Turner syndrome (TS), a genetic disorder due to incomplete dosage compensation of X-linked genes, affects multiple organ systems, leading to hypogonadotropic hypogonadism, short stature, cardiovascular and vascular abnormalities, liver disease, renal abnormalities, brain abnormalities, and skeletal problems. Patients with TS experience premature ovarian failure with a rapid decline in ovarian function caused by germ cell depletion, and pregnancies carry a high risk of adverse maternal and fetal outcomes. Aortic abnormalities, heart defects, obesity, hypertension, and liver abnormalities, such as steatosis, steatohepatitis, biliary involvement, liver cirrhosis, and nodular regenerative hyperplasia, are commonly observed in patients with TS.
1. Introduction
Turner syndrome (TS) is one of the most common disorders caused by chromosomal abnormalities, affecting approximately 1 in 2500 live female births. It is the only viable monosomy syndrome caused by partial or complete loss of one of the two sex chromosomes [
1]. TS was first reported in 1938 by Henry H. Turner as a syndrome of infantilism, congenital webbed neck, and cubitus valgus, and Ford et al. found that the disease was caused by sex chromosomal abnormality in 1959 [
2,
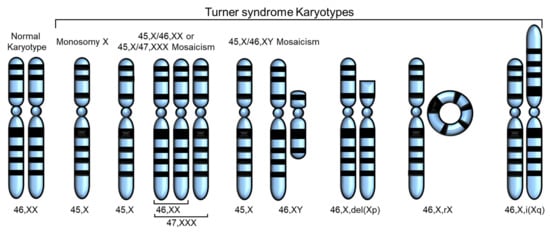
3]. The most common karyotype in TS is 45,X, accounting for 40–50% of all cases of TS, whereas 45,X/46,XX or 45,X/47,XXX mosaicism account for 20–30%. The remaining cases include Y chromosome variants and X chromosome structural abnormalities, such as isochromosome Xq, deletion of Xp or Xq (which can occur as mosaicism), and ring X (which is always mosaic) [
4] (
Figure 1). Thus, in TS, only one X chromosome is normal and the others are absent or abnormal. The diagnosis of TS has traditionally relied on the clinical phenotype in addition to standard chromosomal analysis [
5]. Total or partial loss of one of the two sex chromosomes affects biological pathways and networks [
5], and, in some cases,
SHOX gene defects have been linked to certain phenotypes of TS [
6,
7] (
Table 1).
Figure 1. Various karyotypes of Turner syndrome (TS) modified from Huang et al. [
8]. Partial or complete loss of the second sex chromosome results in TS. The most common karyotype in TS is monosomy X (45,X), and the others are 45,X/46,XX or 45,X/47,XXX mosaicism, 45,X/45,XY mosaicism, deletion of Xp or Xq, ring X (46,X,rX), and isochromosome Xq.
Table 1. Genes associated with Turner Syndrome (TS).
Individuals with TS are at an increased risk of endocrine diagnoses, including diabetes, thyroid and parathyroid disorders, celiac disease, and osteoporosis [
23,
24], as well as cardiovascular diseases, including arrhythmia, ischemic heart disease, hypertension, hyperlipidemia, and stroke. This is supported by the increased use of prescription drugs by patients with TS [
25]. The 45,X karyotype is associated with the highest rates of morbidity and mortality, whereas the mosaic karyotype is associated with a low prevalence for cardiovascular, metabolic, renal, and reproductive phenotypes [
26,
27,
28,
29,
30,
31,
32,
33]. Despite ongoing research, no feasible treatment has been proposed owing to the severe effects of losing an entire chromosome and the numerous genes that are simultaneously affected [
34].
2. Fertility Problems
Infertility is one of the most common symptoms of TS, despite low rates of spontaneous pregnancies [
31,
35,
36,
37]. TS is accompanied by hypogonadotropic hypogonadism in almost all patients, leading to primary or secondary amenorrhea and infertility owing to premature ovarian failure (POF) (affecting approximately 95% of women with TS) and premature ovarian insufficiency [
28,
38,
39]. Therefore, women with TS do not produce enough eggs or the necessary hormones to support pregnancy. The ovaries in a 45,X fetus appear to develop normally until birth; however, follicular atresia is induced by birth or early childhood [
40]. Moreover, 5–20% of girls with TS retain enough follicles to permit spontaneous menarche, even if early menopause typically follows. Women with TS who have a mosaic karyotype, or experience spontaneous puberty, have follicles in one or both ovaries [
39]. Furthermore, those with low levels of 45,X/46,XX mosaicism are less severely affected and have a high likelihood of experiencing spontaneous menstruation and pregnancy, although karyotype does not always predict phenotype [
41,
42,
43]. Accelerated germ cell death is presumed to be the major mechanism causing germ cell depletion in patients with TS.
Reynaud et al. analyzed 10 aborted fetuses with TS and found that the number of germ cells in the genital ridge was similar to that in the control group up to 12 weeks of gestation, indicating normal migration of primordial germ cells in fetuses with TS [
44]. However, differences were observed from 18 weeks of gestation, where germ cells were rarely detected, and completely absent at 25 weeks of gestation in fetuses with 45,X TS. Moreover, primordial and antral follicles were absent in fetuses with 45,X TS, although they were present in fetuses with TS with mosaicism. These studies suggest that folliculogenesis is severely impaired in ovaries of patients with TS, possibly owing to the loss of germ cells [
44]. Additionally, the eggs from women with TS might be of poor quality, decreasing the chances of successful fertilization and pregnancy [
45].
TS can also cause abnormalities in the structure and function of the uterus, affecting the implantation and growth of fertilized eggs [
46]. Only about a quarter of people with TS have a fully developed uterus in size and shape, while most others have a slightly smaller uterus; about one-third have an immature form of the uterus. Notably, the difference in the size of the uterus between women with TS and those with a normal karyotype is not significant; however, on average, women with TS have a smaller uterine volume than those with a normal karyotype. The size of the uterus in individuals with TS can be influenced by various factors, including the age of the patient, duration of estrogen use, use of hormone replacement therapy (HRT), and type of estrogen medication administered. However, with appropriate and timely treatment, women with TS can achieve normal uterine development [
46].
In addition, an imbalance in sex hormone levels affects the fertility of patients with TS. Women with TS showed 30–50% lower levels of androgens, including testosterone, free androgen index, androstenedione, and dehydroepiandrosterone sulfate, than those with a normal karyotype, but an increase in Follicle stimulating hormone (FSH), Luteinizing hormone (LH), and estrone sulfate levels up to twice the normal range [
47]. High levels of FSH and LH during adolescence are linked to reduced ovarian function [
48]. However, patients with TS showed a normal biphasic age pattern of reproductive hormones, with peak FSH and LH levels occurring at three months of age, followed by a subsequent decrease to minimal levels during mid-childhood and reactivation at puberty [
48,
49].
Pregnancy is rare among patients with TS and shows a high risk of miscarriage, stillbirth, and birth defects [
50]. Only 2–5% of patients with TS become pregnant spontaneously, and approximately 3.8% of patients with TS have one or more live-born children [
28,
35]. Both natural and medically assisted pregnancies in patients with TS have a higher risk of adverse maternal and fetal outcomes than those in healthy women. For instance, 23–50% of women with TS have congenital heart disease, and pregnancy causes a 50% increase in cardiac output, making patients with TS susceptible to aortic dissection or rupture. As a result, the risk of death during pregnancy for patients with TS can reach up to 2% [
51,
52].
3. Heart and Cardiovascular Disease
Congenital and acquired heart defects and cardiovascular conditions are the leading cause of death in patients with TS, affecting about 25–50% of cases, with a higher incidence in those with 45,X karyotypes than in those with other TS variants [
55]. Miyabara et al. conducted an autopsy of a 20-week-old fetus with 45,X karyotype and found that the wall of the aortic arch was much thinner than normal and that the number of smooth muscle cells and elastic fibers in the aorta was significantly reduced [
56]. Anomalies of the coronary arteries are diverse and include many variants other than two arteries originating from aortic sinuses [
57]. Many types of coronary artery anomalies have been reported in TS, especially in patients with bicuspid aortic valve (BAV) [
58,
59,
60]. Although not all patients with TS have arch anomalies, aortic arch anomalies are common in TS owing to the complex embryological development of this vessel [
61,
62,
63]. The most common anomalies include elongation of the arch and aberrant right subclavian artery [
64,
65]. Patients with TS and aortic arch anomalies are also at risk of developing aortic dilation, which could increase the risk of aortic dissection, occurring in 1–2% of patients with TS [
66,
67].
Aortic arch hypoplasia is another congenital aortic anomaly associated with TS and may vary in severity from mild aortic stenosis to severe transverse arch hypoplasia, interrupted aortic arch, or hypoplastic left heart syndrome [
68]. Patients with TS are also prone to increased carotid artery thickness and arterial diameter, possibly owing to estrogen deficiency, which can be attenuated by estrogen hormone therapy [
69,
70,
71]. Abnormalities of the venous system, such as hypoplasia of the portal vein system, are also observed in patients with TS, and vascular atrophy is involved in liver dysfunction [
72].
As abnormal extracellular matrix (ECM) composition induces aortic structural malformation, matrix metalloproteinases (MMPs, a degradation factor of ECM), and tissue inhibitors of matrix metalloproteinases (TIMPs, inhibitor of MMPs) are involved in aortic abnormalities [
88]. Increased expression of MMPs and reduced expression of
TIMP1 and
TIMP3 can lead to the degradation of ECM components of the aortic wall, resulting in thinning of the aortic wall and enlargement of the diameter. These changes are implicated in the pathogenesis of various abnormal aortic morphogeneses, such as BAV and aortic aneurysms [
88,
89]. Therefore, hemizygous expression of
TIMP1 on the Xp locus in patients with TS may increase susceptibility to abnormal aortic morphogenesis. Decreased expression of
TIMP3, a
TIMP1 paralogue on chromosome 22, can augment the risk for aortopathy and BAV [
88]. In addition,
TIMP1 is hypermethylated, which suggests that this gene is epigenetically inactive in patients with TS [
90]. Moreover, reduced expression of
TIMP1 and
TIMP3 was observed in the euploid population with BAV and aortopathy [
89].
4. Liver Abnormalities
Although liver involvement is mostly asymptomatic in patients with TS, a wide range of abnormal phenotypes may be observed in the liver, including steatosis, steatohepatitis, liver cirrhosis, biliary involvement, and nodular regenerative hyperplasia (NRH) [
91,
92,
93,
94,
95,
96]. Singh et al. reported that approximately twice the number of girls with TS showed liver enzyme elevation (alanine aminotransferase and aspartate aminotransferase) compared with normal controls [
97]. These liver enzyme levels have clinical significance as girls with TS with elevated liver enzyme levels are more likely to be diagnosed with liver disease [
97]. For example, hypertransaminasemia is common in patients with TS and is typically associated with hepatic steatosis, which can also be caused by other factors, such as diabetes mellitus and dyslipidemia [
98]. In addition, women with TS with elevated liver enzymes are overweight and exhibit high levels of cholesterol, triglycerides, apolipoproteins A and B, and gamma-glutamyl transferase [
99]. Excessive body weight is a common cause of liver disease in patients with TS [
99,
100]. Patients who are overweight (>25 kg/m
2), as defined by body mass index (BMI) values, frequently experience insulin secretion disorders and diabetes mellitus. However, increased weight and BMI in patients with TS are not necessarily estrogen-related. Moreover, the lack of estrogen or GH (Growth Hormone) treatment is not the primary cause of the increase in liver enzymes.
5. Kidney Abnormalities
Kidney abnormalities are common in patients with TS, with a prevalence of 33–70%, and include kidney and urinary tract anomalies, such as abnormal ureter structure leading to urine regurgitation, horseshoe kidney (kidney fusion), renal aplasia, duplex collecting system, single unilateral kidney, and formation of cilia and cysts in the kidney [
111,
112,
113,
117]. The most frequently reported renal anomaly is the horseshoe kidney, which occurs in 20–45% of patients with TS, whereas it is observed in less than 3% of the general population [
141,
142]. Horseshoe kidney is caused by the fusion of the two kidneys, forming a U-shaped structure. While patients with TS with horseshoe kidney may be asymptomatic during childhood, they may experience recurrent urinary tract infections and kidney stones in the later stages of the condition [
112,
115,
116,
119]. The incidence of renal malformations is significantly higher in patients with TS with a non-mosaic 45,X karyotype than in those with mosaicism, probably owing to lymphatic retention and organ system compression [
116]. Hypertension can also be caused by renal malformations besides aortic stenosis and intrarenal vascular changes in patients with TS [
116]. Other rare cases of malformations include rotation and postural abnormalities, severe and mild hydronephrosis, and unilateral/bilateral overlap collector type.
In TS, congenital anomalies of the kidney and renal-urinary tract (CAKUT) can manifest as hemiplegic, neoplastic, and polycystic kidneys. While most patients with horseshoe kidneys have normal kidney function, renal hypoplasia may lead to impaired renal function. X-structural abnormalities were observed in 68.7% of patients with a non-mosaic 45,X karyotype and in 9.0% of patients with a 45,X mosaic karyotype. In those with 45,X monosomy, 45,X with mosaicism, and X-structural abnormalities, the CAKUT incidence was 11.5%, 7.4%, and 25.0%, respectively, indicating a reduced ability to form kidneys with non-mosaic X chromosome abnormalities [
112].
6. Skeletal Abnormalities and Short Stature
Girls with TS often suffer from reduced bone density and delayed bone formation owing to estrogen deficiency during adolescence [
126,
145]. Osteopenia or osteoporosis are identified as common factors for problems in bone formation [
126,
127,
128,
129,
130]. Growth retardation of the joints of the finger bones was also noticeable in patients with TS compared with normal controls. This difference in bone formation between patients with TS and normal controls is minor until the age of 10 years, but becomes more significant during puberty [
125].
Bone density analysis showed decreased bone density in patients with TS in various areas [
120,
121]. For example, bone mineral apparent density (BMAD) in patients with TS was significantly lower in the femoral neck—an area of predominantly cortical bone—than in normal controls [
120,
122]. In addition, proximal radius and cortical volumetric bone mineral density (vBMD) exhibited a decreasing trend in cortical thickness [
120,
123]. BMD was maintained predominantly in trabecular bone, and BMD in the lumbar spine, an area rich in trabecular bone, was not significantly different between TS and control groups [
120]. Women with TS also showed low BMAD in the cortical and trabecular bone of the forearm [
124], and the width of the ultradistal radius (predominantly in the trabecular bone) was reduced [
122].
7. Brain Abnormalities
While no visible brain abnormalities are apparent, structural, electrophysiological, cognitive, and psychosocial studies have reported differences between patients with TS and normal control. Reiss et al. suggested that the brain structure of women with TS could be distinguishable from that of age-matched controls [
160]. Several other studies also suggested that patients with TS had a small volume of cerebral hemispheres and an increased volume of cerebrospinal fluid and the fourth ventricle [
161,
162]. The size of gray and white matter mainly determines brain volume and size. When comparing patients with TS against controls, although not statistically significant, there was an increase in gray matter in the right superior temporal gyrus and left amygdala and an increase in white matter in the left superior temporal gyrus [
163]. However, many reports also suggested that the brain structure was smaller than that of the control group. Compared with that of controls, in individuals with TS, there is a reduction in gray matter in various regions, including the right calcarine cortex, precentral region, supramarginal gyri, cuneus, lingual cortex, superior parietal, rostral anterior portion, pericalcarine, and postcentral and precuneus of the right hemisphere’s cingulate cortex, as well as a reduction in white matter in the entorhinal cortex, pars opercularis, frontal pole, and occipital lobe [
164,
165,
166]. Most gray matter reductions are related to surface area reduction [
164].
8. Relevance to X Chromosome Inactivation and Escape Genes
During the early development of mammals, one of the two X chromosomes in females (XX) is randomly inactivated by X chromosome inactivation (XCI), by which the total amount of X-linked genes expressed in females becomes equivalent to that in males (XY) [
185,
186]. Normal female somatic cells contain one active X chromosome (Xa) and one inactive X chromosome (Xi), resulting in a XaXi state. If X-linked genes in the Xi are completely silenced, the removal of Xi from XaXi may not have a harmful effect on cells. However, in TS the complete or partial loss of the Xi leads to a myriad of abnormalities. This is because some genes located outside the condensed heterochromatin of the Xi can escape from inactivation and be expressed, leading to differences in the number of expressed X-linked genes between 46,XaXi and 45,Xa states. These genes that are expressed from the Xi are called escape genes [
187,
188]. Approximately 15% and 3% of X-linked genes in humans and mice, respectively, are escape genes [
188]. Human X chromosomes have pseudoautosomal regions (PARs) that behave like autosomes where crossing over strictly occurs (
Table 1). Genes within PARs on the X chromosome usually escape from XCI [
155]. The PAR1 genes, including
SHOX, play essential roles in the phenotypic traits associated with TS, including short stature, Madelung’s wrist deformity, and intellectual disabilities [
9,
10]. Variations in the expression of these genes may contribute to growth deficits or increased height in affected individuals. Decreased expression of
SHOX contributes to growth deficits observed in patients with TS, whereas increased expression in Klinefelter syndrome (47,XXY), Triple X (47,XXX), and Double Y (47,XYY) is associated with increased height [
11].
In addition, 12 genes (AKAP17A, ASMT, ASMTL, CD99, CD99P1, CRLF2, CSF2RA, DHRSX, FABP5P13, GTPBP6, IL3RA, PLCXD1, PPP2R3B, P2RY8, SHOX, SLC25A6, XG, and ZBED1) located outside the PAR1 region have a single functionally Y homolog and are broadly expressed in human tissues [
12]. USP9X genes on the X chromosome could evade Xi and be expressed in both human adult and embryonic tissues [
53]. Quilter et al. found that the expression of escape genes, USP9X and ZFX, was associated with immune cell development, oocyte growth, and ovarian development [
54].
Variants of the
KDM6A gene, known to escape XCI, are also associated with Kabuki syndrome, a multisystem syndrome with TS-like phenotypic traits, such as growth delay, short stature, varying degrees of intellectual disabilities, skeletal and renal abnormalities, and congenital heart defects [
189,
190].
RPS4X and
RSPS4Y are also considered dosage-sensitive genes, and several studies reported
RPS4X downregulation in TS [
17,
18,
19]. Wang et al. identified 25 upregulated and 60 downregulated genes in patients with TS compared with those in normal women and found five genes, including
CD99, CSF2RA, MYL9, MYLPF, and
IGFBP2, possibly involved in the pathogenesis of TS [
20]. In addition, epigenetic mechanisms, such as DNA methylation, are also involved in the etiology of TS [
191]. However, further studies are required to understand the correlation between escape genes and TS.
This entry is adapted from the peer-reviewed paper 10.3390/cells12101365