Modern diabetes management is moving from glucose-centred care to precision cardiometabolic risk stratification. Because patients who share the same HbA1c can carry very different cardiovascular, renal, hepatic and metabolic risks, treatment is increasingly guided by clinical phenotype rather than by glucose alone. Drawing on the evidence for GLP-1 receptor agonists and SGLT2 inhibitors, this outcome-centred approach tailors therapy to each patient's dominant risk and targets the long-term outcomes that matter most beyond glycaemic control.

1. The Era of Glucose-Centred Diabetes Care Is Over
For many years, glycated haemoglobin (HbA1c) represented the cornerstone of diabetes management. Achieving glycaemic targets was rightly considered the primary therapeutic goal, because lowering glucose reduces the risk of microvascular complications such as retinopathy, nephropathy and neuropathy. The UK Prospective Diabetes Study established this microvascular benefit decades ago, yet its macrovascular signal emerged only slowly, a reminder that glucose lowering protects small vessels far more readily than it protects the heart. Glucose control alone never fully explained why some patients deteriorated despite excellent HbA1c values, while others remained stable. Cardiovascular outcome trials and contemporary guidelines have since transformed our understanding of the disease. Today, type 2 diabetes is recognised as a complex cardiometabolic disorder in which cardiovascular disease, chronic kidney disease, obesity, metabolic dysfunction-associated steatotic liver disease (MASLD) and heart failure frequently coexist and strongly influence prognosis [1–3].
2. Every Patient Has a Different Cardiometabolic Profile
Two patients may present with an identical HbA1c value while requiring completely different therapeutic strategies. A younger individual living with obesity and MASLD has different priorities from an older patient with chronic kidney disease and a previous myocardial infarction. For this reason, treatment decisions increasingly rely on comprehensive clinical phenotyping rather than on isolated laboratory parameters. Cardiovascular risk, renal function, albuminuria, heart failure, body weight, liver involvement, frailty and life expectancy should all contribute to therapeutic selection. Modern guidelines reflect this by suggesting that the first therapeutic question is no longer simply how high the glucose is, but which organs are most at risk. The same diagnosis, in other words, can describe profoundly different patients, and each profile points towards a different first choice of therapy [1,2].
3. Precision Medicine Has Already Entered Routine Care
Precision medicine is often associated with genomics or advanced molecular profiling. In type 2 diabetes, however, it is already part of everyday practice. The landmark cardiovascular outcome trials made this concrete. In EMPA-REG OUTCOME, the sodium-glucose cotransporter-2 (SGLT2) inhibitor empagliflozin reduced cardiovascular death and heart failure hospitalisation in patients with established cardiovascular disease [4]. In LEADER and SUSTAIN-6, the glucagon-like peptide-1 (GLP-1) receptor agonists liraglutide and semaglutide reduced major cardiovascular events in high-risk patients [5,6]. Importantly, these were not merely glucose-lowering effects: the benefits appeared too early and too consistently to be explained by HbA1c reduction alone, pointing instead to direct cardiac and renal actions. Selecting a GLP-1 receptor agonist when obesity and atherosclerotic risk predominate, or an SGLT2 inhibitor when heart failure or chronic kidney disease is present, is precision medicine in action. The objective is simple: the right treatment, for the right patient, at the right time. This shift from glucose-centred to outcome-centred medicine is summarised in Figure 1 [1–6].
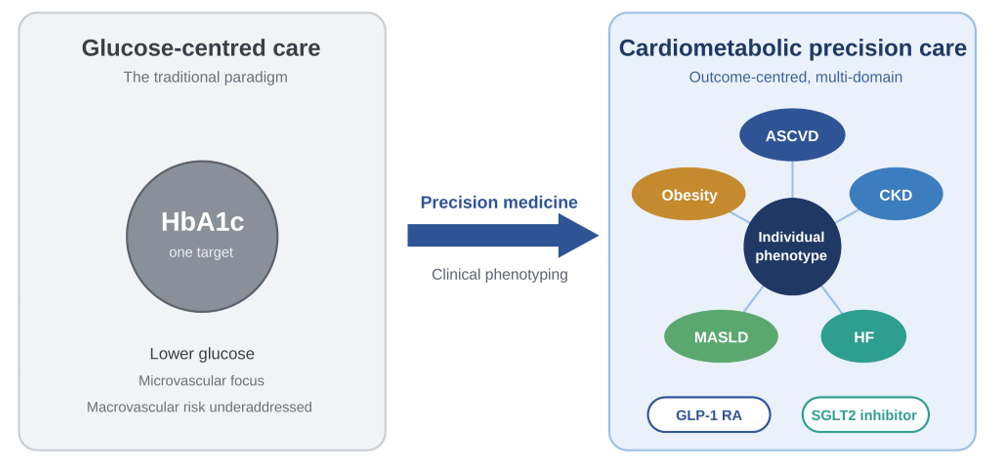
Figure 1. From traditional glucose-centred diabetes care to precision cardiometabolic medicine. ASCVD: atherosclerotic cardiovascular disease; CKD: chronic kidney disease; HF: heart failure; MASLD: metabolic dysfunction-associated steatotic liver disease.
4. Residual Cardiometabolic Risk: What HbA1c Does Not Capture
Even when glycaemic targets are met, a substantial burden of risk often remains. This residual cardiometabolic risk is driven by factors that HbA1c simply does not measure: persistent albuminuria, visceral adiposity, atherogenic dyslipidaemia, subclinical heart failure and ongoing kidney decline. Recognising it has reframed the therapeutic goal from normalising a single number to protecting the organs most likely to fail. The DAPA-HF trial, for example, showed that dapagliflozin reduced worsening heart failure and cardiovascular death even in patients without diabetes [7], while FLOW demonstrated that semaglutide slowed kidney disease progression in patients with diabetes and chronic kidney disease [8]. The benefit, in these settings, is no longer about glucose at all.
5. The Next Frontier: Integrated Cardiometabolic Risk
Future diabetes care will depend on integrating multiple clinical domains into a single decision-making framework. Digital health technologies, artificial intelligence, continuous glucose monitoring and electronic health records may help clinicians identify high-risk phenotypes and select personalised strategies, flagging, for instance, the patient whose declining estimated glomerular filtration rate and rising albuminuria warrant earlier organ protection. Used well, such systems could shorten the gap between a worsening trajectory and the moment a protective therapy is actually started. These tools are not intended to replace clinical judgement, but to enhance it through more efficient interpretation of increasingly complex information. The challenge will be to transform data into decisions that are clinically meaningful, feasible and centred on the individual patient [8–10].
6. Looking Beyond HbA1c
The success of modern diabetes care should no longer be measured exclusively by lower HbA1c values. Preserving kidney function, reducing cardiovascular events, preventing heart failure, improving metabolic health and addressing obesity have become equally important therapeutic objectives. The evidence now extends beyond diabetes itself: in SELECT, semaglutide reduced cardiovascular events in people with obesity but without diabetes, underlining how far the field has moved from a purely glucose-centred view [9]. Precision medicine is therefore not a distant aspiration, but the natural evolution of evidence-based diabetes care. As therapies continue to expand and risk assessment becomes more sophisticated, clinicians will be increasingly able to deliver personalised cardiometabolic care focused on the outcomes that matter most to patients.
References
- American Diabetes Association Professional Practice Committee. Standards of Care in Diabetes—2025. Diabetes Care. 2025, 48, S1–S350.
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; et al. Management of hyperglycaemia in type 2 diabetes, 2022. A consensus report by the ADA and EASD. Diabetologia. 2022, 65, 1925–1966.
- Marx, N.; Federici, M.; Schütt, K.; Müller-Wieland, D.; Ajjan, R.A.; Antunes, M.J.; Christodorescu, R.M.; Crawford, C.; et al. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes. Eur. Heart J. 2023, 44, 4043–4140.
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N. Engl. J. Med. 2015, 373, 2117–2128.
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.E.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N. Engl. J. Med. 2016, 375, 311–322.
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jodár, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N. Engl. J. Med. 2016, 375, 1834–1844.
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N. Engl. J. Med. 2019, 381, 1995–2008.
- Perkovic, V.; Tuttle, K.R.; Rossing, P.; Mahaffey, K.W.; Mann, J.F.E.; Bakris, G.; Baeres, F.M.M.; Idorn, T.; et al. Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes. N. Engl. J. Med. 2024, 391, 109–121.
- Lincoff, A.M.; Brown-Frandsen, K.; Colhoun, H.M.; Deanfield, J.; Emerson, S.S.; Esbjerg, S.; Hardt-Lindberg, S.; Hovingh, G.K.; et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N. Engl. J. Med. 2023, 389, 2221–2232.
- Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group. KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2022, 102, S1–S127.
Biography
Antonio Maria Labate, MD, is a specialist in Internal Medicine working as an outpatient diabetology and internal medicine specialist at ASST Franciacorta and ASST Mantova, in Lombardy, Italy. He trained in Internal Medicine at the University of Messina and has broad clinical experience spanning internal medicine, emergency medicine and diabetology. His work focuses on clinical diabetology, cardiovascular and cardiometabolic risk in type 2 diabetes, real-world evidence, and the clinical use of newer glucose-lowering therapies such as GLP-1 receptor agonists and SGLT2 inhibitors. He has authored peer-reviewed articles and congress communications on the cardiovascular, renal and metabolic effects of these agents, and serves as a reviewer for several international journals.
