Ferroptosis is a new type of cell death caused by lipid peroxidation due to iron metabolism disorders and ROS accumulation. It is different from other regulated cell death (RCD), such as apoptosis, autophagy and pyroptosis, in morphology and mechanisms. Morphologically, ferroptosis is neither featured with typical apoptotic features, such as chromatin agglutination and apoptotic body formation, nor the formation of autophagic vacuoles, unique autophagy features or the release of proinflammatory factors, which is a typical feature of pyroptosis; instead, ferroptotic cells mainly manifest as shrunken mitochondria with increased membrane density and disappeared mitochondrial cristae [
4,
5]. Mechanistically, although other RCDs can also be triggered by ROS overload [
6], ferroptosis is always accompanied by significant iron accumulation, glutathione (GSH) depletion, and changes in genes related to iron homeostasis and lipid metabolism [
7]. Polyunsaturated fatty acid (PUFA) is the source of ferroptosis. PUFAs participate in the synthesis of membrane phospholipids catalyzed by acyl-CoA synthetase long-chain family member 4 (ACSL4) and lysophosphatidylcholine acyltransferase 3 (LPCAT3) [
8,
9], then cytochrome P450 oxidoreductase (POR) and lipoxygenases (LOX) will oxidize polyunsaturated phospholipids (PUFA-PL) to lipid peroxides (L-OOH) [
10,
11,
12]. Normally, on the one hand, the cytotoxic L-OOH can be reduced to the corresponding alcohols by glutathione peroxidase (GPX4) [
13]. On the other hand, it can be converted into L-OO
. through Fenton reaction, while L-OO
. can be reduced by ubiquinol (CoQH2) to protect cells from lipid peroxidation [
14,
15]. However, when Fe
2+ or PUFA is overloaded or the antioxidant system is imbalanced, L-OO
. will accumulate in large quantities, resulting in lipid peroxidation of membrane phospholipids, and ultimately lead to ferroptosis [
7]. Cystine/glutamate antiporter solute carrier family 7 member 11 (SLC7A11; also known as xCT) is a key factor regulating ferroptosis. It controls the synthesis of GSH, which allows GPX4 to reduce L-OOH [
16]. Furthermore, tetrahydrobiopterin (BH4) and ferroptosis suppressor protein 1 (FSP1) also play an important role in inhibiting ferroptosis by producing CoQH2 [
14,
17]. In addition, with the increasing research on ferroptosis, it has been found that it plays an important role in the process of cell death caused by radiation. Lang et al. found that radiation can activate the ataxia-telangiectasia mutated gene (ATM) and inhibit the expression of SLC7A11, thereby promoting ferroptosis [
18]. Moreover, Lei et al. verified this view and found that ionizing radiation (IR) significantly increased the staining of C11-BODIPY and 4-hydroxynonenal (4-HNE) in tumor cells, thus causing typical morphological changes in ferroptosis [
19]. Further studies have shown that ferroptosis inducers such as sulfasalazine, ras-selective lethal small molecule 3 (RSL-3), and cyst(e)inases have an obvious effect on radiation sensitization; such sensitization is mainly related to ROS accumulation and lipid peroxidation [
18].
2. Hypoxia Protects Tumor Cells from Ferroptosis by Regulating Iron Homeostasis
Hypoxia has been recognized as one of the basic and important characteristics of solid tumors; it plays an important role in various physiological events, such as cell proliferation, angiogenesis, metabolism, tumor invasion, and metastasis [
22]. HIF-1 is a key regulator of hypoxia response in tumor cells and plays a key role in the adaptation of tumor cells to the hypoxic microenvironment. Hypoxia and HIF-1 overexpression are associated with radiation and chemotherapy resistance, as well as poor clinical prognosis of solid tumors [
22,
23]. Radiation resistance caused by hypoxia is considered to be the main reason why radiation therapy for solid tumors fails to achieve the expected results. Different mechanisms have been proposed to explain radiation resistance caused by hypoxia, among which the oxygen fixation hypothesis is the most accepted [
24]. In addition, the upregulation of HIF-1α and enhancement of antioxidant system activity caused by hypoxia are also considered to be important factors for radiation resistance [
3,
20]. Interestingly, recent studies have shown that hypoxia can protect tumor cells from ferroptosis [
25], which may explain the poor prognosis of hypoxic tumors.
In the body, cellular iron is essential for maintaining various metabolic pathways. Excessive free iron (Fe
3+ or Fe
2+) may lead to oxidative damage and cell death [
26]. In addition, intracellular free iron can induce ferroptosis by activating arachidonate lipoxygenases (ALOXs) and promoting ROS production [
4,
27]. Therefore, the maintenance of iron homeostasis plays a crucial role in cell development; ferritin plays the most important role in regulating intracellular iron homeostasis. Ferritin heavy chain (FTH), ferritin light chain (FTL), and mitochondrial ferritin (FTMT) are three known ferritin proteins that have ferroxidase activity which can store Fe
3+ and reduce intracellular free Fe
2+ levels [
28], thus playing an important role in ferroptosis. The release of iron in ferritin is regulated by the process of ferritinophagy; nuclear receptor coactivator 4 (NCOA4), its main regulator, directly binds to FTH and transports the complex to the lysosome for degradation [
29]. The results of Fuhrmann et al. demonstrated that under hypoxic conditions, the transcription rate of NCOA4 decreases, leading to an increased FTH and FTMT expression, which protects cells from ferroptosis [
25] (
Figure 1). Subsequently, this was verified in diabetic mice, osteoporotic mice, and other animal models [
30,
31]. Furthermore, it was proven that the downregulation of NCOA4 and inhibition of ferroptosis under hypoxic conditions were associated with poor prognosis of stomach adenocarcinoma and hepatocellular carcinoma [
32,
33]. In conclusion, hypoxia represses ferritinophagy-mediated ferroptosis and leads to unfavorable prognosis; correspondingly, the induction of ferritinophagy and disruption of iron homeostasis may be an effective way to improve the therapeutic effect of hypoxic tumor cells.
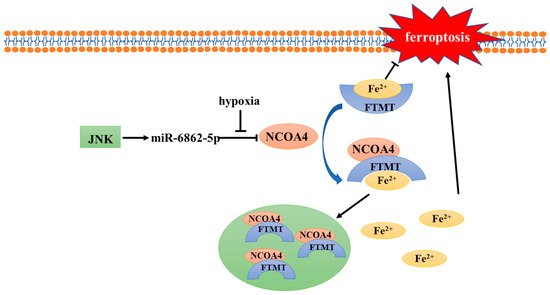
Figure 1. Mechanism of NCOA4 regulation under hypoxia.
The transcription of NCOA4 is related to miR-6862-5p. Under normoxic conditions, NCOA4 can bind with FTMT and Fe2+, and then send the complex to the autolysosome for degradation. However, the transcription of NCOA4 is inhibited when hypoxia occurs, thus blocking ferritinophagy and inhibiting ferroptosis. JNK, c-jun N-terminal kinase; NCOA4, nuclear receptor coactivator 4; FTMT, mitochondrial ferritin.
3. Bidirectional Regulation of Hypoxia-Inducible Factors on Ferroptosis
Hypoxia-inducible factors (HIFs) are ubiquitous in human and mammalian cells and can be stably expressed under hypoxic conditions. HIFs are heterodimeric transcription factors, composed of α and β subunits. The activity of HIFs is mainly dependent on α subunits, while β subunits are responsible for maintaining its stability [
34]. The reason why α and β subunits function differently is that α subunits have an oxygen-dependent degradation domain (ODDD) in their structures [
35]. In addition to ODDD, the α subunits have two transactivation domains: NH2-terminal (N-TAD) and COOH-terminal (C-TAD). They are responsible for the transcriptional activity of HIF-1/2α [
36]. There are three subtypes of HIF-α: HIF-1α, HIF-2α, and HIF-3α [
37,
38]. HIF-1α and HIF-2α are particularly important for hypoxia response and can form complexes with HIF-1β [
39]. The role of HIF-3α is unclear, but it has been suggested that HIF-3α may be involved in the transcriptional inhibition of HIF-1α [
40].
The regulatory pathways of HIF-1/2α can be divided into oxygen-dependent and oxygen-independent pathways. Under normoxic conditions, proline residues (P402 and P564) within the ODDD of HIF-1α subunits and (P405 and P531) of HIF-2α subunits are hydroxylated by prolyl hydroxylases domain enzymes (PHD1-4) [
41,
42]. Hydroxylated HIF-1/2α can be recognized and ubiquitinated by the von Hippel–Lindau protein (pVHL), which mediates the assembly of the VHL/elongin C/elongin B/cullin-2 E3 ubiquitin ligase complex and is subsequently degraded by proteasomes [
43]. In addition to prolyl hydroxylase, factor inhibiting HIF (FIH) is another cellular dioxygenase which could hydroxylate the 803 and 847 residues of asparagine within the C-TADs of HIF-1α and HIF-2α, respectively, and inhibit the transcription of HIF-1/2α [
44]. However, PHDs and FIH are both oxygen dependent. Under hypoxic conditions, their activity is inhibited, allowing HIF-1/2α to escape ubiquitination and be transported to the nucleus after binding with HIF-1β [
45,
46]. In addition, ROS can also regulate the activity of PHDs and FIH. Studies have shown that NADPH oxidase 1 (NOX1) and NADPH oxidase 4 (NOX4) maintain HIF-2α expression in renal carcinoma through ROS generation, contributing to renal carcinogenesis [
47]. Moreover, in recent years, several studies have shown that HIF can be regulated without oxygen; for example, heat shock protein 90 (Hsp90) can bind to HIF-1/2α subunits to inhibit their degradation [
48], PI3K/AKT and MAPK/ERK pathways participate in the regulation of HIF-1/2α expression [
49,
50], and post-transcriptional acetylation and deacetylation regulate HIF-1/2α transcription and stability [
51,
52].
HIF-1/2α play a crucial role in the response of tumors to low oxygen [
53]. Furthermore, the expression of HIF-1/2α is often associated with poor prognosis and chemoradiotherapy resistance [
54]. Therefore, inhibiting HIF-1/2α expression and their downstream pathways activation is considered to be a reliable way to enhance radiosensitivity. Recently, HIF-1/2α subunits were found to play an important role in the regulation of ferroptosis (
Figure 2), which further proved that ferroptosis inhibition is an important factor leading to unfavorable prognosis of hypoxic tumors.
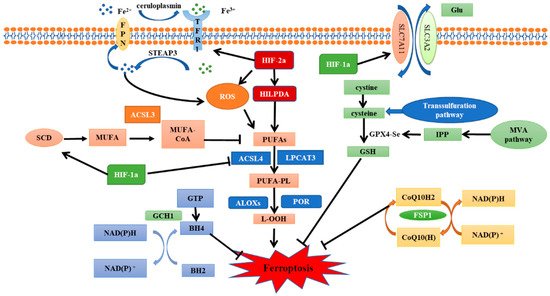
Figure 2. The regulatory pathways of ferroptosis and the role of HIF.
Ferroptosis is regulated by iron metabolism, lipid metabolism and antioxidant system. SLC7A11-GPX4-GSH pathway, FSP1-CoQ10-NAD (P)H pathway and GCH1-BH4-DHFR pathway are several classic ferroptosis inhibition pathways. HIF-1α has a significant inhibitory effect on ferroptosis. It can promote the expression of SCD1 to increase the synthesis of MUFA, inhibit the expression of ACSL4 to avoid lipid peroxidation, and reduce the degradation of SLC7A11 to enhance the antioxidant capacity of cells. In contrast, HIF-2α promotes ferroptosis. Activation of the HIF-2α-HILPDA pathway can promote the synthesis of PUFAs to induce lipid peroxidation. HIF-2α can also regulate iron metabolism gene to increase intracellular free iron content and oxidize cysteine to increase ROS production. SLC7A11, Cystine/glutamate antiporter solute carrier family 7 member 11; GPX4, glutathione peroxidase 4; GSH, glutathione; FSP1, ferroptosis suppressor protein 1; GGH1, GTP Cyclohydrolase 1; BH4, tetrahydrobiopterin; DHFR, dihydrofolate reductase; HIF, hypoxia-inducible factor; SCD1, stearoyl-CoA desaturase 1; MUFA, monounsaturated fatty acids; ACSL4, acyl-CoA synthetase long-chain family member 4; HILPDA, hypoxia inducible lipid droplet-associated proteins; and PUFAs, polyunsaturated fatty acids.
3.1. HIF-1α—A Negative Regulator of Ferroptosis
HIF-1α plays an important role in the metabolic regulation of hypoxic cells. Activation of HIF-1α can enhance the activities of glycolysis, serine synthesis, and pentose phosphate pathways [
55], thereby allowing cells to adapt to the hypoxic environment. The massive production of antioxidants induced by HIF-1α is also considered as one of the mechanisms of radiation resistance in hypoxic cells. In recent years, it has been found that HIF-1α expression is associated with ferroptosis.
To begin with, HIF-1α can inhibit ferroptosis by regulating SLC7A11. SLC7A11 expression is positively associated with HIF-1α in human hepatocellular carcinoma (HCC) tissues [
56]. It has been shown that HIF-1α can inhibit methyltransferase-like 14 (METTL14) expression, thus inhibiting the degradation of SLC7A11 mRNA and reducing the sensitivity of HCC cells to ferroptosis [
57]. Moreover, the HIF-1α/SLC7A11 pathway has also been reported in the nervous system and oral squamous cell carcinoma (OSCC) [
58,
59,
60]. Unfortunately, one study found that HIF-1α does not regulate SLC7A11 in breast cancer cells [
61]. Therefore, the application scope and specific mechanism of this pathway need to be further studied. HIF-1α can also inhibit ferroptosis by regulating lipid metabolism. Yang et al. demonstrated in a variety of human tumor cell lines that aryl hydrocarbon receptor nuclear translocator-like protein 1 (ARNTL, also call BMAL1) inhibits ferroptosis by inhibiting EGLN2 (also call PHD2) activation and activating HIF-1α. Additionally, HIF-1α-induced ferroptosis inhibition may be related to its role in promoting lipid storage [
62]. Conversely, EGLN1 (also call PHD1) inhibits ferroptosis by promoting lymphoid-specific helicase (LSH) expression in lung cancer cell lines [
63]. This result further proves that the regulation of HIF-1α on ferroptosis is complex and variable. Furthermore, ACSL4 is a key enzyme in the formation of polyunsaturated fatty acids; HIF-1α inhibits the synthesis of ACSL4 to inhibit ferroptosis [
64]. In nasopharyngeal carcinoma (NPC), HIF-1α upregulates the expression of stearoyl-CoA desaturase 1 (SCD1), which mediates the production of monounsaturated fatty acids and inhibits ferroptosis [
65]. Finally, a study of cervical cancer (CC) demonstrated that HIF-1α activation can suppress ferroptosis by destroying iron homeostasis imbalance [
66].
These findings confirm that HIF-1α plays an important role in the regulation of ferroptosis. Under hypoxic conditions, HIF-1α can produce antioxidants to resist oxidative stress caused by radiation-induced ROS. It has been confirmed that IR can also cause significant upregulation of HIF-1α, thus further aggravating radiation resistance of hypoxic cells [
67,
68]. Therefore, HIF-1α is an effective target for radiation sensitization of hypoxic cells [
69,
70]. Ferroptosis accounts for a large proportion of IR-induced cell death, even more than apoptosis and necrosis [
19]. HIF-1α-mediated ferroptosis inhibition is closely associated with poor prognosis and treatment tolerance of hypoxic tumors [
60]. Consequently, it may be practical to reduce HIF-1α-induced radiation resistance by regulating the occurrence of ferroptosis.
3.2. HIF-2α—A Positive Regulator of Ferroptosis
As two important members of the HIF family, both HIF-1α and HIF-2α share 48% structural homology [
71]. Thus, they have certain functional similarities in regulating physiologic and pathologic responses in hypoxic environments and in affecting the development of hypoxia-related diseases. However, increasing evidence has revealed that when expressed in the same cell type, HIF-1α and HIF-2α activation can produce highly different or even opposite results [
72,
73]. Previous studies on ferroptosis have shown that HIF-2α plays a positive role in ferroptosis in various tumor models [
74,
75].
Zou et al. showed that HIF-2α activation stimulated hypoxia-induced expression of lipid droplet-associated proteins (HILPDA) and selectively enriched polyunsaturated lipids to improve the sensitivity of clear-cell carcinoma cells to ferroptosis. Notably, HIF-1α also plays a role in increasing ferroptosis sensitivity in ovarian clear cell carcinoma cells [
74]. The clear-cell carcinomas (CCCs) are always associated with highly active lipid and glycogen synthesis and deposition, which promotes tumor progression and treatment resistance [
76]. HIF-mediated ferroptosis susceptibility may be related to the special metabolic state and high GPX4 dependence of clear-cell carcinoma cells [
77]. Therefore, the relationship between HIF and ferroptosis in other tumors with high metabolic activities and GPX4 dependence is worth exploring. In addition, under hypoxic conditions, HIF-2α is a major regulator of erythropoiesis and cellular iron metabolism, which can interfere with bone morphogenetic protein (BMP) signaling, inhibit the expression of hepcidin, and regulate iron uptake and mobilization in the intestinal diet [
78,
79]. Studies have shown that HIF-2α activation can upregulate the expression of lipid and iron regulation genes as well as increase the intracellular iron level, thereby leading to the susceptibility of colorectal cancer cells to ferroptosis. Furthermore, HIF-2α activation enhances colon cancer cell death by promoting irreversible cysteine oxidation in an iron-dependent manner to increase ROS production. In contrast, HIF-1α has no significant regulatory effect on colorectal cancers [
75]. A recent study showed that HIF-2α also mediates ferroptosis in chondrocytes [
80], implying a more general role of HIF-2α in ferroptosis in other contexts. However, as a hypoxia-triggered factor, HIF-2α has a similar effect as HIF-1α on radiation resistance, so the role of HIF-2α-mediated ferroptosis in radiotherapy is open to debate.
Radiation and chemotherapy resistance caused by hypoxia has always been a major problem in tumor therapy; however, targeting hypoxic cells remains a challenge, as frequent use of HIF inhibitors can rapidly develop drug resistance in tumor cells. Recent studies have shown that regulating the activity of HIF to promote ferroptosis sensitivity may be a good way to solve the poor prognosis of hypoxic tumors [
60]. As mentioned above, HIF-1α inhibits ferroptosis by targeting SLC7A11, lipid metabolism, and iron homeostasis. HIF-2α induces ferroptosis, perhaps because it is a major regulator of iron metabolism in hypoxic conditions. However, both HIF-1α and HIF-2α show promoting effects on ferroptosis in CCCs, suggesting the regulation of ferroptosis by HIF is complex and can be affected by many factors such as tumor types, metabolic levels and external environment. Therefore, further studies on HIF and ferroptosis should be carried out to provide more effective methods for the radiosensitization of solid tumors.