Table 1. PICOS criteria for inclusion of studies.
| Parameter |
Criterion |
| Population |
Human adults (≥18 years) |
| Interventions/exposures |
Diet supplementation with buckwheat, rutin, quercetin and/or other buckwheat related bioactives |
| Comparisons |
Placebo, no buckwheat or other comparison |
| Outcomes |
Serum lipid profile, type 2 diabetes and glucose homeostasis parameters, inflammatory and oxidative stress markers, body morphology parameters, blood pressure, all-cause and cardiovascular mortality, cardiovascular disease severity and/or clinical progression, markers of vasoconstriction/vasodilatation and/or markers of atherosclerosis, such as atherosclerotic plaque, arterial wall thickness, coronary artery calcification, intima media thickness, etc. |
| Study design |
Prospective cohort studies, case-cohort, nested-case control studies, randomized and non-randomized clinical trials |
2. Discussion
Evidence on exposure–outcome relationships can be inferred from many types of studies, including RCTs, cohort studies, case-control studies, cross-sectional analyses, ecological studies and animal studies. Each study type has characteristic strengths and weaknesses. For example, RCTs are the most robust method for dealing with confounding, but they are often conducted with strict inclusion and exclusion criteria, meaning that trial participants may be unlikely to be fully representative of the general population, as well as being carried out over relatively short durations.
Case-control studies are well suited for understanding the risks linked to rare outcomes, but they may be subject to recall bias for past exposure. Animal studies are widely used in evaluating the risks of consumer products and environmental risks but may not be generalizable to humans. Study design and analysis impacts causal interpretation and understanding of the results.
In our work, we took this fact into account and applied a stricter methodological rigor, differentiating study designs, as well as conducting a more structured evaluation of BW and cardiometabolic health. To the best of our knowledge, this review contains the largest number of human intervention studies to date, i.e., with three additional studies in the meta-analysis compared to the aforementioned review. Furthermore, it important to consider within-subject correlation in pre-post analysis, as failure to do so can lead to meta-analysis with misleading statistical results and inherent biases. To address this. we have used a coefficient of 0.8 in the calculations for the standard deviation of the mean difference [
8].
Moreover, there are other reports that have attempted to ascertain the potential health benefits of consuming BW as a food, supplement, remedy or possible pharmaceutical agent. Recent work has focused on BW’s role in health and disease, especially investigating effects on lipid profile, BP, glucose and body weight, but the majority of these claimed effects in the literature are based on data extrapolated from in vitro studies or animal models [
6,
7].
Although animal models are vital in understanding physiological mechanisms and elucidating the potential health relevance, human intervention studies are scarce and inconsistent in supporting BW benefits identified in nonhuman studies. In the literature, a cross-sectional study with a questionnaire-based assessment of oat and buckwheat intakes showed a significant reduction in both systolic (−3.1 mm Hg,
p < 0.001) and diastolic (−1.3 mm Hg,
p < 0.01) BP [
34]. Due to the study design (i.e., cross-sectional), this survey was not included in our analysis. Nevertheless, it is worth mentioning that the authors highlighted that water-soluble fiber but not total dietary fiber was independently associated with BP. Hence, a possibility exists that there is an effect of BW on these parameters, since BW has higher levels of soluble than insoluble fiber. Only two cross-sectional studies [
34,
35] have suggested that consumption of BW seeds may be a preventative factor for hypertension, dyslipidemia and hyperglycemia. However, the inherent limitations of a cross-sectional design render these findings indicative.
There are some results on the role of
Tatary BW in human nutrition, showing that foods made from grain components of
Tartary BW may have preventive effects against several chronic diseases, including obesity, CVDs, gallstone formation and hypertension [
36]. However, these findings are almost entirely based on in vitro and nonhuman models, with little relevance to human health. Additionally, such effects are hypothetically attributed to resistant starch, protein, and phenolic substances in the grain, and to the interactions among these constituents, without any methodological high-quality study design in humans supporting these claims. Of note, in the systematic review part of our report, several studies used
Tatary BW as intervention [
21,
22,
23,
25,
26,
27].
Results were not consistent with regards to effect of
Tatary BW on CVD markers and study designs were very heterogeneous, with little, if any, considerations on compliance with the BW intervention, including no control arm or head-to-head comparison drugs. In our review, a consistent finding that aligns with previous reviews on BW [
2,
37], is the fact that many of the studies on BW were published before 2010, indicating an additional complexity with regards to methodological and technical procedures used. This aspect warrants further exploration, but it is a reminder that additional caution should be exercised when interpreting the literature on BW with considerations of separation, extraction, formulation, and processing methods.
Another observation is that BW is commonly a basis for noodle recipes in Asia. However, in Europe, BW flour is used in pancakes and crepes, as a common ingredient in gluten-free products, to which coeliac patients are particularly exposed. With such a wide use of BW at population level, it is reasonable to assume that the borderline effect of BW interventions on total and HDL cholesterol warrants further investigation, regardless of the questionable methodological rigor of evidence so far. According to BW’s degree of processing and food matrix, the primary mechanism of action may differ, but we speculate that this mechanism may include slower gastric emptying, the inhibition of hepatic cholesterol synthesis and/or enhanced fecal excretion of cholesterol and bile salts (see Figure 1).
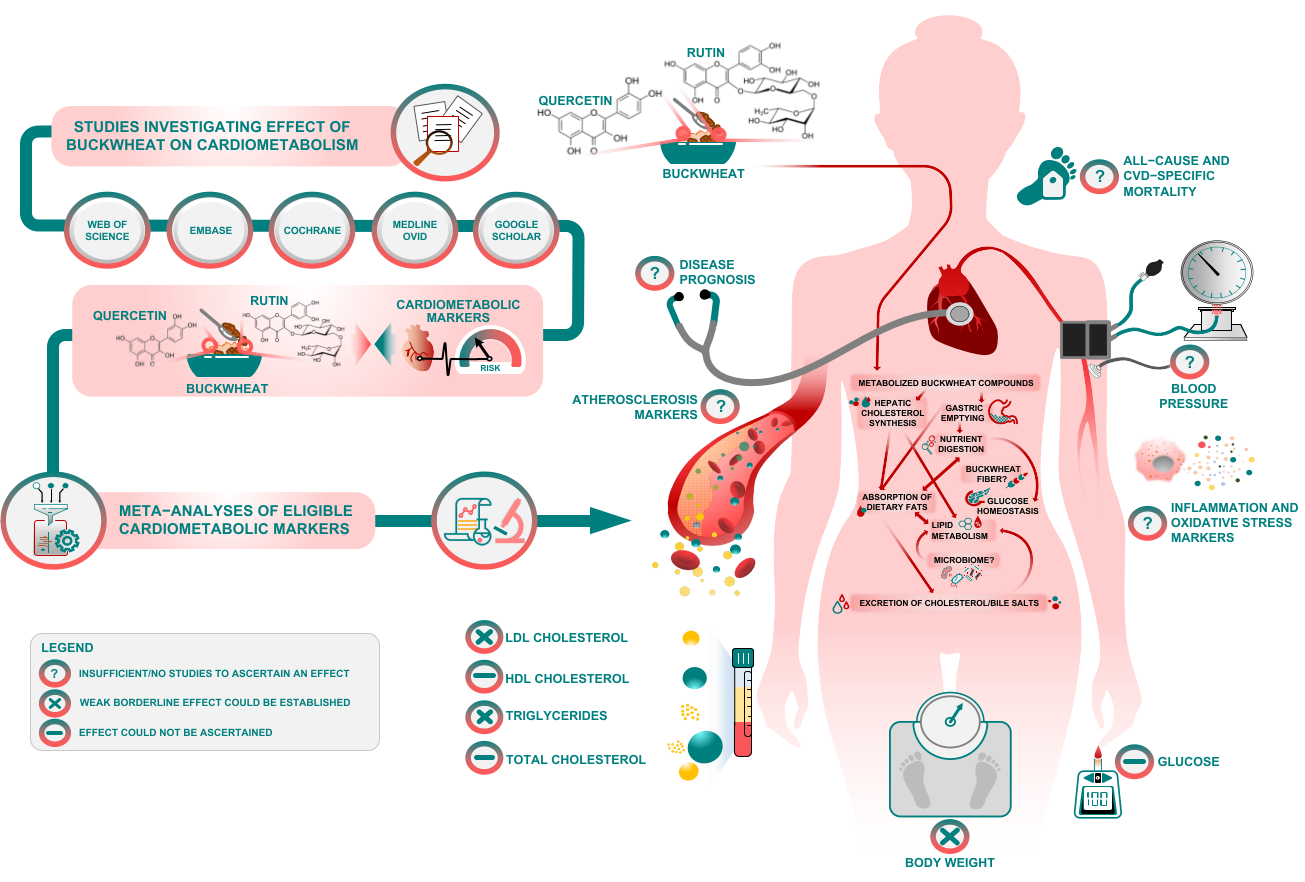 Figure 1.
Figure 1. Visual summary, mechanisms and potential avenues for future research.
Similar effects have been observed from dietary fibers in general [
38] and it is not possible to differentiate the effect of quercetin or rutin from the effects of fibers present in BW. Nevertheless, the gel-forming attributes of soluble fibers in BW may be a basis for the borderline effect on some of lipids and glucose [
39,
40,
41]. It is not clear whether different types of BW supplementation (e.g., grain vs. non-grain components) may have physiologically different effects on health. Herbal supplementation from non-grain components could be a richer source of natural phytochemicals, but this area of BW research remains speculative and to be elucidated in the future.
Processing can also influence the BW matrix and its composition. It may be the case that a single compound (i.e., rutin or quercetin) can influence several physiological functions, but also several BW compounds may affect a single defined physiological mechanism.
Processing, such as the type that disrupts the food matrix, may indirectly influence digestibility and/or bioavailability of BW nutrients, but can also degrade functionality by altering the structure of its components (e.g., depolymerisation of rutin or quercetin, lipid coalescence or protein denaturation) and/or their interaction. This warrants further research to confirm the specific effects and the mechanisms involved.
Over the past five decades, there have been efforts to document and establish health benefits from BW [
5,
6,
7,
36]. Despite its potential to improve human health, BW remains understudied in nutrition and clinical settings. Although the bioactive components present in BW are implicated in beneficial human health effects, future studies should focus on how insufficiently studied BW phytocompounds (such as phenolic acids and polyphenols) are metabolized in humans and influence cardiometabolic health. Thus, findings from this systematic review and meta-analysis might help guide future research to explore the potential health-promoting components of BW, which in turn will shed light on any health benefit this crop may deliver and its potential to be incorporated into human diet for optimal health.
Although our report is the largest review of RCTs and human interventional studies to date, concerns about the scarcity of studies, heterogeneity and methodological rigor concerns undermine establishment of causal inferences. The available interventional studies on BW have multiple limitations and flaws regarding sample size, intervention/follow-up time, confounders, blinding, randomization and allocation issues, which reinforce the need for more and better trials on the topic. In spite of the sensitivity analyses we performed to address limitations of the available evidence base, caution should be paid in interpreting some results as pooled studies had differing health characteristics. This constrains strong casual inferences and generalizability of findings, but we believe it can further stimulate the exploration of BW phytochemicals and their role(s) in human health. In addition, for crossover designs we used data collected from the first period only. Future studies should explore further interactions of BW bioactive components with health (Figure 1).