Lumbopelvic fixation is used to stabilize the lumbosacral junction in complex clinical situations where standard posterior instrumentation is no longer sufficient. These cases are commonly seen in trauma, tumor involvement, infections, or severe deformity, where structural instability may coexist with neural compression.
Although minimally invasive spinal techniques have expanded significantly in recent years, their use in the lumbopelvic region remains limited. This is largely due to the need for direct access to the sacrum in many of these cases. As a result, open surgery continues to play an essential role when decompression or reconstruction cannot be achieved through percutaneous methods alone.
In this context, a technical note published in the Journal of Clinical Medicine, titled “Lumbopelvic Fixation: How to Be Less Invasive When You Cannot Be Minimally Invasive—A New Subcutaneous Supra-Fascial Approach to Minimize Open Iliac Screwing”, describes a modified method for iliac screw placement that aims to reduce soft tissue disruption while maintaining the principles of standard lumbopelvic reconstruction.
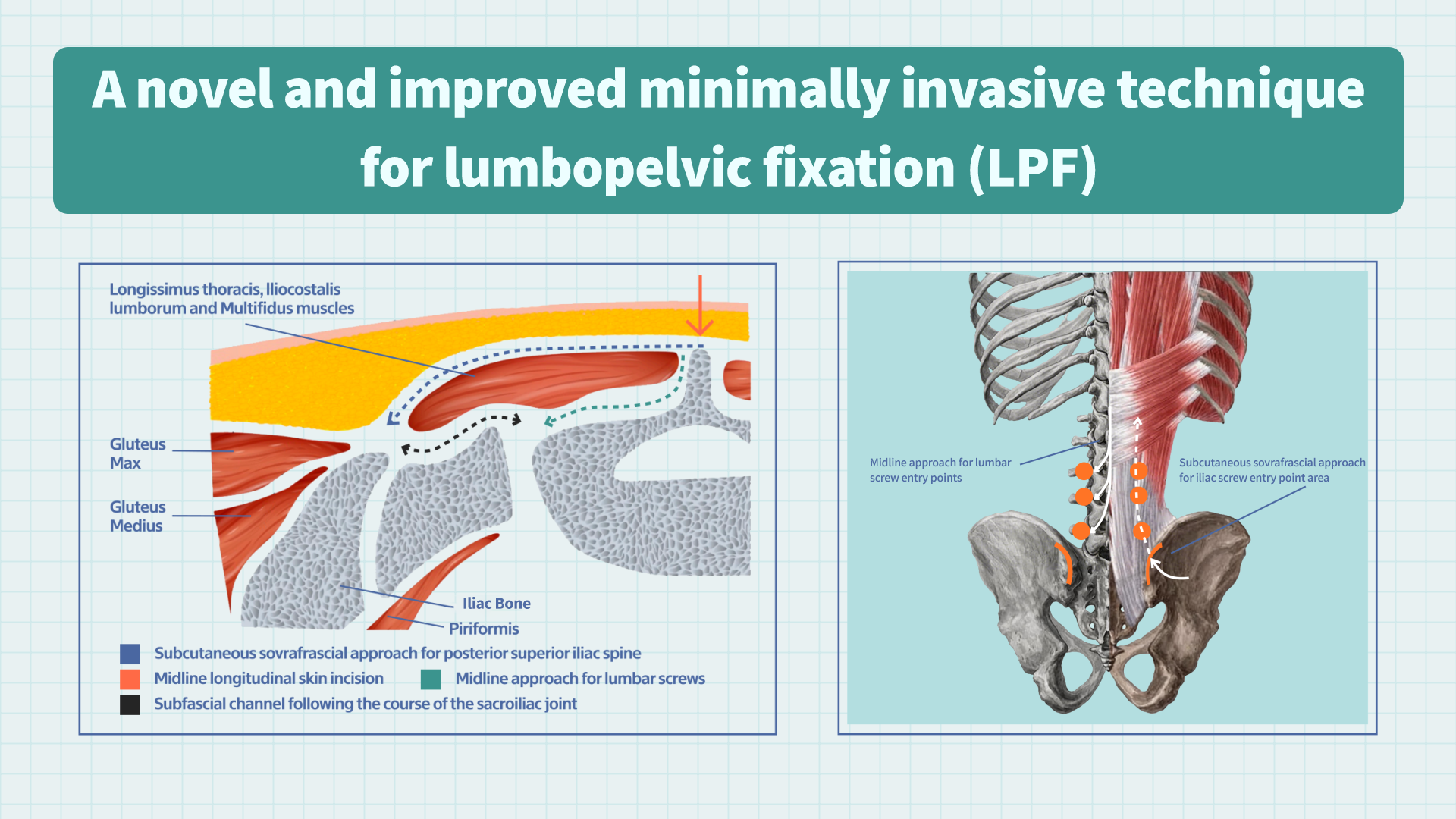
Figure 1. Lumbopelvic Fixation. Produced by MDPI Academic Video Service (Source: https://encyclopedia.pub/video/1788).
1. Clinical Context and Indications
The technique is demonstrated in a clinically complex case involving a 56-year-old female patient diagnosed with metastatic breast carcinoma affecting the sacrum. In this patient, tumor involvement led to significant sacral destruction, accompanied by nerve compression and urinary retention, indicating both mechanical instability and neurological compromise.
In such scenarios, surgical goals typically extend beyond stabilization alone. Decompression of neural elements and partial tumor resection are often required in combination with structural reconstruction of the lumbopelvic junction.
2. Surgical Strategy and Exposure Technique
The procedure was performed using a linear midline incision. Rather than relying on extensive subperiosteal muscle stripping, the authors describe a more controlled subfascial dissection technique. This approach emphasizes preservation of key paraspinal muscles, including the Longissimus thoracis and Iliocostalis lumborum, which are often disrupted in conventional open exposures.
To access the iliac entry point, a subcutaneous supra-fascial corridor is created. This corridor allows instrumentation toward the posterior superior iliac spine while limiting deeper muscular dissection.
Intraoperative CT navigation is used to guide screw placement, particularly important in cases where the exposure is intentionally reduced and anatomical landmarks may be less directly visualized.
A U-shaped cross-link is then applied to complete the construct and enhance overall stability, especially in long-segment reconstructions where rotational control is relevant.
3. Clinical Outcome and Postoperative Course
Following surgery, the patient underwent successful lumbopelvic fixation combined with nerve root decompression and partial tumor resection. No new postoperative neurological deficits were observed.
Over the early postoperative period, the patient showed progressive improvement in sphincter function, suggesting recovery of some degree of neurological function following decompression.
Intraoperative blood loss and soft tissue disruption were reported to be reduced compared with more extensive open dissection approaches.
At six-month follow-up, computed tomography confirmed stable positioning of the lumbopelvic construct. Residual tumor tissue was still present, consistent with the underlying metastatic disease process, but no mechanical failure of fixation was observed.
4. Technical Interpretation
The described approach does not modify the fundamental biomechanics of lumbopelvic fixation. Pedicle and iliac screw constructs continue to function by transferring load from the lumbar spine to the pelvis, effectively bypassing the compromised sacrum.
Instead, the innovation lies in the method of exposure. By combining muscle-preserving dissection, a subcutaneous supra-fascial iliac corridor, and CT navigation, the technique reduces the extent of soft tissue injury required to achieve the same reconstructive goals.
5. Position Within Existing Surgical Strategies
This technique sits within a practical middle ground between conventional open fixation and percutaneous approaches. While minimally invasive techniques aim to reduce exposure entirely, they are not always feasible in cases requiring tumor resection or sacral decompression.
In contrast, traditional open surgery provides full access but at the cost of significant soft tissue disruption. The approach described here represents an attempt to reduce this burden without altering the overall surgical strategy.
6. Broader Clinical Implications
From a clinical perspective, this type of modification reflects an important reality in spine surgery: many complex cases cannot be categorized as purely open or minimally invasive. Instead, surgeons often operate within hybrid conditions where exposure is necessary, but its extent may still be optimized.
In such settings, even modest reductions in muscle dissection and tissue trauma may be clinically meaningful, particularly in patients with oncologic disease who require recovery of neurological function and long-term structural stability.
7. Final Remarks
This report describes a modified subcutaneous supra-fascial approach for iliac screw placement in lumbopelvic fixation performed in the setting of sacral metastasis. The technique combines muscle-preserving dissection, CT-guided instrumentation, and a standardized cross-link construct.
Rather than changing the principles of fixation, it refines how surgical exposure is achieved when open lumbopelvic surgery is unavoidable.