This study presents an overview of the biomechanical and biomolecular aspects of various attachments for implant overdenture. We focused on the following topics: attachment systems, retention of various attachments, stress distribution with different attachments, the design and fabrication of attachments, digital techniques in overdenture attachments, and the effects of attachments in peri-implant health. We found that plastic resin is commonly used for ball and bar attachments, whereas nylon resin is commonly used in locator attachments. The locator system offers a valuable attachment option for implant-retained overdenture. Attachment retention reduces while lateral force increases with implant inclination in overdenture. The higher the retention of an overdenture attachment, the higher the transferred stresses. Additionally, clip loading produces more stress in implants and precision elements than bar-retained dentures. As such, we conclude that the ball and locator systems the best overdenture systems due to their superior tissue response, survival rate, and patient satisfaction.
1. Introduction
At present, implants are widely used to replace missing teeth or retention/support dentures [
1]. The use of implant-retained overdentures in the maxilla and mandible is a successful option to the fixed implant prostheses. The types of attachments available in the market include non-splinted attachments (ball, magnet, locator, and double crown attachment) and splinted attachments (bar and clip attachment) [
2,
3,
4].
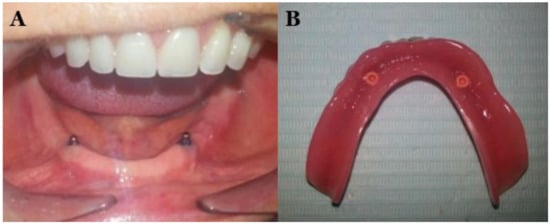
Figure 1 shows the ball attachment to retain overdenture [
3].
Figure 1. Ball attachment to retain overdenture (
A) and overdenture (tissue surface) (
B) [
3].
The locator attachment system is a suitable choice for implant-retained or implant-supported overdenture [
5]. There has been considerable development in attachments for implant overdenture; however, there is a need for updated information regarding implant overdenture attachments is lacking. As such, this review presents an overview of various attachments’ biomechanical and biomolecular aspects, with focus on attachment systems, the retention of various attachments, stress distribution with different attachments, the design and fabrication of attachments, digital techniques in overdenture attachments, and the effects of attachments in peri-implant health. After assessing the available articles on overdenture attachments from January 1980 to August 2021 using the PubMed/MEDLINE, ScienceDirect, and Web of Science resources, relevant studies on overdenture attachments were included in this study.
2. Effects of Attachment Types on Implant Overdenture
Attachments vary in shape and include ball, bar, locator, magnet, and locator types. Stud attachments are either rigid (ball) or resilient (magnet, locator, and double crown attachment). Table 1 presents an overview of the various attachments in overdenture.
Table 1. Advantages and disadvantages of the various attachments in overdenture.
| Attachment Type |
Advantages |
Disadvantages |
Reference |
Ball attachment
(O-ring attachment) |
Simple manufacturing process, the provision of a wide range of movement, cost-effectiveness, ease of use, good retention, easy hygiene maintenance, and high patient satisfaction. |
The abutment requires implants to be parallelly placed, and the loss of parallelism may cause difficulty while inserting and removing the prosthesis or during the fracturing of the abutment. The O-ring needs to be regularly changed because it is subject to wear. |
[10,11] |
| Bar attachment |
Provides retention, implant splinting, and wide-ranging load distribution that results in a movement reduction of the implants. |
Technique-sensitive, expensive, and present difficult hygiene maintenance under the bars, leading to mucosal swelling or gingival hyperplasia. Bars are not indicated in a V-shaped ridge because this leads to the infringement of tongue space. |
[12,13] |
| Locators |
Locators are popular attachments for implant-retained or implant-supported overdenture because of their low level of thickness (2.5 mm height) and ability to self-align, which can correct up to 40° of implant angulations. They can be used in narrow inter-arch space. Locators offer excellent retention and stability, and they allow for easy hygiene maintenance. The telescopic attachment, which offers a self-seating mechanism, is suitable for patients with reduced manual dexterity, such as those with Parkinson’s disease. |
Periodic replacement of the male nylon component is required. Some prosthetic complications such as locator attachments, periodic repair, and higher maintenance double-crown locator attachments require sufficient inter-arch space and the metal display of attachments. |
[8,14,15,16,17] |
| Magnetic attachments |
Magnetic attachments reduce the transfer of horizontal stress to the implants and bone during the insertion and removal of the denture. |
These are low-profile attachments; however, corrosion and loss of magnetism are significant complications associated with their usage. |
[18,19,20,21] |
The ball attachment (O-ring attachment) is the most commonly used overdentures and contains a ball shape for retention. Its advantages include a simple manufacturing process, the provision of a wide range of movement, cost-effectiveness, ease of use and maintenance, the provision of good retention, hygiene maintenance, and good patient satisfaction [
10,
11]. However, the ball attachment abutment requires implants to be parallelly placed, and the loss of parallelism may cause difficulty while inserting and removing the prosthesis or during the fracturing of the abutment [
10]. Additionally, the O-ring needs to be regularly changed because it is subject to wear [
10].
A bar attachment offers retention, the splinting of implants, and the distribution of load, resulting in reduced implant stress, which is critical for the immediate loading protocol [
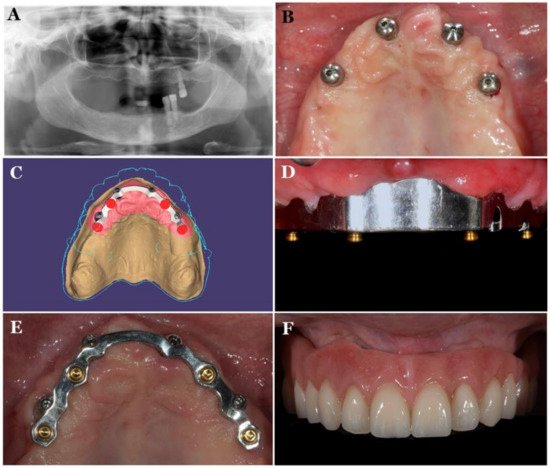
12]. The restoration of moderately to severely atrophic maxilla remains a challenge. In such cases, CAD/CAM titanium bar-supported overdenture can be an important treatment choice for an edentulous patient’s rehabilitation (
Figure 2) [
22].
Figure 2 shows a maxillary overdenture supported by four or six implants for the minimally invasive rehabilitation of atrophic maxillae. The disadvantages of bar attachments include technique-sensitivity, high costs, and difficult hygiene maintenance under the bars that leads to mucosal swelling or gingival hyperplasia [
12,
13]. Furthermore, bars are not indicated in a V-shaped ridge because this causes the infringement of tongue space [
23].
Figure 2. CAD/CAM titanium-bar-supported maxillary overdenture Pretreatment radiograph (
A), 4 implants placed in maxillary arch (
B), CAD design of the titanium bar (
C), titanium bar inserted in the mouth (
D), occlusal view of titanium bar (
E), definitive prosthesis (
F) [
22].
Locators are currently popular attachments because of their low level of thickness (2.5 mm height) [
16] and ability to self-align, which can correct up to 40° of implant angulations [
16]. They can be used in narrow inter-arch space and prevent the fracture of the denture base [
17]. Locators offer excellent retention and stability, and they allow for easy hygiene maintenance. The telescopic attachment, which offers a self-seating mechanism, is appropriate for patients with reduced manual dexterity, such as those with Parkinson’s disease. However, the periodic replacement of the male nylon part is required [
14]. Some prosthetic complications have been noted in locator attachments. One study reported 34 prosthetic complications and a locator housing requiring 16 replacements [
8,
15]. To avoid complications, locator attachments require periodic repair and higher maintenance [
24]. Recently, researchers invented a double-crown attachment option for locator attachments have that connects dentures to prepared teeth [
25]. However, the disadvantages of locators include the need for sufficient inter-arch space and the metal display of attachments [
26]. The locator attachment system is a suitable choice for implant-retained or implant-supported overdenture [
5].
Magnetic attachments have a long history (>60 years) of use in denture retention [
27]. They reduce the transfer of horizontal stress to the implants and the bone during the insertion and removal of the denture [
18]. They are low-profile attachments [
19], and the corrosion and loss of magnetism are significant complications associated with their usage [
20,
21].
Overdenture attachments present very high survival rates. One study reported survival rates ranging from 96% to 97% for bar attachments, 96% to 100% for ball attachments, 90% to 92% for magnets, and 97% for locators with a mean follow-up period of 3 years [
24]. Other studies have reported a 94% five-year survival rate for the bar attachment [
28]; 89% and 93% survival rates for the bar and locator, respectively; [
29], and 98% and 97% survival rates for the bar and the locator, respectively [
30].
This entry is adapted from the peer-reviewed paper 10.3390/polym13193248