Craniofacial surgery is proposed and performed for a variety of reasons, ranging from congenital or acquired malformations to emotional disorders and parafunctions of the masticatory, respiratory, auditory, and visual systems. Surgery of the mandible and its orthostatic repositioning is the most common of these corrections of craniofacial anomalies. Throughout the history of these procedures, various techniques have been proposed and perfected, but always with a high rate of minor and major complications. The recurrence rate of mandibular malposition is high, as is the temporary loss of facial sensitivity and motor skills. These outcomes are often related to the choice of surgical technique rather than the skill of the surgeon, which is considered to be one of the most important factors in the final outcome. Surgical techniques involving direct manipulation of the vascular-nervous bundles, such as bilateral sagittal split osteotomy, clearly present the possibility of major or minor complications.
- orthognathic surgery
- craniofacial surgery
1. Introduction



2. Innovation in Biomechanical Orthognathic Surgery
This entry is adapted from the peer-reviewed paper 10.3390/osteology4010002
References
- Hullihen, S.P. Case of elongation of the underjaw and distortion of the face and neck, caused by a burn, successfully treated. Am. J. Dent. Sci. 1849, 9, 157–161.
- Aziz, S.R.; Simon, P. Hullihen and the origin of orthognathic surgery. J. Oral Maxillofac. Surg. 2004, 62, 1303–1307.
- Blair, V.P. Surgery and Diseases of the Mouth and Jaws; The C.V. Mosby Co.: St. Louis, MO, USA, 1914.
- Steinhäuser, E.W. Historical development of orthognathic surgery. J. Cranio-Maxillofac. Surg. 1996, 24, 195–204.
- Kazanjian, V.H. The treatment of mandibular prognathism with special reference to edentulous patients. J. Oral Surg. Oral Med. Oral Pathol. 1951, 4, 680–688.
- Schuchardt, K. Die Chirurgie als Helferin der Kieferorthopädie . Fortschr. Kieferorthop. 1954, 15, 1–25.
- Obwegeser, H.L. Orthognathic surgery and a tale of how three procedures came to be: A letter to the next generations of surgeons. Clin. Plast. Surg. 2007, 34, 331–355.
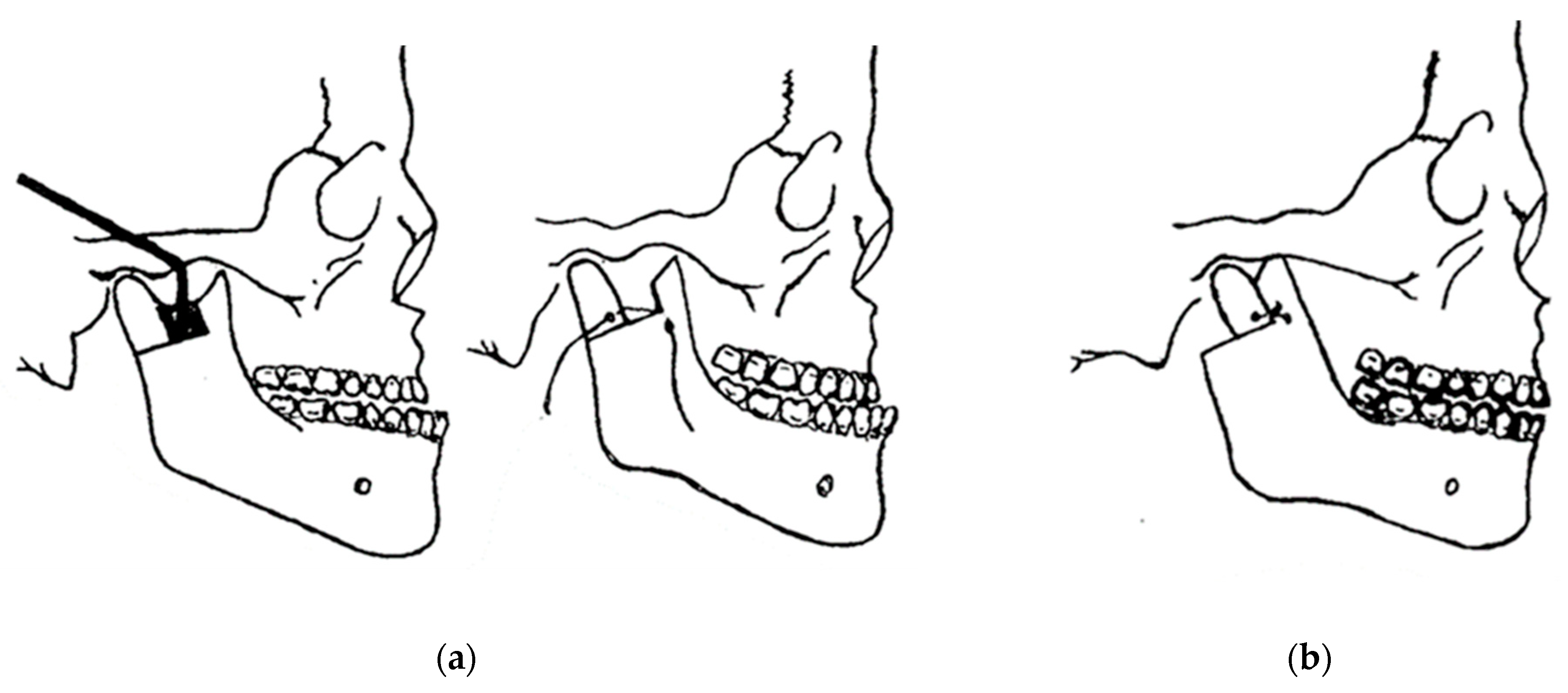
- Caldwell, J.B.; Letterman, G.S. Vertical osteotomy in the mandibular rami for correction of prognathism. J. Oral. Surg. 1954, 12, 185–202.
- Trauner, R.; Obwegeser, H. Zur Operationstechnik bei der Progenia und anderen Unterkieferanomalien. Dtsch. Zahn. Mund. Kieferhlkd. 1955, 23, 11–25.
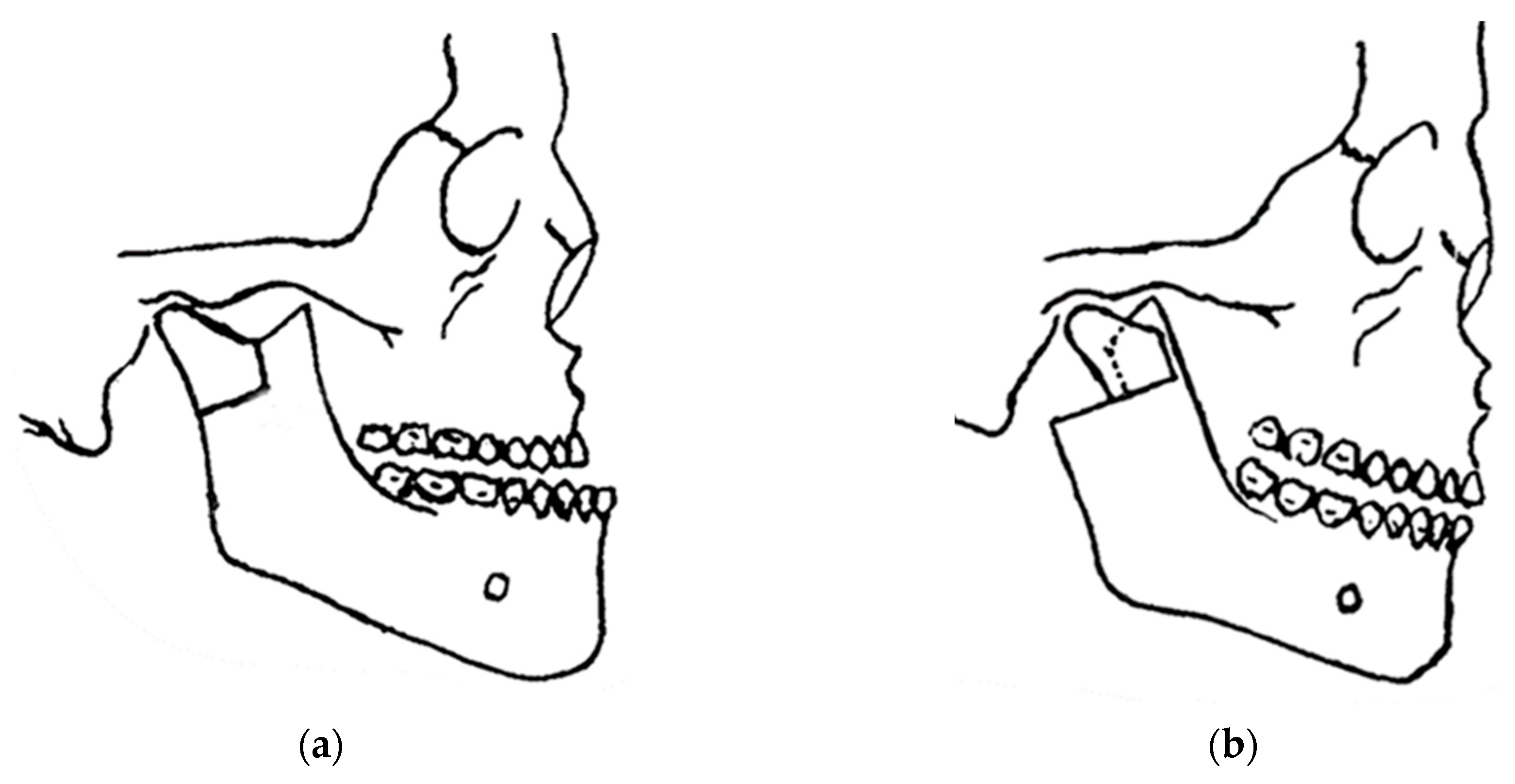
- Dal Pont, G. L’osteotomia retromolare per la correzione della progenia. Minerva. Chir. 1959, 14, 1138–1141.
- Dal Pont, G. Retromolar osteotomy for the correction of prognathism. J. Oral Surg. Anesth. Hosp. Dent. Serv. 1961, 19, 42–47.
- Hunsuck, E.E. A modified intraoral sagittal splitting technic for correction of mandibular prognathism. J. Oral Surg. 1968, 26, 250–253.
- Epker, B.N. Modifications in the sagittal osteotomy of the mandible. J. Oral Surg. 1977, 35, 157–159.
- Schmoker, R.; Spiessl, B.; Tschopp, H.M.; Prein, J.; Jaques, W.A. Die funktionsstablie Osteosynthese am Unterkiefer mittels exzentrisch-dynamischer Kompressionsplatte (EDCP). Ergebnisse einer Nachuntersuchung der ersten 25 Fälle . SSO Schweiz. Monatsschr. Zahnheilkd. 1976, 86, 167–185.
- Ow, A.; Cheung, L.K. Skeletal stability and complications of bilateral sagittal split osteotomies and mandibular distraction osteogenesis: An evidence-based review. J. Oral Maxillofac. Surg. 2009, 67, 2344–2353.
- Saman, M.; Abramowitz, J.M.; Buchbinder, D. Mandibular osteotomies and distraction osteogenesis: Evolution and current advances. JAMA Facial Plast. Surg. 2013, 15, 167–173.
- Hofer, O. Operation del Prognathie und Microgenie. Dtsch. Zahn. Mund. Kleferhlkd. 1942, 9, 121–132.
- Babcock, K.W. Surgical treatment of certain deformities of jaw associated with malocclusion of teeth. J Am Med Assoc. 1909, 53, 833–839.
- Castro, O. Mandibular prognathism. Mandibuloplasty by Smith’s technique. Rev. Lat. Am. Cir. Plast. 1964, 8, 24.
- Castro, O. Surgical correction of prognathism: Angled osteoplasty of the mandibular rami. Br. J. Plast. Surg. 1967, 20, 57–60.
- Castro, O.; Mortari, S.; Colares, H.J. Significant details regarding treatment of prognathism using angled osteotomy of the mandibular rami. Aesth. Plast. Surg. 1980, 4, 349–355.
- Smith, A.E.; Robinson, M. The evaluation of physiologic result from submandibular-notch osteotomy, condylotomy operation for prognathism. Plast. Reconstr. Surg. 1955, 15, 196.
- Rehrmann, A. Horizontal osteotomy of the mandibular rami with wire suture for the correction of prognathism with preservation of the original position of the condyles. Dtsch. Zahn. Mund. Kieferheilkd. Zentralbl. Gesamte. 1967, 49, 72–76.
- Rehrmann, A.; Schettler, D. Treatment of bilateral fractures of the temporomandibular joint in infants and young children with reposition and fixation according to Rehrmann’s method. Dtsch. Zahnarztl. Z. 1966, 21, 777–782.
- Rehrmann, A. Reposition and retention of the mandible in fractures of the articular process and condyle by extraoral elastic traction in the chin region. Dtsch. Zahn. Mund. Kieferheilkd. Zentralbl. Gesamte. 1971, 57, 379–392.
- Obwegeser, H. Die einzeitige Vorbewegung des Oberkiefers und R flick bewegung des Unterkiefers zur Korrektur der extremen ‘Progenie’. Schweiz Mschr. Zahnheilk. 1970, 80, 305.
- Tessier, P.; Guiot, G.; Rougerie, J. Cranio-naso-orbito-facial osteotomies (hypertelorism). Ann. Chir. Plast. 1967, 12, 103–118.
- Luhr, H.G. The compression osteosynthesis of mandibular fracture in dogs. A histological contribution to “primary bone healing”. Eur. Sur. Res. 1967, 1, 3.
- Luhr, H.G. Zur stabilen osteosyntheses bei unterkiefer-frakturen. Dtsch. Zahnarztl. Z 1968, 23, 754.
- Luhr, H.G. Stabile Fixation von Oberkiefer-Mittelgesichtsfrakturen durch Mini-Kompressionsplatten. Dtsch. Zahnarztl. Z 1979, 34, 851.
- Luhr, H.G. Indications for use of a microsystem for internal fixation in craniofacial surgery. J. Craniofac. Surg. 1990, 1, 35–52.
- Dreiseidler, T.; Bergmann, J.; Zirk, M.; Rothamel, D.; Zöller, J.E.; Kreppel, M. Three-dimensional fracture pattern analysis of the Obwegeser and Dal Pont bilateral sagittal split osteotomy. Int. J. Oral Maxillofac. Surg. 2016, 45, 1452–1458.
- Mensink, G.; Verweij, J.P.; Frank, M.D.; Bergsma, J.E.; van Merkesteyn, J.P.R. Bad split during bilateral sagittal split osteotomy of the mandible with separators: A retrospective study of 427 patients. Br. J. Oral Maxillofac. Surg. 2013, 51, 525–529.
- Salzano, G.; Audino, G.; Friscia, M.; Vaira, L.A.; Biglio, A.; Maglitto, F.; Committeri, U.; Piombino, P.; Bonavolontà, P.; Petrocelli, M.; et al. Bad splits in bilateral sagittal split osteotomy: A retrospective comparative analysis of the use of different tools. J. Cranio-Maxillofac. Surg. 2022, 50, 543–549.
- Li, F.; Li, S.; Wu, S.; Le, Y.; Tan, J.; Wan, Q. Effect of the lateral bone cut end on pattern of lingual split during bilateral sagittal split osteotomy in patients with skeletal class III malocclusion. Br. J. Oral Maxillofac. Surg. 2023, 61, 309–314.
- Lasco, G.E. 20 anos de cirurgia maxilo-facial (20 years of maxillofacial surgery). In Atualizaçäo Clínica em Odontologia; Marco Antonio, B., Christa, F., Eds.; Artes Médicas: Säo Paulo, Brazil, 1984; pp. 219–230.
- Lasco, G.E.; Mello, J.B. Contribuiçäo ao tratamento cirúrgico das luxaçöes recidivantes da ATM (Contribution to surgical treatment of temporomandibular joint recidivant dislocation). In Atualizaçäo Clínica em Odontologia; Marco Antonio, B., Christa, F., Eds.; Artes Médicas: Säo Paulo, Brazil, 1984; pp. 231–236.
- Lasco, G.E.; Mello, J.B. Disfunçöes dolorosas da ATM (TMJ pain dysfunctions). In Atualizaçäo Clínica em Odontologia; Marco Antonio, B., Christa, F., Eds.; Artes Médicas: Säo Paulo, Brazil, 1984; pp. 237–242.
- Lasco, G.E. Contribuição ao estudo da patologia e terapêutica da Articulação Temporomandibular (Contribution to the study of the pathology and therapy of the Temporomandibular Joint). Rev. APCD 1967, 2, 264.