Evidence suggests that chronic exercise can increase upper respiratory tract infections in athletes
[17]. The risk of athletes getting respiratory infections after intense exercise training is 7 times more than inactive individuals and 2 times more than active individuals
[17]. Recurrent infections in athletes can be dangerous during a coronavirus pandemic
[18].
Svenndsen et al.
[19] reported that intense skiing increases the risk of infection by 3 times compared to recreational skiers. Nieman & Wentz
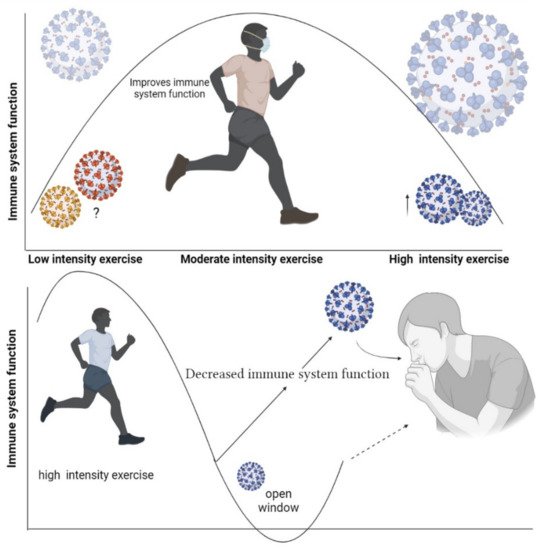
[20] reported that intense physical activity lasting less than 60 min can suppress the immune system. In line with these results, other studies have reported that intense exercise lasting more than 60 to 90 min can suppress immune function
[21][22]. It has also been found that elite athletes who perform intense exercise to prepare for professional competitions may be more susceptible to infectious diseases
[23]. Thus, elite athletes are more prone to URTI during preparation for a professional competition. Being overtired may make this situation worse. Mackinnon et al.
[24] reported that after 4 weeks of high-intensity training in swimmers, 33% of athletes showed symptoms of restlessness and 42% self-reported symptoms of URTI. During intense exercise, the activities of the lymphatic system are disrupted, which can negatively affect the immune system
[25].
Allergic rhinitis is common among athletes due to regular high-intensity exercise
[26]. To prepare for competitions, elite athletes undertake high-intensity training chronically trying to improve their physical fitness. It has been reported that, of 216 Olympic athletes, 56% had a history of conjunctivitis and rhinitis
[26]. Allergic rhinitis impairs physical performance in professional athletes by affecting sleep, decreasing the ability to concentrate, or reducing physical fitness
[26]. Continuous exposure to allergic rhinitis can increase the number of lymphocytes, eosinophils, neutrophils, basophils, and other leukocytes. This can cause the airways to overreact and eventually lead to fibrosis
[27]. Allergens can also stimulate the airway epithelium to release IL-25, IL33, and thymic stromal lymphopoietin (TSLP). These cytokines can activate innate submucosal lymphocytes (ILC2) and release IL-4, IL-5, IL-9, and IL-13
[27], thereby causing airway wall remodeling, bronchial hyperresponsiveness, and goblet cell metaplasia
[27]. These data, along with the open window theory, suggest that elite athletes are at high risk for COVID-19, highlighting the importance of vaccination and health care during infection.
 +1 point
+1 point