Obesity is defined as an elevation of the fat tissue mass in the body, which is not limited to any age group. It is characterized by increased body and fat mass, hormonal disturbances, food intake (eating pattern), and genetic factors [
1]. Obesity is a significant contributor to the global burden of several chronic diseases such as diabetes mellitus type 2, cardiovascular diseases, asthma, etc., which affect the human body. It has been proclaimed a global pandemic with a death rate of approximately 2.8 million people annually [
2,
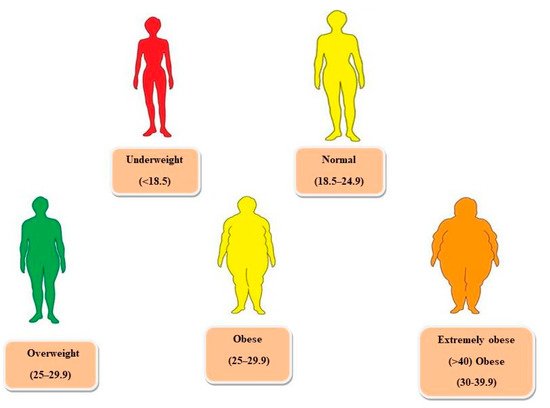
3]. Since fat is present all over the body, it is not possible to measure it directly. Therefore, body mass index (BMI) is used to observe the relationship between weight and height. Whereas waist circumference, waist/hip ratio, skinfold thickness, and bioimpedance help to assess obesity and overweight [
4].
There are two types of fats, visceral and subcutaneous. The fat deposited over visceral organs such as the kidney, abdomen, liver, intestines, heart, and pancreas is known as visceral fat. The other name for visceral fat is active fat because research has proved that it significantly affects our hormonal activity, resulting in metabolic syndrome and insulin resistance. The hormonal activity influences metabolism, body fat distribution, and appetite [
7]. Moreover, the fat underneath the skin is known as subcutaneous fat and can be felt underarm and legs [
8]. The body attains two types of shapes, apple, and pear, due to fat deposition in certain body areas [
9]. In the case of an apple shape (Android), fat accumulation occurs in the upper area of the waist and abdomen. Some deposition also appears on the neck, arms, and shoulders. The main reason behind this body shape is visceral fat, which is associated with the health risk of type 2 diabetes [
10]. In the pear shape (Gynoid), fat deposition occurs on the thighs and buttocks. The amount of visceral fat is low in this type of body shape, resulting in low chances of weight-related diseases [
11].
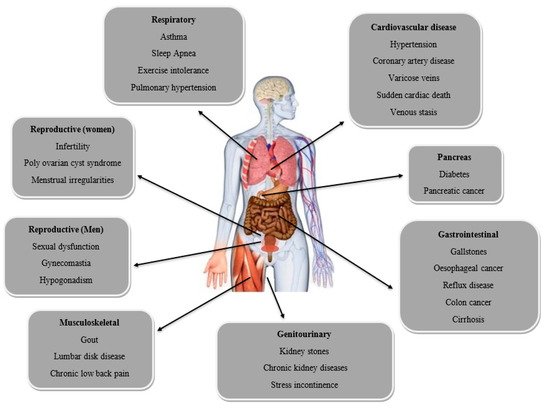
Obesity also causes several complications such as reproductive (women and men), respiratory, cardiovascular diseases, pancreas, and gastrointestinal, as shown in Figure 2.
2. Hormones Related to Obesity
2.1. Leptin
Leptin is a significant hormone that is related to an increase in body weight [
20]. Leptin, the result of the ob (obese) gene product, is the first adipose hormone that links the central regulation of metabolism with peripheral adipose fat mass. In the arcuate nucleus of the hypothalamus, leptin suppresses appetite by either decreasing the activity of orexigenic neuropeptides (NPY and AgRP) or boosting the activity of anorexigenic neuropeptides (α-MSH and CART) [
21,
22]. As adiposity increases, serum leptin concentrations increases along with it. Higher circulating levels of leptin reduce energy intake and increase energy expenditure in a homeostatic system, but this is not the case in those who are suffering from obesity or overweight, thus, indicating a condition of leptin resistance. Circulating soluble leptin receptor (SLR) levels decline with obesity. These receptors are blood-circulating proteins that directly support leptin activity. This combination of high levels of leptin and low SLR may contribute to the leptin resistance seen in obese people [
7]. Clinical investigations have demonstrated that the administration of leptin has minimal effect on the body weight of obese participants, despite enthusiastic research on the use of leptin in the treatment of obesity [
21,
22]. If there is a deficiency of leptin, it can lead to extreme obesity [
23].
2.2. Ghrelin
A 28-amino acid peptide hormone called ghrelin is mainly produced in the stomach. Ghrelin increases the growth hormone release by directly interacting with the GH secretagogue receptor at the pituitary level [
24,
25]. Ghrelin seems to have a role in neuroendocrine and metabolic responses to food intake. Its circulating levels are elevated in anorexia and cachexia and lowered in obesity [
26,
27,
28]. Plasma ghrelin levels are inversely related to body fat mass, body mass index, plasma leptin levels, insulin, and glucose levels [
29]. Various studies imply that ghrelin may be crucial in controlling appetite and weight. GH secretion, food intake, and obesity are all controlled by the GH secretagogue receptor (GHS-R1a) in the arcuate nucleus [
30,
31].
2.3. Insulin
Excess body weight is frequently linked to insulin resistance, a condition in which tissues, particularly skeletal muscle, the liver, and adipose tissue, are less receptive to the physiological effects of insulin [
32,
33]. Plasma insulin levels are persistently increased in insulin-resistant conditions, even while fasting. Increased plasma concentrations of free fatty acids, continually produced from adipose tissue, are the leading cause of insulin resistance by excess weight. Increased hepatic and muscle fatty acid absorption and oxidation due to increased free fatty acid concentrations result in metabolic changes that reduce these tissues’ ability to absorb and utilize glucose for energy metabolism. Reduced insulin receptor levels and post-receptor abnormalities in insulin signaling are included in these adaptations. Increases in intra-abdominal body fat storage, which release free fatty acids into the circulation more quickly than other adipose tissue compartments, are most significantly associated with insulin resistance [
34,
35,
36]. Weight reduction often increases insulin sensitivity and normalizes plasma insulin concentrations in obese patients [
37].
2.4. Adiponectin
Mature adipocytes release adiponectin, and its circulating levels are lower in obese and diabetic people. The plasma level of adiponectin is increased by anti-diabetic and anti-obesity medications such PPARagonists (thiazolidinediones) and CB1 antagonists (rimonabant). Through the activation of AMP kinases, which have been linked with the adiponectin receptors R1 and R2 in animal models and human studies, adiponectin increases insulin sensitivity [
38,
39]. In humans, atherosclerosis, dyslipidemia, and insulin resistance have been linked to lower adiponectin levels in obesity. With an increase in insulin sensitivity, plasma adiponectin levels considerably rise with weight reduction [
7]. As a result, treating insulin resistance associated with obesity and type 2 diabetes may include targeting adiponectin and adiponectin receptors.
3. Synthetic Drugs
Many anti-obesity synthetic drugs such as orlistat, lorcaserin, phentermine/topiramate, bupropion/naltrexone, and liraglutide are already available on the market. These drugs target obesity by increasing noradrenaline, dopamine, and serotonin. However, they have many side effects related to cardiovascular health, increased blood pressure, and affect the central nervous system by causing changes in sleep patterns and affecting hormonal secretion [
47,
48].
3.1. Orlistat
Orlistat, approved in 1998, is a synthetic derivative of lipstatin [
49], a potent and reversible inhibitor of gastrointestinal lipase that inhibits pancreatic and stomach lipase to reduce dietary fat absorption by 30% [
50]. Orlistat was produced as one of the lipstatin analogs and is known as an anti-obesity medication due to its ability to suppress pancreatic lipase activity selectively. Orlistat works by reducing fat absorption by permanently inhibiting lipase activity in the gastrointestinal tract, which reduces energy intake [
49]. The most common side effects include diarrhea, abdominal pain, bloating, flatulence, oily stools, dyspepsia, reduced absorption of fat-soluble vitamins, and in some rare cases, it can cause severe liver and kidney injury [
50].
3.2. Lorcaserin
Lorcaserin, approved in 2012 in the USA, is a selective serotonin 2C (5-HT2C) receptor agonist that decreases body weight by reducing food intake [
50]. Serotonin (5-HT) is released when lorcaserin interacts with the 5-hydroxytryptamine 2C (5-HT2C) receptor, and serotonin uptake is subsequently inhibited [
51]. Because lorcaserin has a low specificity for the 5-HT2B receptor (about 100 times lower than that of the 5-HT2C receptor), there is a limited chance that long-term use of lorcaserin may result in heart-valve abnormalities [
6,
52]. The side effects of lorcaserin include serotonin syndrome or neuroleptic malignant syndrome-like reactions: headache, dizziness, nausea, fatigue, dry mouth, constipation, low blood sugar (hypoglycemia), headache, cough, back pain, and fatigue in diabetic patients [
53].
3.3. Phentermine/Extended-Release Topiramate (Qnexa)
A combination treatment of phentermine and extended-release (ER) topiramate, developed by Vivus, is known as Qnexa. Although the exact mode of action is unknown, phentermine is believed to stimulate the release of catecholamines (including dopamine and noradrenaline) in the hypothalamus. In contrast, topiramate enhances the activity of the neurotransmitter gamma-aminobutyrate, regulates voltage-gated ion channels, and inhibits carbonic anhydrase and AMPA/kainite excitatory glutamate receptors [
54,
55]. The side effects reported include dizziness, paresthesia (tingling in the hands and feet), changed taste perception, dry mouth, dysgeusia, insomnia, and constipation, without increased risk of serious cardiovascular problems [
55].
3.4. Bupropion/Naltrexone (Contrave)
The combination of bupropion and naltrexone synergistically enhances neuronal activity and decreases food uptake by stimulating satiety [
49]. Although bupropion is a relatively poor inhibitor of dopamine and norepinephrine uptake, it stimulates the hypothalamic pro-opiomelanocortin (POMC) system, which activates melanocortin receptors and induces weight reduction through appetite suppression and increased energy expenditure. Naltrexone functions as an antagonist of the opioid receptor that generally causes a negative feedback-mediated inhibition of POMC activation and thus acts synergistically to prolong the bupropion’s action on metabolism [
56]. The most common adverse effects (AEs) reported are nausea, headache, dizziness, vomiting, insomnia, constipation, and dry mouth [
57].
3.5. Liraglutide
An analog of glucagon-like peptide (GLP)-1, liraglutide has a half-life of 13 h, which significantly prolongs its activation of the GLP-1 receptor (the half-life of native GLP-1 is about 1.5 min), increasing stimulation of glucose-dependent insulin secretion and exerting a more substantial effect on glucagon suppression [
58]. Native GLP-1 has central effects that control appetite and feeding centers in the brain [
59]; hence, liraglutide may potentially have the ability to influence energy intake. A 5-week partial crossover trial with liraglutide demonstrated that liraglutide caused weight reduction most likely mediated by lowering appetite and decreasing food consumption. It did not enhance energy expenditure, as measured by appetite scores, post-prandial satiety, and fullness ratings [
60]. The most common side effects reported include nausea, diarrhea, vomiting, constipation, decreased appetite, and low blood sugar (hypoglycemia) [
61].
4. Herbs That Control Obesity
Herbs have always proved to be an essential and functional source for many chronic diseases, and obesity is one of them. Other than a few allergic reactions in susceptible individuals, herbs have fewer adverse effects than single-compound drugs. Medicinal herbs such as
Nigella sativa,
Hibiscus sabdariffa,
Ilex paraguariensis,
Coffea arabica,
Caralluma fimbriata,
Panax ginseng, and many others have shown positive effects on obesity by different mechanisms such as suppressing appetite; reducing triglyceride levels; increasing the metabolic rate; inhibiting pancreatic lipase, etc. Hence, they facilitate the process of weight loss [
62,
63].
4.1. Nigella sativa
The herb is a member of the Ranunculaceae family, also known as black seed. The origin of the herb belongs to south European countries, including Albania, Bosnia, Bulgaria, and Cyprus, as well as some southwest Asian countries such as Indonesia, Thailand, and Singapore. It is also grown in India, Pakistan, Turkey, and Syria [
64,
65]. The herb contains vitamins and minerals such as copper, potassium, zinc, and iron [
66]. It treats various diseases and disorders related to liver, cardiovascular health, inflammation, gastrointestinal health, and diabetes. It has antioxidant, anti-inflammatory, anti-bacterial, and anti-fungal properties [
67,
68]. The herb is a potent anti-obesity agent. The main bioactive compound, Thymoquinone (TQ), is mainly responsible for anti-obesity activity. It targets obesity by suppressing the appetite and reducing triglyceride levels. It also plays a significant role in adiponectin hormone level, which plays a vital role in protecting against insulin obstinacy in the body [
69,
70].
4.2. Hibiscus sabdariffa
The other name for the herb is roselle; it is a sub-shrub that can grow up to 8 ft in height. It is a native plant of India and Malaysia but is grown in other parts of the world, such as China, Thailand, Sudan, Nigeria, Jamaica, etc. [
71,
72]. It is a vital source of vitamins and minerals such as calcium, iron, phosphorus, riboflavin, and vitamin C.
Hibiscus sabdariffa helps to fight against many diseases related to kidney stones, gastrointestinal disorders, and liver damage. It has antioxidant, antimicrobial, anti-inflammatory, anti-carcinogenic, anti-obesity, and anti-diabetic properties [
73]. The main bioactive compounds, such as anthocyanins, flavonoids, and organic acids, are responsible for the anti-obesity activity of the herb [
74]. The extract of
Hibiscus sabdariffa has the potential to enhance insulin sensitivity and resistance while lowering lipid accumulation and oxidative stress. An increase in lipoprotein lipase activity and a decrease in the expression of the adipogenesis genes are two ways that anthocyanin suppresses lipid accumulation and decreases fat mass in high-fat diet-induced obese rats. The loss of visceral adipose tissue reduces inflammatory cytokines and oxidative state, which reduces insulin resistance and enhances insulin sensitivity in obese rats [
75].
4.3. Ilex paraguariensis
The herb’s common name is yerba mate; it belongs to the
Aquifoliaceae family. It is a native plant of South America (Brazil, Argentina, etc.) [
76]. The height of the plant can be up to 20 m. It is one of the richest sources of flavonoids (quercetin and rutin) and phenolic acids such as chlorogenic and caffeic acid. It also contains saponins and caffeine. It has many pharmacological properties such as antioxidant activity, anti-obesity, anti-diabetic, anti-tumor, neuroprotective, and anti-inflammatory [
77]. It helps in the regulation of insulin as well as targets obesity by inhibiting the expression of genes that regulate adipogenesis, improve the lipid profile, and act as an appetite suppressant. It also inhibits the inflammatory action in adipose tissue caused by obesity. It enhances peripheral insulin sensitivity [
78] and modulates the leptin release by adipose tissue [
79].
4.4. Rosmarinus officinalis
The other name of the herb is rosemary; it belongs to
Lamiaceae Mint family. The herb is native to the Mediterranean region. The leaves are a vital part of the herb used for medicinal purposes [
80]. Anti-bacterial, antioxidant, anti-cancer, anti-diabetic, anti-inflammatory, anti-thrombotic, neuroprotective, and hepatoprotective are some of the herb’s uses [
81]. It also has an anti-viral effect and helps to regulate blood pressure [
82,
83]. Certain studies revealed a significant anti-obesity impact with the help of carnosic acids that alter the activity of 3T3-L1 preadipocytes differentiation [
84,
85]. Evidence of the inhibitory effect of rosemary extract on pancreatic lipase activity, a crucial enzyme in the digestion and absorption of fat, as well as on gastric lipase activity, suggests that limiting lipid absorption is the primary mechanism by which rosemary extract lowered weight gain and adiposity index [
86].