Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Biochemistry & Molecular Biology
The rising tide of antibacterial drug resistance has given rise to the virtual elimination of numerous erstwhile antibiotics, intensifying the urgent demand for novel agents. A number of drugs have been found to possess potent antimicrobial action during the past several years and have the potential to supplement or even replace the antibiotics.
- thioxanthenes
- antipsychotic drugs
- non-antibiotics
1. Introduction
The first goal of antipsychotic medication is to minimize or eliminate the symptoms within a short period of time. Originally, antipsychotic drugs were designed and tested empirically on psychiatric patients to determine their effectiveness. The first antipsychotic drug that was primarily used as an anesthetic agent in surgery was chlorpromazine [1]. In the beginning, chlorpromazine was administered to psychiatric patients to determine its calming effects. However, it was soon realized that the drug also reduced psychosis. Antipsychotic drugs have been classified as either low or high potency based on their ability to bind to dopamine receptors and not on their effectiveness on patients. Antipsychotic drugs tend to block the action of D2 neuroreceptors in the dopamine pathway in the brain, resulting in reduction of the release of dopamine in the relevant synapses [2]. Thus, an antipsychotic drug should be able to also block the D2 receptors in the mesolimbic pathway of the brain [3,4].
Currently there are two main types of antipsychotics in use, typical and atypical. The main difference between typical and atypical antipsychotic drugs is the ability of the latter to address the negative symptoms of schizophrenia. These atypical neuroleptics, known as newer drugs, date back to the introduction of clozaril [5]. These atypical drugs usually do not cause unpleasant side effects. Atypical drugs may improve cognitive symptoms and can be effective in patients resistant to typical antipsychotic drugs. Such drugs can be active on other receptors, in addition to the dopamine receptor, and many have no extra-pyramidal side effects. Atypical antipsychotics possess an almost identical effect on D2 receptors but are usually more selective, targeting the intended pathway to a larger degree than other drugs.
Typical antipsychotics are sometimes referred to as major tranquilizers, since many of them, in large doses, can sedate and tranquilize [6].
Typical antipsychotics can be classified into three major groups (phenothiazines, butyrophenones and thioxanthenes). Of these, phenothiazines are the most widely used. Table 1 lists the chemical classification of the neuroleptics, illustrated by a selection of the most commonly prescribed drugs from each class along with their structures.
Table 1. Chemical classification of antipsychotic drugs.
| Class of Antipsychotics | Drugs and Their Chemical Structures |
|---|---|
1. Phenothiazines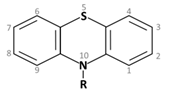 Phenothiazine basic ring structure |
|
| a. Amino alkyl compounds: (Low/medium potency agents that can antagonize α1-adenoreceptors, histamine H1 receptors and muscarinic cholinergic receptors) |
Chlorpromazine: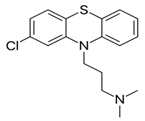 |
| b. Piperidine compounds: (Low/medium potency agents and also muscarinic antagonist) |
Thioridazine: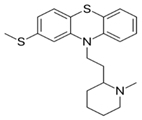 |
| c. Piperazine compounds: (Medium/high potency agents) |
Trifluoperazine: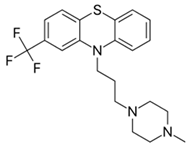 |
2. Butyrophenones Butyrophenone basic ring structure (High potency agents) |
Haloperidol: |
Droperidol: |
|
3. Thioxanthenes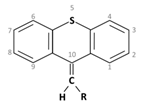 Thioxanthene basic ring structure (Medium potency agents) |
Chlorprothixene: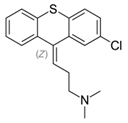 |
Flupenthixol: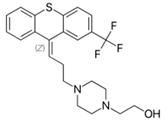 |
|
|
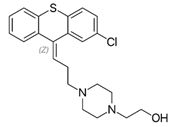
Clopenthixol:
|
(Note: The terms “low/medium/high potency” indicates their potency in binding to the dopamine D2 receptor).
Thioxanthenes, the third group of antipsychotics, are represented in two geometric stereoisomers: Z- and E-compounds, of which the former have been shown to be more neuroleptically active [7,8]. Due to structural similarity, the antipsychotic activities of flupenthixol and clopenthixol are quite similar to the ‘piperazine group’, one of three groups in the phenothiazine class. These compounds are able to benefit psychotic patients by blocking postsynaptic dopamine receptors in the brain. Thioxanthenes also produce an alpha-adrenergic blocking effect and depress the release of a large number of hypothalamic and hypophyseal hormones [8].
Thioxanthenes were synthesized and developed with the hope of eliminating the toxic effects of chlorpromazine. The first thioxanthene that came to the market in Scandinavia in 1959 was chlorprothixene. A more potent compound, clopenthixol, was introduced in Denmark and other European countries in 1961, followed by introduction of thiothixene and flupenthixol [9].
2. Therapeutic Usage of Thioxanthenes
Much like the other neuroleptics, thioxanthenes are prescribed for patients suffering from schizophrenia. In addition to this, some of the drugs in this group possess specific characteristics that justify their application in clinical medicine.
Table 2 includes a comparative summary of these three classes of neuroleptics, listing some of the common risks of antipsychotic medications [10,11,12,13,14,15,16,17,18,19].
Table 2. Comparative summary of antipsychotic side effects.
| Adverse Effects |
Drugs | ||||||
|---|---|---|---|---|---|---|---|
| (1) Phenothiazines | (2) Butyro- Phenones |
(3) Thioxanthenes | |||||
| Chlorpromazine | Thioridazine | Trifluoperazine | Haloperidol | Chlorprothixene | Flupenthixol | Clopenthixol | |
| Extra Pyramidal Side Effects: The muscle related side effects observed with antipsychotic medications are termed as ‘Extra -Pyramidal Side Effects’ or EPS [10] |
Low | Low | High | Very high | In a comparative study it was observed that Parkinsonian symptoms were more often found with chlorpromazine than chlorprothixene [11] |
Develops in high dosages, can be controlled by anti-parkinsonian drugs [12,13] |
High |
| Anti-cholinergic Effects: This includes symptoms like urinary difficulties, constipation, dry mouth, blurred visions and may lead to cognitive impairments. |
High | High | Low | Very low | Moderate | Low | Both clopenthixol and flupenthixol were found to have lower effect in comparison to chlorprothixene [14] |
| Sedation: This is common with antipsychotic medications and is dose dependent. |
High | High | Low | Produces much lesser sleepiness and calming effect than chlorpromazine [15] |
High | Low | Low |
| Hypotension: Antipsychotics commonly cause orthostatic hypotension, depending on the degree of α1 adrenoreceptor antagonism. |
High | High | Low | Very low | High | Moderate | Treatment with clopenthixol is often associated with orthostatic hypotension [19] |
| Other Effects: | Photosensitivity: Chlorpromazine is known to induce photosensitivity and skin pigmentation [16]. An intensive study with phenothiazines and thioxanthenes on schizophrenic patients [17] reported that patients receiving chlorpromazine showed statistically significant changes in the lens and cornea while patients treated with thioxanthenes did not. |
Hyperprolactinemia: Thioxanthenes cause high prolactin levels due to the blockade of prolactin inhibitory factors (PIF), that inhibits release of prolactin from the pituitary gland [18]. |
|||||
The first thioxanthene, chlorprothixene, was found to have an excellent effect in schizophrenic patients [20]. Chlorprothixene had been used in the treatment of neuroses, not only due to its sedative and calming effects but also due to its low level of toxicity and side effects. Treatment with rather low doses results in favorable results in neuroses with anxiety, tension, insomnia, psychosomatic disorders, and depression. Chlorprothixene had also been found useful for treating alcoholics and alcohol psychoses [21].
Flupenthixol is the highly potent thioxanthene analogue of the phenothiazine fluphenazine [22]. Flupenthixol possesses a distinct anxiolytic property. At low and, sometimes, rather higher doses, this drug is effective against hallucinations and delusions. Flupenthixol manifests stimulating or activating properties in low doses; sometimes even apathetic patients show greater alertness. Schizophrenic patients treated with chlorpromazine, levomepromazine, or other thioxanthenes are sometimes given flupenthixol in low doses as aftercare. It can control psychotic symptoms without affecting the alertness or working ability of the patients [9,23]. The action of flupenthixol is much similar to that of trifluoperazine, but the former induces much less extra-pyramidal effects [24]. Flupenthixol is often prescribed for mood stabilization when psychiatric patients suffer from depressive neurosis. During the early 1970′s, intensive clinical studies repeatedly proved the excellent efficacy of flupenthixol over other neuroleptics in depressive patients [25,26]. Administration of this drug in low dosages does not usually produce side effects, however, sleep disturbances may occur in some patients who are treated after 5 pm [9].
Clopenthixol has a narrower field of application compared to chlorprothixene, although often it produces quick action on patients suffering from delusions, aggressiveness, destructiveness, impulsiveness, and even hallucination, and has also been proven to be definitely better than chlorpromazine for treating paranoid schizophrenics [27]. It produces highly satisfactory results in paranoids and catatonics [28]. Treatment with clopenthixol may start with a low dose followed by a gradual increase. However, therapy has to be continued on a regular basis with one tablet in the evening.
3. Pharmacological Properties of Thioxanthenes
Much like the phenothiazines, thioxanthenes exhibit varied pharmacological actions, peripheral as well as central. However, therapeutic uses of these compounds depend on their psychopharmacological activity. The neuroleptic potency of a synthesized thioxanthene depends on the structure of the side chain in position 9. The compounds with β-hydroxyethylpiperazinopropyl or β-hydroxyethylpiperidinopropyl side chains are more potent neuroleptically than those with a dimethylaminopropyl side chain [29]. The antagonistic effect against methylphenidate-induced stereotypes in mice was employed to determine the exact duration of neuroleptic action of a compound. It was found that the peak effect was between 2 and 6 h, and by 24 h, effects of all the compounds were gone [9,30].
Neuroleptics are known to block the dopamine-induced formation of cyclic adenosine monophosphate (cAMP). In an elaborate study, Iversen et al. (1974) [31] observed that Z-flupenthixol was the most potent neuroleptic among all the test phenothiazines, thioxanthenes, and tyrophenones. Interestingly, they noted that E-flupenthixol was completely inactive.
It is known that neuroleptics have to be administered to psychiatric patients on a long term basis. In 1974, Moller et al. [32] observed that the antagonistic effect of neuroleptics undergoes tolerance development in animal models after prolonged therapy. They reported that when rats were pre-treated with flupenthixol for 12 days, followed by 3 days withdrawal, the antagonistic potency against apomorphine stereotypes was decreased. This reduction in potency subsequently gradually disappeared.
Neuroleptics are known for their α-adrenolytic function. Between phenothiazines and thioxanthenes, the adrenolytic activity was found to be more prominent in the Z-isomers of chlorprothixene, flupenthixol, and clopenthixol, while chlorpromazine and fluphenazine (which has no E/Z center) revealed much less activity [33].
Nasrallah & Tandon (2013) [9] observed that there was a moderate reduction in adrenaline pressor response after administration of either chlorprothixene or flupenthixol to anaesthetized cats. Furthermore, in vagotomized cats, the carotid occlusion reflex was reduced. After administration of chlorprothixene in these animals, respiration remained unaffected, although initially there was a transient rise in respiratory minute volume, due to increased tidal volume. Intravenous infusion of chlorprothixene or flupenthixol in conscious dogs resulted in the fall of blood pressure, without any change in pulse pressure. Treatment of dogs exhibiting tachycardia with flupenthixol resulted in a normalization of heart rate for 15 min [9,14].
This entry is adapted from the peer-reviewed paper 10.3390/molecules27010196
This entry is offline, you can click here to edit this entry!