 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Anagha Kumar | + 2584 word(s) | 2584 | 2021-07-15 10:57:24 | | | |
| 2 | Lily Guo | Meta information modification | 2584 | 2021-07-28 02:54:08 | | |
Video Upload Options
Social distancing has been a critical public health measure for the COVID-19 pandemic, yet a long history of research strongly suggests that loneliness and social isolation play a major role in several cognitive health issues. What is the true severity and extent of risks involved and what are potential approaches to balance these competing risks? This review aimed to summarize the neurological context of social isolation and loneliness in population health and the long-term effects of social distancing as it relates to neurocognitive aging, health, and Alzheimer’s disease and related dementias. The full scope of the underlying causal mechanisms of social isolation and loneliness in humans remains unclear partly because its study is not amenable to randomized controlled trials; however, there are many detailed experimental and observational studies that may provide a hypothesis-generating theoretical framework to better understand the pathophysiology and underlying neurobiology. To address these challenges and inform future studies, we conducted a topical review of extant literature investigating associations of social isolation and loneliness with relevant biological, cognitive, and psychosocial outcomes, and provide recommendations on how to approach the need to fill key knowledge gaps in this important area of research.
1. Introduction
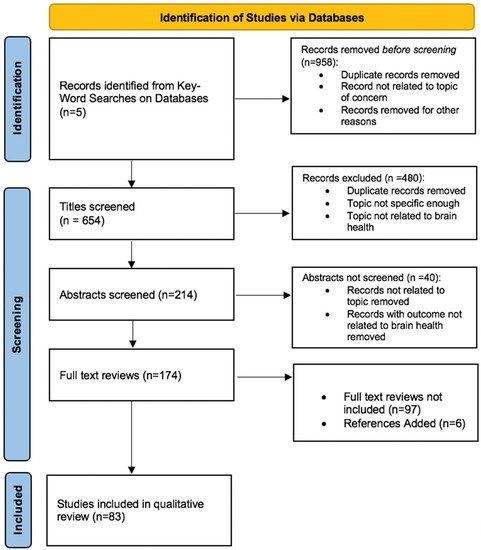
2. Study Selections
3. Biological Outcomes
3.1. Associations with Inflammation
3.2. Associations with Neuroimaging Measures
3.3. Associations with Neuropathology
3.4. Associations with Neuroplasticity
3.5. Associations with Sleep
4. Cognitive Outcomes
Associations with Cognitive Function
5. Psychosocial Outcomes
5.1. Associations with Depression, Anxiety, and Stress
5.2. Mediating and Modifying Factors
6. Future Directions
6.1. Intervention Studies
6.2. Recommendations to Address Knowledge Gaps
References
- Holt-Lunstad, J.; Smith, T.B.; Layton, J.B. Social Relationships and Mortality Risk: A Meta-analytic Review. PLoS Med. 2010, 7, e1000316.
- Luo, Y.; Hawkley, L.C.; Waite, L.J.; Cacioppo, J.T. Loneliness, health, and mortality in old age: A national longitudinal study. Soc. Sci. Med. 2012, 74, 907–914.
- McGinty, E.E.; Presskreischer, R.; Han, H.; Barry, C.L. Psychological Distress and Loneliness Reported by US Adults in 2018 and April 2020. JAMA 2020, 324, 93.
- Evans, I.E.; Martyr, A.; Collins, R.; Brayne, C.; Clare, L. Social Isolation and Cognitive Function in Later Life: A Systematic Review and Meta-Analysis. J. Alzheimer Dis. 2019, 70, S119–S144.
- Okamoto, S.; Kobayashi, E. Social Isolation and Cognitive Functioning: A Quasi-Experimental Approach. J. Gerontol. Ser. B 2020.
- Cacioppo, J.T.; Cacioppo, S. Social Relationships and Health: The Toxic Effects of Perceived Social Isolation. Soc. Personal. Psychol. Compass 2014, 8, 58–72.
- Clair, R.; Gordon, M.; Kroon, M.; Reilly, C. The effects of social isolation on well-being and life satisfaction during pandemic. Humanit. Soc. Sci. Commun. 2021, 8, 1–6.
- Livingston, G.; Huntley, J.; Sommerland, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446.
- Necka, E. After COVID, Research on Social Isolation and Loneliness Is Needed More than Ever; National Institute on Aging: Bethesda, MD, USA, 2021.
- Donovan, N.J.; Okereke, O.I.; Vannini, P.; Amariglio, R.E.; Rentz, D.M.; Marshall, G.A.; Johnson, K.A.; Sperling, R.A. Association of Higher Cortical Amyloid Burden With Loneliness in Cognitively Normal Older Adults. JAMA Psychiatry 2016, 73, 1230.
- Poey, J.L.; Burr, J.A.; Roberts, J.S. Social Connectedness, Perceived Isolation, and Dementia: Does the Social Environment Moderate the Relationship Between Genetic Risk and Cognitive Well-Being? Gerontologist 2017, 57, 1031–1040.
- Cudjoe, T.K.M.; Roth, D.L.; Szanton, S.L.; Wolff, J.L.; Boyd, C.M.; Thorpe, R.J. The Epidemiology of Social Isolation: National Health and Aging Trends Study. J. Gerontol. Ser. B 2020, 75, 107–113.
- Holwerda, T.J.; Deeg, D.J.H.; Beekman, A.T.F.; van Tilburg, T.; Stek, M.L.; Jonker, C.; Schoevers, R.A. Feelings of loneliness, but not social isolation, predict dementia onset: Results from the Amsterdam Study of the Elderly (AMSTEL). J. Neurol. Neurosurg. Psychiatry 2014, 85, 135–142.
- Koyama, Y.; Nawa, N.; Yamaoka, Y.; Nishimura, H.; Sonoda, S.; Kuramochi, J.; Miyazaki, Y.; Fujiwara, T. Interplay between social isolation and loneliness and chronic systemic inflammation during the COVID-19 pandemic in Japan: Results from U-CORONA study. Brain Behav. Immun. 2021, 94, 51–59.
- Cole, S.W.; Hawkley, L.C.; Arevalo, J.M.; Sung, C.Y.; Rose, R.M.; Cacioppo, J.T. Social regulation of gene expression in human leukocytes. Genome Biol. 2007, 8, R189.
- Smith, K.J.; Gavey, S.; Riddell, N.E.; Kontari, P.; Victor, C. The association between loneliness, social isolation and inflammation: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2020, 112, 519–541.
- Vingeliene, S.; Hiyoshi, A.; Lentjes, M.; Fall, K.; Montgomery, S. Longitudinal analysis of loneliness and inflammation at older ages: English longitudinal study of ageing. Psychoneuroendocrinology 2019, 110, 104421.
- Walker, E.; Ploubidis, G.; Fancourt, D. Social engagement and loneliness are differentially associated with neuro-immune markers in older age: Time-varying associations from the English Longitudinal Study of Ageing. Brain Behav. Immun. 2019, 82, 224–229.
- Lind, A.; Salomäki, S.; Parkkola, R.; Haataja, L.; Rautava, P.; Junttila, A.; Koikkalainen, J.; Lötjönen, J.; Saunavaara, V.; Korja, R.; et al. Brain volumes in relation to loneliness and social competence in preadolescents born very preterm. Brain Behav. 2020, 10, e01640.
- Kanai, R.; Bahrami, B.; Duchaine, B.; Janik, A.; Banissy, M.J.; Rees, G. Brain Structure Links Loneliness to Social Perception. Curr. Biol. 2012, 22, 1975–1979.
- Kanai, R.; Bahrami, B.; Roylance, R.; Rees, G. Online social network size is reflected in human brain structure. Proc. R. Soc. B Biol. Sci. 2012, 279, 1327–1334.
- Uquillas, F.D.; Jacobs, H.I.L.; Biddle, K.D.; Properzi, M.; Hanseeuw, B.; Schultz, A.P.; Rentz, D.M.; Johnson, K.A.; Sperling, R.A.; Donovan, N.J. Regional tau pathology and loneliness in cognitively normal older adults. Transl. Psychiatry 2018, 8.
- Spreng, R.N.; Dimas, E.; Mwilambwe-Tshilobo, L.; Dagher, A.; Koellinger, P.; Nave, G.; Ong, A.; Kernbach, J.M.; Wiecki, T.V.; Ge, T.; et al. The default network of the human brain is associated with perceived social isolation. Nat. Commun. 2020, 11, 1–11.
- Dong, H.; Goico, B.; Martin, M.; Csernansky, C.; Bertchume, A.; Csernansky, J.; Dong, H.; Goico, B.; Martin, M.; Csernansky, C.; et al. Modulation of hippocampal cell proliferation, memory, and amyloid plaque deposition in APPsw (Tg2576) mutant mice by isolation stress. Neuroscience 2004, 127, 601–609.
- Bennett, D.A.; Schneider, J.A.; Tang, Y.; Arnold, S.E.; Wilson, R.S. The effect of social networks on the relation between Alzheimer’s disease pathology and level of cognitive function in old people: A longitudinal cohort study. Lancet Neurol. 2006, 5, 406–412.
- Hankey, G.J. Social Network and Stroke Risk. Stroke 2014, 45, 2853–2854.
- Nagayoshi, M.; Everson-Rose, S.; Iso, H.; Mosley, T.H.; Rose, K.M.; Lutsey, P.L. Social Network, Social Support, and Risk of Incident Stroke. Stroke 2014, 45, 2868–2873.
- Holmes, A.; Xu, Y.; Lee, J.; Maniskas, M.E.; Zhu, L.; McCullough, L.D.; Venna, V.R. Post-Stroke Social Isolation Reduces Cell Proliferation in the Dentate Gyrus and Alters miRNA Profiles in the Aged Female Mice Brain. Int. J. Mol. Sci. 2020, 22, 99.
- Venna, V.R.; Xu, Y.; Doran, S.; Patrizz, A.; McCullough, L.D. Social interaction plays a critical role in neurogenesis and recovery after stroke. Transl. Psychiatry 2014, 4, e351.
- Van Praag, H.; Kempermann, G.; Gage, F.H. Neural consequences of enviromental enrichment. Nat. Rev. Neurosci. 2000, 1, 191–198.
- Gheusi, G.; Ortega-Perez, I.; Murray, K.; Lledo, P.-M. A niche for adult neurogenesis in social behavior. Behav. Brain Res. 2009, 200, 315–322.
- Hsiao, Y.-H.; Hung, H.-C.; Chen, S.-H.; Gean, P.-W. Social Interaction Rescues Memory Deficit in an Animal Model of Alzheimer’s Disease by Increasing BDNF-Dependent Hippocampal Neurogenesis. J. Neurosci. 2014, 34, 16207–16219.
- Dunlap, K.D.; Chung, M. Social novelty enhances brain cell proliferation, cell survival, and chirp production in an electric fish, Apteronotus leptorhynchus. Dev. Neurobiol. 2013, 73, 324–332.
- Dunlap, K.D.; Chung, M.; Castellano, J.F. Influence of long-term social interaction on chirping behavior, steroid levels and neurogenesis in weakly electric fish. J. Exp. Biol. 2013, 216, 2434–2441.
- Dunlap, K.D.; Silva, A.C.; Chung, M. Environmental complexity, seasonality and brain cell proliferation in a weakly electric fish, Brachyhypopomus gauderio. J. Exp. Biol. 2011, 214, 794–805.
- Lieberwirth, C.; Wang, Z. The Social Environment and Neurogenesis in the Adult Mammalian Brain. Front. Hum. Neurosci. 2012, 6, 118.
- Zupanc, G.K.H.; Sîrbulescu, R.F. Adult neurogenesis and neuronal regeneration in the central nervous system of teleost fish. Eur. J. Neurosci. 2011, 34, 917–929.
- Westenbroek, C.; Boer, J.A.D.; Veenhuis, M.; Ter Horst, G.J. Chronic stress and social housing differentially affect neurogenesis in male and female rats. Brain Res. Bull. 2004, 64, 303–308.
- Li, M.; Du, W.; Shao, F.; Wang, W. Cognitive dysfunction and epigenetic alterations of the BDNF gene are induced by social isolation during early adolescence. Behav. Brain Res. 2016, 313, 177–183.
- Salinas, J.; Beiser, A.; Himali, J.J.; Satizabal, C.L.; Aparicio, H.; Weinstein, G.; Mateen, F.J.; Berkman, L.F.; Rosand, J.; Seshadri, S. Associations between social relationship measures, serum brain-derived neurotrophic factor, and risk of stroke and dementia. Alzheimer Dement. Transl. Res. Clin. Interv. 2017, 3, 229–237.
- Benson, J.A.; McSorley, V.E.; Hawkley, L.C.; Lauderdale, D.S. Associations of loneliness and social isolation with actigraph and self-reported sleep quality in a national sample of older adults. Sleep 2021, 44.
- Eccles, A.M.; Qualter, P.; Madsen, K.R.; Holstein, B. Loneliness in the lives of Danish adolescents: Associations with health and sleep. Scand. J. Public Health 2020, 48, 877–887.
- Cacioppo, J.T.; Hawkley, L.C.; Berntson, G.G.; Ernst, J.M.; Gibbs, A.C.; Stickgold, R.; Hobson, J.A. Do Lonely Days Invade the Nights? Potential Social Modulation of Sleep Efficiency. Psychol. Sci. 2002, 13, 384–387.
- Hawkley, L.C.; Preacher, K.J.; Cacioppo, J.T. Loneliness impairs daytime functioning but not sleep duration. Health Psychol. 2010, 29, 124–129.
- Jacobs, J.M.; Cohen, A.; Hammerman-Rozenberg, R.; Stessman, J. Global Sleep Satisfaction of Older People: The Jerusalem Cohort Study. J. Am. Geriatr. Soc. 2006, 54, 325–329.
- Kurina, L.M.; Knutson, K.; Hawkley, L.C.; Cacioppo, J.T.; Lauderdale, D.S.; Ober, C. Loneliness Is Associated with Sleep Fragmentation in a Communal Society. Sleep 2011, 34, 1519–1526.
- Riegel, B.; Weaver, T.E. Poor sleep and impaired self-care: Towards a comprehensive model linking sleep, cognition, and heart failure outcomes. Eur. J. Cardiovasc. Nurs. 2009, 8, 337–344.
- Nebes, R.D.; Buysse, D.J.; Halligan, E.M.; Houck, P.R.; Monk, T.H. Self-Reported Sleep Quality Predicts Poor Cognitive Performance in Healthy Older Adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2009, 64, 180–187.
- McHugh, J.E.; Casey, A.M.; Lawlor, B.A. Psychosocial correlates of aspects of sleep quality in community-dwelling Irish older adults. Aging Ment. Health 2011, 15, 749–755.
- Griffin, S.C.; Williams, A.B.; Ravyts, S.G.; Mladen, S.N.; Rybarczyk, B.D. Loneliness and sleep: A systematic review and meta-analysis. Health Psychol. Open 2020, 7, 205510292091323.
- Cacioppo, J.T.; Ernst, J.M.; Burleson, M.H.; McClintock, M.K.; Malarkey, W.B.; Hawkley, L.C.; Kowalewski, R.B.; Paulsen, A.; Hobson, J.; Hugdahl, K.; et al. Lonely traits and concomitant physiological processes: The MacArthur social neuroscience studies. Int. J. Psychophysiol. 2000, 35, 143–154.
- Hawkley, L.C.; Thisted, R.A.; Cacioppo, J.T. Loneliness predicts reduced physical activity: Cross-sectional & longitudinal analyses. Health Psychol. 2009, 28, 354–363.
- Donovan, N.J.; Wu, Q.; Rentz, D.M.; Sperling, R.A.; Marshall, G.A.; Glymour, M.M. Loneliness, depression and cognitive function in older U.S. adults. Int. J. Geriatr. Psychiatry 2017, 32, 564–573.
- Ertel, K.A.; Glymour, M.M.; Berkman, L.F. Effects of Social Integration on Preserving Memory Function in a Nationally Representative US Elderly Population. Am. J. Public Health 2008, 98, 1215–1220.
- Wallace, D.L.; Han, M.-H.; Graham, D.L.; Green, T.A.; Vialou, V.; Iñiguez, S.; Cao, J.-L.; Kirk, A.; Chakravarty, S.; Kumar, A.; et al. CREB regulation of nucleus accumbens excitability mediates social isolation–induced behavioral deficits. Nat. Neurosci. 2009, 12, 200–209.
- Luchetti, M.; Terracciano, A.; Aschwanden, D.; Lee, J.H.; Stephan, Y.; Sutin, A.R. Loneliness is associated with risk of cognitive impairment in the Survey of Health, Ageing and Retirement in Europe. Int. J. Geriatr. Psychiatry 2020, 35, 794–801.
- Wilson, R.S.; Krueger, K.R.; Arnold, S.E.; Schneider, J.A.; Kelly, J.F.; Barnes, L.L.; Tang, Y.; Bennett, D.A. Loneliness and Risk of Alzheimer Disease. Arch. Gen. Psychiatry 2007, 64, 234.
- Yu, B.; Steptoe, A.; Chen, Y.; Jia, X. Social isolation, rather than loneliness, is associated with cognitive decline in older adults: The China Health and Retirement Longitudinal Study. Psychol. Med. 2021, 1–8.
- Stewart, C.C.; Yu, L.; Glover, C.M.; Mottola, G.; Bennett, D.A.; Wilson, R.S.; Boyle, P.A. Loneliness Interacts With Cognition in Relation to Healthcare and Financial Decision Making Among Community-Dwelling Older Adults. Gerontologist 2020, 60, 1476–1484.
- Tilvis, R.S.; Kähönen-Väre, M.H.; Jolkkonen, J.; Valvanne, J.; Pitkala, K.H.; Strandberg, T.E. Predictors of Cognitive Decline and Mortality of Aged People Over a 10-Year Period. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, M268–M274.
- Akhter-Khan, S.C.; Tao, Q.; Ang, T.F.A.; Itchapurapu, I.S.; Alosco, M.L.; Mez, J.; Piers, R.J.; Steffens, D.C.; Au, R.; Qiu, W.Q. Associations of loneliness with risk of Alzheimer’s disease dementia in the Framingham Heart Study. Alzheimer Dement. 2021.
- Sundström, A.; Adolfsson, A.N.; Nordin, M.; Adolfsson, R. Loneliness Increases the Risk of All-Cause Dementia and Alzheimer’s Disease. J. Gerontol. Ser. B 2020, 75, 919–926.
- Sutin, A.R.; Stephan, Y.; Luchetti, M.; Terracciano, A. Loneliness and Risk of Dementia. J. Gerontol. Ser. B 2020, 75, 1414–1422.
- Sun, W.; Matsuoka, T.; Oba, H.; Narumoto, J. Importance of loneliness in behavioral and psychological symptoms of dementia. Int. J. Geriatr. Psychiatry 2021, 36, 540–546.
- Krendl, A.C.; Perry, B.L. The Impact of Sheltering in Place During the COVID-19 Pandemic on Older Adults’ Social and Mental Well-Being. J. Gerontol. Ser. B 2021, 76, e53–e58.
- Lee, S.L.; Pearce, E.; Ajnakina, O.; Johnson, S.; Lewis, G.; Mann, F.; Pitman, A.; Solmi, F.; Sommerlad, A.; Steptoe, A.; et al. The association between loneliness and depressive symptoms among adults aged 50 years and older: A 12-year population-based cohort study. Lancet Psychiatry 2021, 8, 48–57.
- McQuaid, R.J.; Cox, S.M.; Ogunlana, A.; Jaworska, N. The burden of loneliness: Implications of the social determinants of health during COVID-19. Psychiatry Res. 2021, 296, 113648.
- Rivera, D.S.; Lindsay, C.B.; Oliva, C.A.; Codocedo, J.F.; Bozinovic, F.; Inestrosa, N.C. Effects of long-lasting social isolation and re-socialization on cognitive performance and brain activity: A longitudinal study in Octodon degus. Sci. Rep. 2020, 10, 18315.
- van Roekel, E.; Ha, T.; Verhagen, M.; Kuntsche, E.; Scholte, R.H.J.; Engels, R.C.M.E. Social stress in early adolescents’ daily lives: Associations with affect and loneliness. J. Adolesc. 2015, 45, 274–283.
- Campagne, D.M. Stress and perceived social isolation (loneliness). Arch. Gerontol. Geriatr. 2019, 82, 192–199.
- Doane, L.D.; Adam, E.K. Loneliness and cortisol: Momentary, day-to-day, and trait associations. Psychoneuroendocrinology 2010, 35, 430–441.
- Steptoe, A.; Owen, N.; Kunz-Ebrecht, S.R.; Brydon, L. Loneliness and neuroendocrine, cardiovascular, and inflammatory stress responses in middle-aged men and women. Psychoneuroendocrinology 2004, 29, 593–611.
- Hawkley, L.C.; Cole, S.W.; Capitanio, J.P.; Norman, G.J.; Cacioppo, J.T. Effects of social isolation on glucocorticoid regulation in social mammals. Horm. Behav. 2012, 62, 314–323.
- Aguilera, G. HPA axis responsiveness to stress: Implications for healthy aging. Exp. Gerontol. 2011, 46, 90–95.
- Varghese, F.P.; Brown, E.S. The Hypothalamic-Pituitary-Adrenal Axis in Major Depressive Disorder. Prim. Care Companion J. Clin. Psychiatry 2001, 3, 151–155.
- Dunlavey, C.J. Introduction to the Hypothalamic-Pituitary-Adrenal Axis: Healthy and Dysregulated Stress Responses, Developmental Stress and Neurodegeneration. J. Undergrad. Neurosci. Educ. 2018, 16, R59–R60.
- Miller, G.E.; Chen, E.; Zhou, E.S. If it goes up, must it come down? Chronic stress and the hypothalamic-pituitary-adrenocortical axis in humans. Psychol. Bull. 2007, 133, 25–45.
- Loades, M.E.; Chatburn, E.; Higson-Sweeney, N.; Reynolds, S.; Shafran, R.; Brigden, A.; Linney, C.; McManus, M.N.; Borwick, C.; Crawley, E. Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 1218–1239.
- Lara, E.; Moreno-Agostino, D.; Martín-María, N.; Miret, M.; Rico-Uribe, L.A.; Olaya, B.; Cabello, M.; Haro, J.M.; Ayuso-Mateos, J.L. Exploring the effect of loneliness on all-cause mortality: Are there differences between older adults and younger and middle-aged adults? Soc. Sci. Med. 2020, 258, 113087.
- Giné-Garriga, M.; Jerez-Roig, J.; Coll-Planas, L.; Skelton, D.A.; Inzitari, M.; Booth, J.; Souza, D.L. Is loneliness a predictor of the modern geriatric giants? Analysis from the survey of health, ageing, and retirement in Europe. Maturitas 2021, 144, 93–101.
- Beutel, M.E.; Klein, E.M.; Brähler, E.; Reiner, I.; Jünger, C.; Michal, M.; Wiltink, J.; Wild, P.S.; Münzel, T.; Lackner, K.J.; et al. Loneliness in the general population: Prevalence, determinants and relations to mental health. BMC Psychiatry 2017, 17, 113087.
- Noback, M.; Zhang, G.; White, N.; Barrow, J.C.; Carr, G.V. Post-weaning social isolation increases ΔFosB/FosB protein expression in sex-specific patterns in the prelimbic/infralimbic cortex and hippocampus in mice. Neurosci. Lett. 2021, 740, 135423.
- Donovan, M.; Mackey, C.S.; Platt, G.N.; Rounds, J.; Brown, A.N.; Trickey, D.J.; Liu, Y.; Jones, K.M.; Wang, Z. Social isolation alters behavior, the gut-immune-brain axis, and neurochemical circuits in male and female prairie voles. Neurobiol. Stress 2020, 13, 100278.
- Sol, K.; Sharifian, N.; Manly, J.J.; Brickman, A.M.; Zahodne, L.B. Associations Between Loneliness, Reading Ability and Episodic Memory in Non-Hispanic Black and White Older Adults. Arch. Clin. Neuropsychol. 2021.
- Mann, F.; Bone, J.; Lloyd-Evans, B.; Frerichs, J.; Pinfold, V.; Ma, R.; Wang, J.; Johnson, S. A life less lonely: The state of the art in interventions to reduce loneliness in people with mental health problems. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 627–638.
- Masi, C.M.; Chen, H.-Y.; Hawkley, L.C.; Cacioppo, J.T. A Meta-Analysis of Interventions to Reduce Loneliness. Personal. Soc. Psychol. Rev. 2011, 15, 219–266.
- Shvedko, A.V.; Thompson, J.; Greig, C.A.; Whittaker, A.C. Physical Activity Intervention for Loneliness (PAIL) in community-dwelling older adults: Protocol for a feasibility study. Pilot Feasibility Stud. 2018, 4, 187.
- Cohen, G.D.; Perlstein, S.; Chapline, J.; Kelly, J.; Firth, K.M.; Simmens, S. The Impact of Professionally Conducted Cultural Programs on the Physical Health, Mental Health, and Social Functioning of Older Adults. Gerontologist 2006, 46, 726–734.
- Fakoya, O.A.; McCorry, N.K.; Donnelly, M. Loneliness and social isolation interventions for older adults: A scoping review of reviews. BMC Public Health 2020, 20.


