Mirizzi syndrome is a rare condition caused by the compression of the common hepatic duct due to stones located in the cystic duct or the neck of the gallbladder, which causes obstruction of the extrahepatic biliary tract, what is most commonly presented as jaundice and upper abdominal pain. Mirizzi syndrome occurs approximately in 0.05-4% of patients undergiong cholecystectomy. Prolonged inflammation caused by the stones impacted in the cystic duct or the neck of the gallbladder may lead to advanced stages of Mirizzi syndrome and the formation of a cholecystocholedochal fistula or even a cholecystoenteric fistula. Diagnosis is made upon the symptoms, laboratory results and imaging techniques such as ultrasonography, computed tomography, magnetic resonance imaging or endoscopic retrograde choleangiopancreatography (ERCP), which is considered as the golden standard. However, the preoperative diagnosis is difficult and a large part of all cases is diagnosed intraoperatively. Management of Mirizzi syndrome is mostly surgical, but early stages of the syndrome can be treated with the use of ERCP.
1. Introduction
Mirizzi syndrome (MS) is a rare condition caused by the compression of the common hepatic duct due to stones located in the cystic duct or the neck of the gallbladder. The main symptoms noticed in patients with this condition are upper abdominal pain and jaundice
[1][2][3]. It was first mentioned in 1905 by Kehr and later in 1908 by Ruge, who described it as a disease caused by the external obstruction of the bile duct associated with jaundice. Eventually, in 1948, the Argentinean surgeon Pablo Mirizzi defined it as the compression of a bile duct by a gallstone, associated with pressure ulceration generating local inflammation. The compression may lead to external obstruction, erosion, fibrosis or fistula with various levels of complexity
[1][4][5]. It means that it can be generally depicted as an uncommon manifestation of cholelithiasis
[2]. The reported frequency of MS is approximately 0.05–4%. Based on data presented in articles, the overall frequency of MS was higher in females than in males. The proportion of females suffering from MS ranged between 55.6–77%
[6][7][8][9][10]. However, the available data vary in different parts of the world. Thus, in well-developed countries and regions, such as Europe, MS is found in 0.5% of all cholecystectomies, but in Asia, Central and South America the statistics are generally higher and reach as much as 4.7–5.7%
[1][11][12][13][14][15]. In the population of patients undergoing endoscopic retrograde cholepancreatography (ERCP), the incidence of MS is estimated to be 1.07%
[5].
Two main, widely used classifications for Mirizzi syndrome can be found in original papers. McSherry’s paper proposes a classification based on ERCP findings and distinguished two types of MS. Furthermore, Csendes’ classification determines four types of MS, but it is based on dividing cholecystobiliary communication into three types according to the size of the cholecystocholedochal fistula in comparison to the common bile duct (CBD)
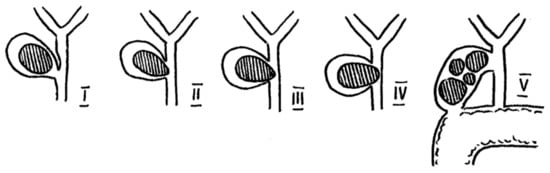
[1][16]. A schematic sketch of MS is presented in
Figure 1.
Figure 1. Anatomical sketch of Mirizzi Syndrome according to Csendes and Beltrán (2008).
2. Classification
The first classification of Mirizzi syndrome was developed by Corlette et al. in 1975 and they identified two types depending on the degree of cholecystobiliary fistulas
[17]. However, the first widely accepted classification, which is still used today, was prepared by McSherry et al. in 1982 based on the ERCP findings. They divided MS into two types, in which type I was an external compression of the bile duct by a gallstone impacted in the neck of the gallbladder and type II was a cholecystobiliary fistula caused by eroded stones
[18].
In 1989, Csendes et al. proposed a classification which expanded the one proposed by McSherry. The authors presented four types of the syndrome—type I, which was equal to the McSherry type I; and types II–IV relating to the different stages of the fistula. Type II represents a cholecystobiliary fistula with up to one-third of bile duct wall erosion. Type III consists of a fistula involving two-thirds of the bile duct wall. Finally, type IV refers to the complete destruction of the bile duct and its walls being fused with the gallbladder
[19]. This classification remained unchanged for almost two decades, but in 2008 Csendes and Beltrán complemented the previous classification by adding types Va and Vb. Type Va includes an uncomplicated cholecystoenteric fistula, while type Vb represents a cholecystoenteric fistula followed by a gallstone ileus
[20].
Meanwhile, in 1997 Nagakawa et al. proposed a different classification based on their own experience, in which types I and II were consistent with the McSherry classification, but type III involved the presence of stones in the confluence of the cystic duct and the common hepatic duct, and type IV was determined as a bile duct stricture without stones, but due to an inflammatory process such as cholecystitis
[21].
In 2009 Solis-Caxaj suggested a way to simplify Cesendes and Beltrán’s classification into three types: types I and II were the same as McSherry’s types regarding cholecystoenteric fistulas—IIIa (without gallstone ileus) and IIIb (with gallstone ileus)
[22]. Based on this suggestion, Beltrán et al. validated the previous classification in 2012 by implementing Solis-Caxaj types IIIa and IIIb instead of types Va and Vb, but also resigned from the previous types II-IV and simplified them to types IIa (a fistula involving <50% of the bile duct diameter) and IIb (a fistula involving >50% of the bile duct diameter)
[23].
In 2017, Payá-Llorente et al. proposed a modified classification based upon Beltrán’s from 2012. The authors in this article make the point that, in their opinion, the presence of a cholecystoenteric fistula should not constitute a type of Mirizzi syndrome, but rather a subtype. Thus they formed a 3 type classification with A, B and C subtypes for each number. Type 1 is extrinsic compression of CHD, types 2 and 3 describe a cholecystobiliary fistula that affects <50% of CBD (2) and >50% of CBD (3). Subtypes A, B and C always correspond to the cholecystoenteric fistula in which A means no fistula, while B and C refer to a fistula with (B) or without (C) gallstone ileus. The researchers also suggested proper schemes of treatment along with their classification, which can be helpful in planning the management of MS
[24]. The above classifications have been gathered in
Table 1.
Table 1. Classifications of Mirizzi Syndrome.
| Authors |
McSherry et al.-1982 |
Csendes et al.-1989 and Complemented in 2008 |
Beltrán et al.-2012 |
Payá-Llorente et al.-2017 |
Nagakawa et al.-1997 |
| Classification |
Type I—external compression of the bile duct |
Type I—external compression of the bile duct |
Type I—external compression of the bile duct |
Type 1—external compression of the bile duct |
Type I—external compression of the bile duct |
| Type II—cholecystobiliary fistula |
Type II—cholecystobiliary fistula—up to 1/3 of the bile duct wall erosion |
Type IIa—cholecystobiliary fistula involving <50% of the bile duct diameter |
Type 2—cholecystobiliary fistula involving <50% of the bile duct diameter |
Type II—cholecystobiliary fistula |
| Type III—cholecystobiliary fistula—up to 2/3 of the bile duct wall erosion |
| Type IV—cholecystobiliary fistula—complete destruction of the bile duct wall and fusion with gallbladder |
Type IIb—cholecystobiliary fistula involving >50% of the bile duct diameter |
Type 3—cholecystobiliary fistula involving >50% of the bile duct diameter |
| |
Type Va—cholecystoenteric fistula |
Type IIIa—cholecystoenteric fistula |
Subtypes describing cholecystoenteric fistula: A-no fistula/B-fistula without gallstone ileus/C-fistula with gallstone ileus |
Type III—gallstones in the cystic duct and common hepatic duct confluence |
| |
Type Vb—cholecystoenteric fistula with gallstone ileus |
Type IIIb—cholecystoenteric fistula with gallstone ileus |
Type IV—stricture without stones (e.g., due to cholecystitis) |
Among the articles that were reviewed, one study conducted by Ya Feng Ji et al. compared two classifications—by Csendes and by Nagakawa—for their accuracy in MS diagnosis by computed tomography (CT) and magnetic resonance imaging (MRI). The evaluation proved Nagakawa‘s system to be superior to Csendes’ in terms of diagnostic accuracy
[25].
3. Symptoms, laboratory resulst and imaging
Several symptoms were acknowledged in patients suffering from MS. According to the original papers, the most common symptoms were abdominal pain (incidence 65.7–100%) and jaundice (ranging between 45–87.5%). Other symptoms were nausea and vomiting (31–62%), cholangitis (up to 56%), fever (21–42%) and anorexia (11–29.2%)
[6][7][26][27][28][29][30]. Furthermore, Shirah et al. reported that there was a positive Murphy’s sign in 50% of their patients during physical examination
[6]. The mean duration of the various symptoms was determined to be between 3 to 24 months
[13][24][31], but it is worth mentioning that Prasad et al. noticed that symptoms in patients suffering from uncomplicated gallstone disease lasted half as long as in those with MS
[32]. The overall percentage of asymptomatic patients ranged between 3.7% and 17%
[26][33].
Several original articles present laboratory test results performed on patients with MS. The most common examinations are white blood cell count (WBC), alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), bilirubin and gamma-glutamyl transpeptidase (GGT).
Leukocytosis was diagnosed in 73.4% of MS patients in the study by Shirah et al.
[6]. Ahlawat reported elevated WBC only if acute cholecystitis, cholangitis or pancreatitis occurred along with MS
[34]. Articles that present numerological data show that mean WBC levels are generally around the upper limit of normal levels or slightly beyond. A few papers specify the results for different types of MS. According to Payá-Llorente and Erben
[24][26], mean WBC levels were moderately lower when a cholecystobiliary fistula was present. On the other hand, Lledó et al. presented contrary data with an inverted trend
[29].
ALT and AST levels are reported to be generally elevated in 39–98% of tests for ALT and 37–89% for AST
[6][27][30][33][34]. According to some of the articles, the mean levels of ALT and AST in MS patients are several times higher than normal and can reach 286 and 263 U/L, respectively. Data describing those parameters in relation to MS type are inconsistent. Erben et al. report a significant decline in AST and ALT levels from over 250 U/L to less than 100 U/L when there is a cholecystobilliary fistula, while Lledó et al. show a gradual growth in the levels of the parameters with the advancement of the fistula, but neither ALT or AST exceed 90 U/L in this study
[8][15][26][29].
The results of ALP test are said to be elevated in even 93.8% of patients and its mean levels are reported to be approximately 324–402 U/L, but can be as high as 1236 U/L
[15][27][30][31][33][35].
Most authors concur that total bilirubin levels are elevated in MS patients—even in as many as 92.2% of them
[6][30][33]. Payá-Llorente as well as Lledó report increasing mean levels of bilirubin with the advancement of the cholecystobiliary fistula. Erben et al., however, present data showing a decline in blilirubin when there is a cholecystobiliary fistula. Interestingly, Payá-Llorente and colleagues report much lower bilirubin in Csendes type V, which may be due to a discharge of the bile straight to the intestines. Generally, the mean bilirubin levels are reported to be between 2–9.9 mg%
[8][15][24][26][29][31][35].
The literature is consistent when it comes to GGT levels, which are commonly elevated according to multiple articles. The mean range could be depicted as 204–1018 U/L
[15][24][27][33][35].
Ultrasonography was the initial diagnostic tool used in a number of studies, but its sensitivity ranged from a few percent up to about 50%. One study, however, reported that US could reveal a suspicion of MS in almost 80% of patients. In our opinion, suspected MS in an US is enough information to guide the next steps in the diagnostic process. Some authors claim that introducing modern US imaging could raise the effectiveness of this method
[36].
CT proved to be approximately as sensitive as the US, but it was repeatedly pointed out that its main advantage is differentiating MS from malignant strictures
[29][30]. MS is listed as one of the diseases mimicking cholangiocarcinoma, but the fact us that the coexistence of MS and GBC is no less important
[32][37][38][39]. Prasad et al. reported that patients with MS and simultaneous GBC were a decade older than and had twice as long a history of symptoms as patients who only had MS alone
[32].
MRCP and ERCP compete for the best diagnostic modality. Both showed high levels of sensitivity—in general 63–89% for MRCP and 63–72% for ERCP with singular reports of lower and higher effectiveness. Nevertheless, ERCP is still widely recognised as the gold standard in MS diagnosis, thanks to its high sensitivity and therapeutic options
[31][40]. The low availability and high cost of MRCP are its main drawbacks, preventing it from being commonly used
[40]. Furthermore, MRCP without a conventional MRI may sometimes struggle to differentiate benign from malignant causes of biliary stricture
[35]. Yun et al. report that combining MRCP and CT might increase the number of patients being diagnosed
[41].
Some other diagnostic methods emerge in original papers. Authors report EUS as a relatively good tool with a level of sensitivity similar to ERCP ranging from 63–73%
[31][35]. Interesting data are delivered by Wehrmann et al. about IDUS, which was reported to be diagnostically accurate in 97% of cases. According to the article, the biggest concerns preventing the widespread use of IDUS are the costs, the length of the procedure and the technical difficulties caused by damage to the IDUS probes. However, the authors mention that the cost of one probe, which can be used several hundred times, is about EUR 3500 euros, and the additional time needed to perform IDUS was 8 min on average
[35].
Recently, Tataria et al. published a study that is new in the field of MS management and diagnosis. On the basis of research from various databases and after taking into account clinical, biochemical and radiological parameters presented in MS, the authors developed a scoring system to help predict Mirizzi syndrome preoperatively. The scale consists of 10 parameters gathered in 3 groups: clinical, biochemical and imaging. Each parameter is given 0 or 1 point. In clinical parameters +1 point could be noted for: symptom duration symptoms >24 months; the frequency of abdominal pain >1; and the presence of jaundice. The biochemical results which are given +1 point are: bilirubin level >1.2 mg%; leukocytosis >11,000/mm
3; and alkaline phosphatase level >150 U/L. The radiological features included in the scale are: the presence of hepatolithiasis/choledocholithiasis; intrahepatic biliary radical dilatation (IHBRD); meniscus sign; and mass at the confluence. The analysis included retrospectively collected data from 96 patients with complicated cholecystitis, who were divided into two groups—the first-without MS and the second with MS. There were 32 patients with MS. The authors further evaluated the patients according to the scoring system they had developed and conducted a statistical analysis which showed that a score of 3 or more out of 10 has a sensitivity of 90.6% and specificity of 78.1% in predicting the Mirizzi syndrome
[39].
Making a preoperative diagnosis is still difficult, but the numbers vary greatly—between 12% and 84%. Many authors underline the importance of a preoperative diagnosis of MS to avoid exposing surgeons to difficult operating conditions and therefore to limit complications by choosing the right approach
[42][43][44][45]. Along with a precise diagnosis, proper treatment must follow. Open cholecystectomy is in general accepted as the procedure of choice, yet some studies recommend a laparoscopic approach, which is said to be safe, especially when there is no cholecystobiliary fistula
[31][42]. However, it is crucial that MS is diagnosed preoperatively when planning laparoscopic treatment. Research shows a high conversion rate when the diagnosis in not made prior to the surgery and this increases with the advancement of the disease
[42][46].
 +1 credit
+1 credit