Celiac disease (CD) is a multisystemic disorder with different clinical expressions, from malabsorption with diarrhea, anemia, and nutritional compromise to extraintestinal manifestations. Anemia might be the only clinical expression of the disease, and iron deficiency anemia is considered one of the most frequent extraintestinal clinical manifestations of CD. Therefore, CD should be suspected in the presence of anemia without a known etiology. Assessment of tissue anti-transglutaminase and anti-endomysial antibodies are indicated in these cases and, if positive, digestive endoscopy and intestinal biopsy should be performed. Anemia in CD has a multifactorial pathogenesis and, although it is frequently a consequence of iron deficiency, it can be caused by deficiencies of folate or vitamin B12, or by blood loss or by its association with inflammatory bowel disease (IBD) or other associated diseases.
1. Introduction
Celiac disease (CD) is one of the most frequent genetic diseases, affecting 1% of the world population. Diagnosed cases are increasing and it seems to be due to the actual increase in the incidence rather than due to the advancement of diagnostic methods or to the larger awareness of the disease among the lay population [
1,
2].
Celiac disease is a systemic disorder, caused by an immune reaction activated by the ingestion of gluten and related proteins occurring in individuals carrying haplotypes of major histocompatibility antigen (HLA) class II: more than 90% of celiac patients are HLA-DQ2 haplotype positive, and almost all of the remaining patients carry HLA-DQ8. Exposure to gluten has a double effect, triggering both innate and adaptive immune responses, with symptoms at the intestinal and extra-intestinal levels [
3]. The contact of the intestinal mucosa with gluten leads to a characteristic histological lesion, although not pathognomonic. Their typical histological features are an increase in intraepithelial lymphocytes, villous atrophy, crypt hyperplasia, and infiltration of inflammatory cells in the lamina propria.
Diagnosis of CD is conducted by combining serological screening tests (anti-tissue-transglutaminase and anti-endomysial IgA antibodies) and an intestinal biopsy [
4]. The duodenal biopsy can be avoided [
5] in adolescents and children with symptoms or signs of CD and with high anti-tissue-transglutaminase antibody levels, positivity for anti-endomysial antibodies, and presence of HLA DQ21 or HLA-DQ8 heterodimer.
Recent reports have demonstrated that specific miRNAs are modulated in duodenal mucosa affected by CD. The miRNAs dysregulated during the development of CD could be potentially involved in the pathogenesis of CD [
6]. Overexpression or downregulation of several miRNAs could potentially stimulate or inhibit pathways related to the pathogenesis of CD. A study has demonstrated the regulation of circulating miRNA-21 and miRNA-31 expression levels in children with CD and showed that miR-21 expression level was positively correlated with the anti-tissue-transglutaminase IgA antibodies [
7]. This correlation may indicate that the altered expression of the circulating miRNAs could be used as potential non-invasive diagnostic and prognostic biomarkers for CD patients. In addition, Vaira et al. [
8] have shown the downregulation of miR-194-5p and the overexpression of miR-638 in celiac patients with anemia compared with celiac patients with classical symptoms.
Patients with CD could feature various deficiency states, leading to anemia and bone mass loss and a wide range of digestive and extra-digestive symptoms. Upon diagnosis, nutritional deficiencies were found in vitamins and minerals; patients should be tested for micronutrient deficiencies, in particular iron, folic acid, vitamin B
12, vitamin D, copper, and zinc. Celiac disease is a cause of anemia, usually due to the malabsorption of iron, folic acid, and vitamin B
12 [
9]. Anemia is mainly due to the fact of iron deficiency as a consequence of iron malabsorption. Iron malabsorption is usually observed in CD, being considered a clinical diagnostic feature of CD even in subjects not presenting the classic digestive symptoms. Iron deficiency anemia (IDA) is a frequent finding in patients with overt CD (10–20% of cases) [
10], despite the fact that they are consuming iron supplements. A recent meta-analysis found that more than 3% of patients with IDA have histological evidence of CD. This high percentage of subjects with IDA who are celiac, reinforces the need for screening CD in patients with IDA [
11]. Folate and vitamin B
12 malabsorption, nutritional deficiencies, blood loss, inflammation, development of refractory CD or concomitant
Helicobacter pylori infection are other causes of anemia in such patients [
12] (
Table 1).
Table 1. Etiology of anemia in celiac disease.
|
Cause
|
Incidence
|
|
Iron deficiency
|
12–69% (adults)
10–20% (children)
|
|
Folic acid deficiency
|
20–30%
|
|
Vitamin B12 deficiency
|
8–41%
|
|
Copper deficiency
|
Very low
|
|
Zinc deficiency
|
Very low *
|
|
Bad response to the gluten-free diet
|
23%
|
|
Medullary aplasia
|
Very low (12 cases)
|
|
Chronic disease
|
4–17%
|
* It has been reported that 50% of celiac patients have low serum levels at diagnosis, but it has not been related to celiac disease (CD).
The mainstay of treatment for CD remains adherence to a gluten-free diet (GFD). In the vast majority of cases, strict monitoring of GFD leads to the disappearance of clinical symptoms and serological signs, the recovery of normal histology in the duodenum and the prevention of complications derived from CD [
13]. However, in approximately 20% of celiac patients, symptoms persist despite excluding gluten from their diet [
14].
2. Micronutrient Deficiencies and Celiac Disease
2.1. Iron Deficiency
Iron is an essential micronutrient, it is required for adequate erythropoietic function, oxidative metabolism, enzymatic activities, and cellular immune responses [
15]. IDA is a major public health problem. Iron deficiency anemia occurs when iron loss and body’s requirement for iron are not met by dietary sources, therefore the iron storage of the organism is depleted. This pathological process is characterized by the production of smaller red cells because the concentration of hemoglobin (Hb) is abnormally low [
15]. Iron deficiency anemia results in fatigue and diminished muscular oxygenation, which may affect muscle strength and quality and, subsequently, physical performance [
16]. Celiac disease constitutes one of the groups at highest risk of iron deficiency (ID) [
17]. Iron requirements exceed iron intake at some time points throughout life: the first 6–18 months of life and then, for women, during adolescence and all fertile period. Iron deficiency during the first year of life occurs at a time point of rapid neural development and when morphological, biochemical, and bioenergetic alterations may all influence future functioning [
18]. The brain is the most vulnerable organ during critical periods of development [
19]. Iron is present in the brain from very early in life, when it participates in the neural myelination processes [
20], learning, and interacting behaviors, and iron is needed by enzymes involved in the synthesis of serotonin and dopamine neurotransmitters [
21].
The most common causes of ID are blood loss and failure of the enterocytes of the proximal intestine to uptake iron from the diet in patients who have enough dietary iron. Celiac disease leads to an abnormal immune response, which is followed by a chronic inflammation of the small intestinal mucosa with progressive disappearance of intestinal villi [
22] leading to a decrease in absorption of many nutrients, including iron [
23,
24]. Unfortunately, this interesting association between CD and IDA has been poorly appreciated [
25] in spite of the great interest of micronutrient deficiency as a diagnostic clue in asymptomatic CD, especially for iron and IDA [
26].
Celiac disease is an increasingly recognized disorder in Caucasian populations of European origin. Murray et al. [
27] analyzed HLA genotypes and frequencies of CD between Caucasians and non-Caucasians with ID. The results showed that CD is associated with ID in Caucasians, but CD is rare among non-Caucasians—even among individuals with features of CD, such as ID. Pirán Arce et al. [
28] evaluated the nutritional status of iron in 44 celiac children by determining biochemical parameters and their relationship with the intake of this mineral and adherence to the GFD. These authors concluded that under conditions of adequate iron consumption, iron status is related to the degree of adherence to the GFD. Although GFD is an effective treatment for CD, IDA remains an occasional finding during follow-up and correlates to inadequate gluten exclusion [
10].
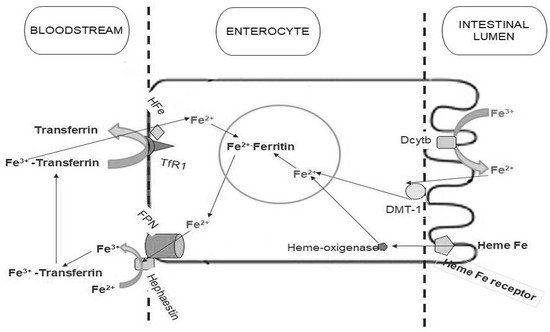
Iron enters the enterocytes through an apical divalent metal transporter (DMT-1) (
Figure 1). Sharma et al. [
35] have evaluated iron regulatory proteins in celiac patients compared to controls and iron deficient patients using duodenal biopsies. The results showed that DMT-1, ferroportin, hephaestin, and transferrin receptor protein mRNA increased, primarily due to the fact of iron deficiency, while body iron stores were reduced in CD. In contrast, these authors [
35] showed that expression of DMT1 and ferroportin are increased in CD patients with or without ID. In this study, ferritin expression was also found to be increased in CD, but only in those with ID.
Figure 1. Iron absorption metabolism. Non-heme iron is ultimately taken up from the lumen by divalent metal transporter (DMT-1) on the microvillus membrane, before joining the labile iron pool in the cell. Ferric iron has to be reduced to the ferrous form by duodenal cytochrome b (Dcytb) before the uptake. Ferrous iron in the labile iron pool is then transferred to the circulation by ferroportin (FPN), which requires hephaestin for oxidation to the ferric form to bind transferrin. Heme iron is taken up by a specific receptor. Internalized heme iron is degraded by heme-oxygenase, releasing non-heme iron. The non-heme iron is then transported to the cytoplasm, joining the labile iron pool and is then transferred to the bloodstream by FPN in the same manner as non-heme iron.
The prevalence of CD in subjects presenting IDA has been described by other authors [
39,
40,
41] with different results, due to the probable differences in the study of the designs. Lasa et al. [
40] designed a study to avoid the abovementioned bias. They decided to evaluate all patients diagnosed with IDA by performing upper endoscopy and duodenal biopsies, and not only those with positive antibodies or with IDA of unknown origin (after an extensive work-up). Patients with IDA have an increased risk for CD, up to 25% of these patients may not present any endoscopic sign suggesting villous atrophy [
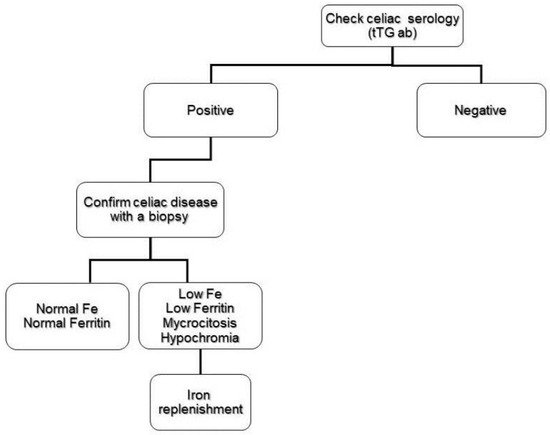
39]. This finding makes routine duodenal biopsy necessary when performing upper endoscopy on IDA patients. In a systematic review and meta-analysis, Mahadev et al. [
3] found that approximately 1 out of 31 patients with IDA have histologic evidence of CD; this prevalence value justifies the screening of patients with IDA for CD (
Figure 2).
Figure 2. Abbreviated flow chart of the investigation of iron deficiency anemia in celiac disease patients.
2.2. Folate and Vitamin B12 Deficiency
Usually, people suffering from CD can develop folate and vitamin B12 deficiencies as a result of generalized malabsorption linked to villi atrophy. Both vitamins are essential for normal hematopoiesis and neurologic function.
Folate absorption occurs primarily in the jejunum, which is commonly affected by CD [
10,
42]. Several studies in adult celiac patients have shown an increased risk of folate deficiency, which can reach up to 20–30% of newly diagnosed patients [
43,
44]. Prior to uptake, folate must be deconjugated by a brush border membrane peptidase and the intestinal mucosa damage in CD may affect enzyme activity leading to a folate deficiency. Serum and red cell folate measurements are usually used for the diagnosis of folate deficiency. Serum folate levels reflect largely folate intake and it is common for levels to be high in patients with a vitamin B
12 deficiency. Red cell folate is not a specific indicator for folate deficiency, as it can be decreased in patients with vitamin B
12, but red cell folate levels are less influenced by variations in folate intake. Patients with CD commonly have elevated levels of homocysteine which may serve as an important clue for the diagnosis. However, the sensitivity of this measurement is somewhat less for vitamin B
12 deficiency [
45].
Vitamin B
12 requires formation of a primary complex with intrinsic factor to be absorbed in the proximal small intestine, and small amounts may also be absorbed by passive transport throughout the entire intestine. Deficiency of vitamin B
12 is common in CD and frequently results in anemia. Though the terminal ileum is the primary site of absorption of vitamin B
12, García-Manzanares and Lucendo [
44] reported a prevalence of vitamin B
12 deficiency between 8% and 41% in patients with newly diagnosed CD.
The causes of B
12 deficiency in CD are still not clear, but they may be related to complications of small intestinal injury including a decreased gastric acidity, cobalamin intake due to the frequent finding of bacterial overgrowth, autoimmune gastritis, and decreased efficiency of the intrinsic factor or even dysfunction of the distal small intestine. Abnormalities in the absorption of folate or vitamin B
12 may result in anemia in children with untreated CD. The range of low folate and low vitamin B
12 prevalence were 15.7–18.3% and 4.3–8%, respectively [
42,
46].
Both folate and vitamin B
12 deficiencies can lead to a macrocytic anemia with low values for hemoglobin or hematocrit, and high mean corpuscular volume levels. Vitamin B
12 deficiency should be considered in patients with CD and hematological and neurological disorders [
47]. Vitamin B
12 levels measured within the lower range of normal or if they coexist with folic acid deficiency can be misleading and difficult to interpret. Under these circumstances, high serum levels of methylmalonic acid may improve the diagnostic accuracy of vitamin B
12 deficiency [
48].
2.3. Copper and Zinc Deficiency
Micronutrient deficiencies are common in celiac patients. In addition to the abovementioned deficiencies (i.e., iron, folic acid, and vitamin B
12), at the time of diagnosis there may be deficiencies for other vitamins and minerals, in particular copper and zinc [
22].
Copper deficiency is a rare complication in CD and its prevalence remains unknown. This deficiency can lead to anemia, thrombocytopenia, neutropenia, and peripheral neuronal involvement. In adult celiac patients, peripheral myeloneuropathy has been described along with hypocupremia with a good clinical response to copper supplementation [
49,
50]. Halfdanarion et al. [
51] reported five cases of adult celiac patients with copper deficiency; all of them presented neurological complications and three of them presented hematological abnormalities. Cavallieri et al. [
52] recently described a rare case of myelopathy induced by copper deficiency secondary to undiagnosed CD, and they have suggested that patients with hypocupremia should be tested for CD.
Likewise, the presence of clinical alterations as a consequence of zinc deficiency is also uncommon in celiac patients. Fractional zinc absorption is no different between celiac patients and controls, but the rapid zinc exchange body compartment is lower in CD than in control patients [
49]. The mechanism of zinc depletion and its possible implications are unknown [
53].
3. Refractory Anemia to the Gluten-Free Diet
The etiology of persistent refractory anemia is multiple, and it must first be ruled out that it is due to the poor adherence to a GFD. Other causes of refractory anemia are chronic inflammation or anemia of chronic disorders, refractory celiac disease (RCD), the higher prevalence of the disease than expected by the involvement of other intestinal sections or the appearance of other comorbidities [
77].
The first suggested finding is that it is a false refractoriness or persistence of anemia because the adherence to the treatment is not being conducted correctly. GFD is not easy to comply with nor is it generally well performed [
78]. The traditional methods used to monitor the disease have poor performance, because, for example, with the serological method, for every six examinations we would detect the transgression in only one of them [
79], besides presenting little correlation with villus atrophy [
80]. The immunogenic gluten peptide in feces is postulated as a better tool for assessing diet adherence [
81].
Celiac disease responds in the majority of patients on a GFD in a few weeks [
13]. However, despite the correct adherence to a GFD, villous atrophy, malabsorption, and chronic intestinal inflammation persist in some patients for 12 months, which defines the RCD [
82,
83,
84]. This can lead to persistence of symptoms and signs, including anemia. RCD is considered a rarity in pediatric age and, although its exact prevalence and incidence in adulthood is unknown, it is an uncommon condition [
85]. Due to the poor response of the disease to treatment at this stage and its prognosis, it is important to correctly make the diagnosis [
86], which is considered exclusion. The complete histological evaluation of the entire small intestine is needed for the diagnosis of refractoriness or complications [
87].
The presence of other comorbidities, not always associated with CD itself, are linked to persistent symptoms once adherence to the GFD has been verified, such as microscopic colitis, irritable bowel syndrome, food allergies, motility disorders or collagen sprinkles [
85]. The sprue collagen manifests itself in the form of refractoriness, and its occasional association with EATL has also been described [
97]. The diagnosis is performed by biopsy and pathological analysis.
This entry is adapted from the peer-reviewed paper 10.3390/nu11112557