 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Borvornwut Buranawat | + 1219 word(s) | 1219 | 2021-10-22 09:04:01 | | | |
| 2 | Jessie Wu | Meta information modification | 1219 | 2021-11-03 06:49:39 | | | | |
| 3 | Jessie Wu | Meta information modification | 1219 | 2021-11-03 06:50:21 | | |
Video Upload Options
This study presents an overview of the biomechanical and biomolecular aspects of various attachments for implant overdenture. We focused on the following topics: attachment systems, retention of various attachments, stress distribution with different attachments, the design and fabrication of attachments, digital techniques in overdenture attachments, and the effects of attachments in peri-implant health. We found that plastic resin is commonly used for ball and bar attachments, whereas nylon resin is commonly used in locator attachments. The locator system offers a valuable attachment option for implant-retained overdenture. Attachment retention reduces while lateral force increases with implant inclination in overdenture. The higher the retention of an overdenture attachment, the higher the transferred stresses. Additionally, clip loading produces more stress in implants and precision elements than bar-retained dentures. As such, we conclude that the ball and locator systems the best overdenture systems due to their superior tissue response, survival rate, and patient satisfaction.
1. Introduction
2. Effects of Attachment Types on Implant Overdenture
| Attachment Type | Advantages | Disadvantages | Reference |
|---|---|---|---|
| Ball attachment (O-ring attachment) |
Simple manufacturing process, the provision of a wide range of movement, cost-effectiveness, ease of use, good retention, easy hygiene maintenance, and high patient satisfaction. | The abutment requires implants to be parallelly placed, and the loss of parallelism may cause difficulty while inserting and removing the prosthesis or during the fracturing of the abutment. The O-ring needs to be regularly changed because it is subject to wear. | [6][7] |
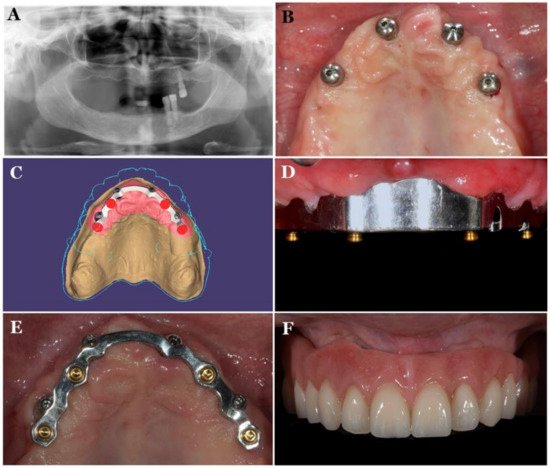
| Bar attachment | Provides retention, implant splinting, and wide-ranging load distribution that results in a movement reduction of the implants. | Technique-sensitive, expensive, and present difficult hygiene maintenance under the bars, leading to mucosal swelling or gingival hyperplasia. Bars are not indicated in a V-shaped ridge because this leads to the infringement of tongue space. | [8][9] |
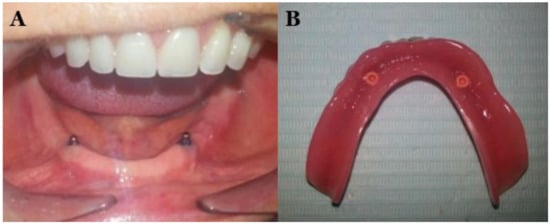
| Locators | Locators are popular attachments for implant-retained or implant-supported overdenture because of their low level of thickness (2.5 mm height) and ability to self-align, which can correct up to 40° of implant angulations. They can be used in narrow inter-arch space. Locators offer excellent retention and stability, and they allow for easy hygiene maintenance. The telescopic attachment, which offers a self-seating mechanism, is suitable for patients with reduced manual dexterity, such as those with Parkinson’s disease. | Periodic replacement of the male nylon component is required. Some prosthetic complications such as locator attachments, periodic repair, and higher maintenance double-crown locator attachments require sufficient inter-arch space and the metal display of attachments. | [10][11][12][13][14] |
| Magnetic attachments | Magnetic attachments reduce the transfer of horizontal stress to the implants and bone during the insertion and removal of the denture. | These are low-profile attachments; however, corrosion and loss of magnetism are significant complications associated with their usage. | [15][16][17][18] |
References
- Vi, S.; Pham, D.; Du, Y.Y.M.; Arora, H.; Tadakamadla, S.K. Mini-implant-retained overdentures for the rehabilitation of completely edentulous maxillae: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 4377.
- Aldhohrah, T.; Mashrah, M.A.; Wang, Y. Effect of 2-implant mandibular overdenture with different attachments and loading protocols on peri-implant health and prosthetic complications: A systematic review and network meta-analysis. J. Prosthet. Dent. 2021, in press.
- Ceraulo, S.; Leonida, A.; Lauritano, D.; Baldoni, A.; Longoni, S.; Baldoni, M.; Caccianiga, G. Proposal for a clinical approach to geriatric patients with anchor need on implant for removable denture: New technique. Prosthesis 2020, 2, 185–195.
- Amornvit, P.; Rokaya, D.; Bajracharya, S.; Keawcharoen, K.; Supavanich, W. Management of obstructive sleep apnea with implant retained mandibular advancement device. World J. Dent. 2014, 5, 184–189.
- Daou, E.E. Stud attachments for the mandibular implant-retained overdentures: Prosthetic complications. A literature review. Saudi Dent. J. 2013, 25, 53–60.
- Winkler, S.; Piermatti, J.; Rothman, A.; Siamos, G. An overview of the o-ring implant overdenture attachment: Clinical reports. Oral Implant. 2002, 28, 82–86.
- Sadowsky, S.J. Mandibular implant-retained overdentures: A literature review. J. Prosthet. Dent. 2001, 86, 468–473.
- Cakarer, S.; Can, T.; Yaltirik, M.; Keskin, C. Complications associated with the ball, bar and locator attachments for implant-supported overdentures. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e953–e959.
- Payne, A.G.; Solomons, Y.F.; Tawse-Smith, A.; Lownie, J.F. Inter-abutment and peri-abutment mucosal enlargement with mandibular implant overdentures. Clin. Oral Implant. Res. 2001, 12, 179–187.
- Alsabeeha, N.H.; Swain, M.V.; Payne, A.G. Clinical performance and material properties of single-implant overdenture attachment systems. Int. J. Prosthodont. 2011, 24, 247–254.
- Alsabeeha, N.H.; Payne, A.G.; De Silva, R.K.; Thomson, W.M. Mandibular single-implant overdentures: Preliminary results of a randomised-control trial on early loading with different implant diameters and attachment systems. Clin. Oral Implant. Res. 2011, 22, 330–337.
- Kleis, W.K.; Kämmerer, P.W.; Hartmann, S.; Al-Nawas, B.; Wagner, W. A comparison of three different attachment systems for mandibular two-implant overdentures: One-year report. Clin. Implant Dent. Relat. Res. 2010, 12, 209–218.
- Vasant, R.; Vasant, M.K. Retention systems for implant-retained overdentures. Dent. Update 2013, 40, 28–31.
- ELsyad, M.A.; Fathe Mahanna, F.; Samir Khirallah, A.; Ali Habib, A. Clinical denture base deformation with different attachments used to stabilize implant overdentures: A crossover study. Clin. Oral Implant. Res. 2020, 31, 162–172.
- Chung, K.H.; Chung, C.Y.; Cagna, D.R.; Cronin, R.J., Jr. Retention characteristics of attachment systems for implant overdentures. J. Prosthodont.: Off. J. Am. Coll. Prosthodont. 2004, 13, 221–226.
- Naert, I.; Gizani, S.; Vuylsteke, M.; Van Steenberghe, D. A 5-year prospective randomized clinical trial on the influence of splinted and unsplinted oral implants retaining a mandibular overdenture: Prosthetic aspects and patient satisfaction. J. Oral Rehabil. 1999, 26, 195–202.
- Boeckler, A.F.; Ehring, C.; Morton, D.; Geis-Gerstorfer, J.; Setz, J.M. Corrosion of dental magnet attachments for removable prostheses on teeth and implants. J. Prosthodont.: Off. J. Am. Coll. Prosthodont. 2009, 18, 301–308.
- Laverty, D.P.; Green, D.; Marrison, D.; Addy, L.; Thomas, M.B. Implant retention systems for implant-retained overdentures. Br. Dent. J. 2017, 222, 347–359.
- Tallarico, M.; Cervino, G.; Scrascia, R.; Uccioli, U.; Lumbau, A.; Meloni, S.M. Minimally invasive treatment of edentulous maxillae with overdenture fully supported by a cad/cam titanium bar with a low-profile attachment screwed on four or six implants: A case series. Prosthesis 2020, 2, 53–64.
- Karabuda, C.; Tosun, T.; Ermis, E.; Ozdemir, T. Comparison of 2 retentive systems for implant-supported overdentures: Soft tissue management and evaluation of patient satisfaction. J. Periodontol. 2002, 73, 1067–1070.
- Chaware, S.H.; Thakkar, S.T. A systematic review and meta-analysis of the attachments used in implant-supported overdentures. J. Indian Prosthodont. Soc. 2020, 20, 255–268.
- Langer, A. Telescope retainers for removable partial dentures. J. Prosthet. Dent. 1981, 45, 37–43.
- Langer, A. Telescope retainers and their clinical application. J. Prosthet. Dent. 1980, 44, 516–522.
- Gonda, T.; Maeda, Y. Why are magnetic attachments popular in japan and other asian countries? Jpn. Dent. Sci. Rev. 2011, 47, 124–130.
- Mericske-Stern, R.; Oetterli, M.; Kiener, P.; Mericske, E. A follow-up study of maxillary implants supporting an overdenture: Clinical and radiographic results. Int. J. Oral Maxillofac. Implant. 2002, 17, 678–686.
- Kappel, S.; Giannakopoulos, N.N.; Eberhard, L.; Rammelsberg, P.; Eiffler, C. Immediate loading of dental implants in edentulous mandibles by use of locator ® attachments or dolder ® bars: Two-year results from a prospective randomized clinical study. Clin. Implant. Dent. Relat. Res. 2016, 18, 752–761.
- Boven, G.C.; Meijer, H.J.A.; Vissink, A.; Raghoebar, G.M. Maxillary implant overdentures retained by use of bars or locator attachments: 1-year findings from a randomized controlled trial. J. Prosthodont. Res. 2020, 64, 26–33.


