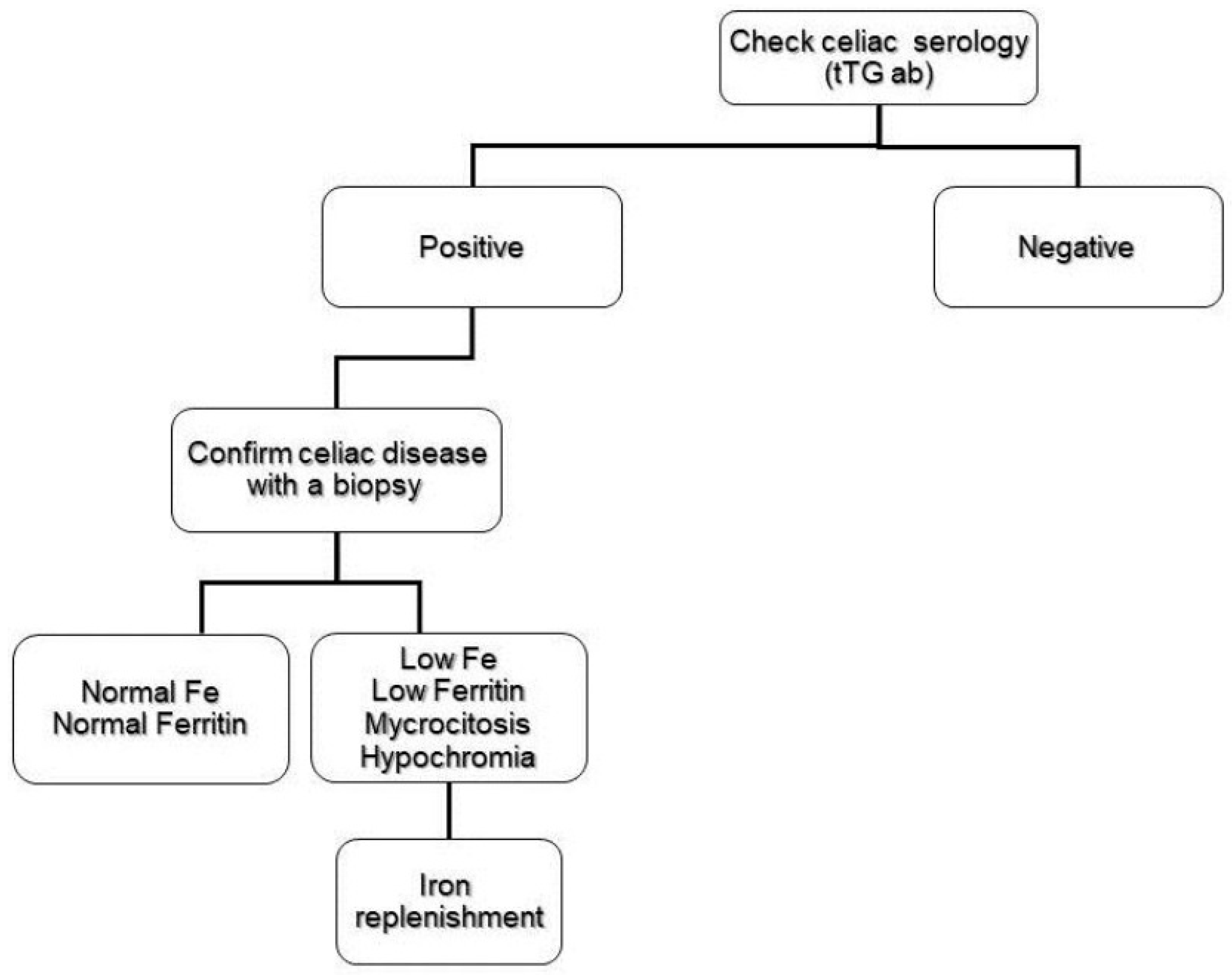
2.1. Iron Deficiency
2.2. Folate and Vitamin B12 Deficiency
2.3. Copper and Zinc Deficiency
3. Refractory Anemia to the Gluten-Free Diet
References
- Rubio-Tapia, A.; Ludvigsson, J.F.; Brantner, T.L.; Murray, J.A.; Everhart, J.E. The Prevalence of Celiac Disease in the United States. Am. J. Gastroenterol. 2012, 107, 1538–1544.
- Larson, S.A.; Khaleghi, S.; Rubio-Tapia, A.; Ovsyannikova, I.G.; King, K.S.; Larson, J.J.; Lahr, B.D.; Poland, G.A.; Camilleri, M.J.; Murray, J.A. Prevalence and Morbidity of Undiagnosed Celiac Disease from a Community-Based Study. Gastroenterology 2017, 152, 830–839.
- Mahadev, S.; Laszkowska, M.; Sundström, J.; Björkholm, M.; Lebwohl, B.; Green, P.H.; Ludvigsson, J.F. Prevalence of Celiac Disease in Patients With Iron Deficiency Anemia—A Systematic Review with Meta-analysis. Gastroenterology 2018, 155, 374–382.
- Guandalini, S.; Assiri, A. Celiac disease: A review. JAMA Pediatr. 2014, 168, 272–278.
- Husby, S.; Koletzko, S.; Korponay-Szabo, I.R.; Mearin, M.L.; Phillips, A.; Shamir, R.; Troncone, R.; Giersiepen, K.; Branski, D.; Catassi, C.; et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 136–160.
- Felli, C.; Balsassarre, A.; Masoptti, A. Intestinal and circulating microRNAs in coeliac disease. Int. J. Mol. Sci. 2017, 18, 1907.
- Amr, K.S.; Bayoumi, F.S.; Eissa, E.; Abu-Zekry, M. Circulating microRNAs as potential non-invasive biomarkers in pediatric patients with celiac disease. Eur. Ann. Allergy Clin. Immunol. 2019, 51, 159–164.
- Vaira, V.; Roncoroni, L.; Barisani, D.; Gaudioso, G.; Bosari, S.; Bulfamante, G.; Doneda, L.; Conte, D.; Tomba, C.; Bardella, M.T.; et al. MicroRNA profiles in coeliac patients distinguish different clinical phenotypes and are modulated by gliadin peptides in primary duodenal fibroblast. Clin. Sci. 2014, 126, 417–423.
- Bledsoe, A.C.; King, K.S.; Larson, J.J.; Snyder, M.; Absah, I.; Murray, J.A. Micronutrient Deficiencies Are Common in Contemporary Celiac Disease Despite Lack of Overt Malabsorption Symptoms. Mayo Clin. Proc. 2019, 94, 1253–1260.
- Halfdanarson, T.R.; Litzow, M.R.; Murray, J.A. Hematologic manifestations of celiac disease. Blood 2007, 109, 412–421.
- Shahriari, M.; Honar, N.; Yousefi, A.; Javaherizadeh, H. Association of potential celiac disease and refractory iron deficiency anemia in children and adolescents. Arq. Gastroenterol. 2018, 55, 78–81.
- Elli, L.; Norsa, L.; Zullo, A.; Carroccio, A.; Girelli, C.; Oliva, S.; Romano, C.; Leandro, G.; Bellini, M.; Marmo, R.; et al. Diagnosis of chronic anaemia in gastrointestinal disorders: A guideline by the Italian Association of Hospital Gastroenterologist and Endoscopist (AIGO) and the Italian Society of Pardiatric Gastroenterology Hepatology and Nutrition (SIGENP). Dig. Liver Dis. 2019, 51, 471–483.
- Murray, J.A.; Watson, T.; Clearman, B.; Mitros, F. Effect of a gluten-free diet on gastrointestinal symptoms in celiac disease. Am. J. Clin. Nutr. 2004, 79, 669–673.
- Leffler, D.A.; Dennis, M.; Hyett, B.; Kelly, E.; Schuppan, D.; Kelly, C.P. Etiologies and Predictors of Diagnosis in Nonresponsive Celiac Disease. Clin. Gastroenterol. Hepatol. 2007, 5, 445–450.
- Muñoz, M.; Villar, I.; García-Erce, J.A. An update on iron physiology. World J. Gastroenterol. 2009, 15, 4617.
- DeLoughery, T.G. Microcytic anemia. N. Engl. J. Med. 2014, 371, 1324–1331.
- Leung, A.K.; Chan, K.W. Iron deficiency anemia. Adv. Pediatr. 2001, 48, 385–408.
- Rao, R.; Georgieff, M.K. Iron in fetal and neonatal nutrition. Semin. Fetal Neonatal Med. 2007, 12, 54–63.
- Beard, J. Iron Deficiency Alters Brain Development and Functioning. J. Nutr. 2003, 133, 1468S–1472S.
- Beard, J.L.; Wiesinger, J.A.; Connor, J.R. Pre- and Postweaning Iron Deficiency Alters Myelination in Sprague-Dawley Rats. Dev. Neurosci. 2003, 25, 308–315.
- Beard, J.L.; Connor, J.R. Iron status and neural functioning. Annu. Rev. Nutr. 2003, 23, 41–58.
- Rubio-Tapia, A.; Hill, I.D.; Kelly, C.P.; Calderwood, A.H.; Murray, J.A. ACG Clinical Guidelines: Diagnosis and Management of Celiac Disease. Am. J. Gastroenterol. 2013, 108, 656–676.
- Harper, J.W.; Holleran, S.F.; Ramakrishnan, R.; Bhagat, G.; Green, P.H.R. Anemia in celiac disease is multifactorial in etiology. Am. J. Hematol. 2007, 82, 996–1000.
- Annibale, B.; Severi, C.; Chistolini, A.; Antonelli, G.; Lahner, E.; Marcheggiano, A.; Iannoni, C.; Monarca, B.; Delle Fave, G. Efficacy of gluten-free diet alone on recovery from iron deficiency anemia in adult celiac patients. Am. J. Gastroenterol. 2001, 96, 132–137.
- Smukalla, S.; Lebwohl, B.; Mears, J.G.; Leslie, L.A.; Green, P.H. How often do hematologists consider celiac disease in iron-deficiency anemia? Results of a national survey. Clin. Adv. Hematol. Oncol. 2014, 12, 100–105.
- Oxentenko, A.S.; Murray, J.A. Celiac Disease: Ten Things That Every Gastroenterologist Should Know. Clin. Gastroenterol. Hepatol. 2015, 13, 1396–1404.
- Murray, J.A.; McLachlan, S.; Adams, P.C.; Eckfeldt, J.H.; Garner, C.P.; Vulpe, C.D.; Gordeuk, V.R.; Brantner, T.; Leiendecker–Foster, C.; Killeen, A.A.; et al. Association between celiac disease and iron deficiency in caucasians, but not non-caucasians. Clin. Gastroenterol. Hepatol. 2013, 11, 808–814.
- Pirán Arce, M.F.; Aballay, L.R.; Leporati, J.L.; Navarro, A.; Forneris, M. Blood iron levels in accordance with adherence to a gluten-free diet in celiac school aged children. Nutr. Hosp. 2018, 35, 25–32.
- Sharma, N.; Begum, J.; Eksteen, B.; Elagib, A.; Brookes, M.; Cooper, B.T.; Tselepis, C.; Iqbal, T.H. Differential ferritin expression is associated with iron defficiency in coeliac disease. Eur. J. Gastroenterol. Hepatol. 2009, 21, 794–804.
- Zamani, F.; Mohamadnejad, M.; Shakeri, R.; Amiri, A.; Najafi, S.; Alimohamadi, S.M.; Tavangar, S.M.; Ghavamzadeh, A.; Malekzadeh, R. Gluten sensitive enteropathy in patients with iron deficiency anemia of unknown origin. World J. Gastroenterol. 2008, 14, 7381.
- Lasa, J.S.; Olivera, P.; Soifer, L.; Moore, R. La anemia ferropénica como presentación de enfermedad celíaca subclínica en una población argentina. Rev. Gastroenterol. Méx. 2017, 82, 270–273.
- Repo, M.; Lindfors, K.; Mäki, M.; Huhtala, H.; Laurila, K.; Lähdeaho, M.L.; Saavalainen, P.; Kaukinen, K.; Kurppa, K. Anemia and iron deficiency in children with potential celiac disease. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 56–62.
- Dinler, G.; Atalay, E.; Kalayci, A.G. Celiac disease in 87 children with typical and atypical symptoms in Black Sea region of Turkey. World J. Pediatr. 2009, 5, 282–286.
- Wierdsma, N.; van Bokhorst-de van der Schueren, M.; Berkenpas, M.; Mulder, C.; van Bodegraven, A. Vitamin and Mineral Deficiencies Are Highly Prevalent in Newly Diagnosed Celiac Disease Patients. Nutrients 2013, 5, 3975–3992.
- García-Manzanares, Á.; Lucendo, A.J. Review: Nutritional and Dietary Aspects of Celiac Disease. Nutr. Clin. Pract. 2011, 26, 163–173.
- Carmel, R. Megaloblastic Anemias: Disorders Ofimpaired DNA Synthesis, 1st ed.; Wintrobe’s Clinical Hematology; Williams & Wilkins: Baltimore, MD, USA, 2004.
- Kuloğlu, Z.; Kirsaçlioğlu, C.T.; Kansu, A.; Ensari, A.; Girgin, N. Celiac disease: Presentation of 109 children. Yonsei Med. J. 2009, 50, 617–623.
- Ward, P.C.J. Modern approaches to the investigation of vitamin B12 deficiency. Clin. Lab. Med. 2002, 22, 435–445.
- Klee, G.G. Cobalamin and folate evaluation: Measurement of methylmalonic acid and homocysteine vs vitamin B(12) and folate. Clin. Chem. 2000, 46, 1277–1283.
- Guevara Pacheco, G.; Chávez Cortés, E.; Castillo-Durán, C. Deficiencia de micronutrientes y enfermedad celíaca. Arch. Argent Pediatr. 2014, 112, 457–463.
- Freeman, H.J. Neurological disorders in adult celiac disease. Can. J. Gastroenterol. 2008, 22, 909–911.
- Halfdanarion, T.R.; Kumar, N.; Hogan, W.J.; Murray, J.A. Copper deficiency in celiac disease. J. Clin. Gastroenterol. 2009, 43, 162–164.
- Cavallieri, F.; Fin, N.; Contardi, S.; Fiorini, M.; Corradini, E.; Valzania, F. Subacute copper-deficiency myelopathy in as patient with occult celiac disease. J. Spinal Cord Med. 2017, 40, 489–491.
- Tran, C.D.; Katsikeros, R.; Manton, N.; Krebs, N.F.; Hambidge, K.M.; Butler, R.N.; Davidson, G.P. Zinc homeostasis and gut function in children with celiac disease. Am. J. Clin. Nutr. 2011, 94, 1026–1032.
- Berry, N.; Basha, J.; Varma, N.; Varma, S.; Prasad, K.K.; Vaiphei, K.; Dhaka, N.; Sinha, S.K.; Kochhar, R. Anemia in celiac disease is multifactorial in etiology: A prospective study from India. JGH Open 2018, 2, 196–200.
- Elli, L.; Ferretti, F.; Orlando, S.; Vecchi, M.; Monguzzi, E.; Roncoroni, L.; Schuppan, D. Management of celiac disease in daily clinical practice. Eur. J. Intern. Med. 2019, 61, 15–24.
- Barratt, S.M.; Leeds, J.S.; Sanders, D.S. Quality of life in Coeliac Disease is determined by perceived degree of difficulty adhering to a gluten-free diet, not the level of dietary adherence ultimately achieved. J. Gastrointestin Liver Dis. 2011, 20, 241–245.
- Martín Masot, R.; Ortega Páez, E. El péptido del gluten en heces puede ser útil en el seguimiento de la enfermedad celíaca. Evid. Pediatr. 2018, 14, 37.
- Silvester, J.A.; Kurada, S.; Szwajcer, A.; Kelly, C.P.; Leffler, D.A.; Duerksen, D.R. Tests for Serum Transglutaminase and Endomysial Antibodies Do Not Detect Most Patients with Celiac Disease and Persistent Villous Atrophy on Gluten-free Diets: A Meta-analysis. Gastroenterology 2017, 153, 689–701.
- Gerasimidis, K.; Zafeiropoulou, K.; Mackinder, M.; Ijaz, U.Z.; Duncan, H.; Buchanan, E.; Cardigan, T.; Edwards, C.A.; McGrogan, P.; Russell, R.K. Comparison of Clinical Methods With the Faecal Gluten Immunogenic Peptide to Assess Gluten Intake in Coeliac Disease. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 356–360.
- Rubio-Tapia, A.; Murray, J.A. Classification and management of refractory coeliac disease. Gut 2010, 59, 547–557.
- van Gils, T.; Nijeboer, P.; van Wanrooij, R.L.; Bouma, G.; Mulder, C.J.J. Mechanisms and management of refractory coeliac disease. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 572–579.
- Ryan, B.M.; Kelleher, D. Refractory celiac disease. Gastroenterology 2000, 119, 243–251.
- Rishi, A.R.; Rubio-Tapia, A.; Murray, J.A. Refractory celiac disease. Expert Rev. Gastroenterol. Hepatol. 2016, 10, 537–546.
- Mooney, P.D.; Evans, K.E.; Singh, S.; Sanders, D.S. Treatment failure in coeliac disease: A practical guide to investigation and treatment of non-responsive and refractory coeliac disease. J. Gastrointestin Liver Dis. 2012, 21, 197–203.
- Delabie, J.; Holte, H.; Vose, J.M.; Ullrich, F.; Jaffe, E.S.; Savage, K.J.; Connors, J.M.; Rimsza, L.; Harris, N.L.; Müller-Hermelink, K.; et al. Enteropathy-associated T-cell lymphoma: Clinical and histological findings from the international peripheral T-cell lymphoma project. Blood 2011, 118, 148–155.

