2. Life Cycle of Schistosoma haematobium
The life cycle of
S. haematobium passes through two phases, asexual and sexual, which involve infection of the snail intermediate host and the vertebrate definitive host, respectively. Typically, the cycle starts when eggs released with urine from an infected host come into contact with a freshwater body harbouring snails belonging to the genus
Bulinus. The eggs hatch immediately to release free-swimming miracidia that penetrate the host. Upon successful establishment, these develop asexually through several stages into cercariae that leave the snail in search of the definitive host. While having a very short life span, a single miracidium established in a suitable snail host produces about 200 cercariae daily
[19][20][19,20]. Cercariae penetrate the skin of suitable definitive hosts who come into contact with the contaminated water body, whereupon they transform into schistosomula. Usually, this penetration takes place in surface water, where people and livestock congregate daily for domestic and recreational purposes
[21]. The schistosomula migrate through the epidermis and dermis, entering the blood to home to the lungs
[20][22][23][24][20,22,23,24]. Subsequently, schistosomula exit the lungs to the left side of the heart through the pulmonary veins and enter the abdominal aorta, where they either pass through the coeliac trunk, the inferior and superior mesenteric arteries, or the iliac arteries to reach the portal veins of the liver
[24]. Here, schistosomula lose their migratory ability, grow, and develop into adult male and female pairs
[24]. Thereafter, a pair travels against the blood flow in the venous circulation, settles in the vesical venous plexus and produces eggs that migrate to the bladder, ureter, and other parts of the urinary tract
[20][24][20,24]. These eggs permeate the walls of blood vessels, bladder, or genital organs
[24]. Those that access the bladder are passed out with urine into a body of freshwater, where hatched miracidia continue the transmission cycle
[20]. Other
Schistosoma species follow a similar life cycle, but with different predilection sites and egg morphologies
[25][26][25,26].
3. Zoonotic Schistosomiasis
The terms zoonosis or zoonotic disease are used to classify a range of infectious diseases and their causative agents that are capable of being transmitted and subsequently established between human and animal hosts
[27]. Hence, zoonotic schistosomiasis refers to the disease condition in which a
Schistosoma species known to affect a particular human or animal host is found in another host not specific to the schistosome group
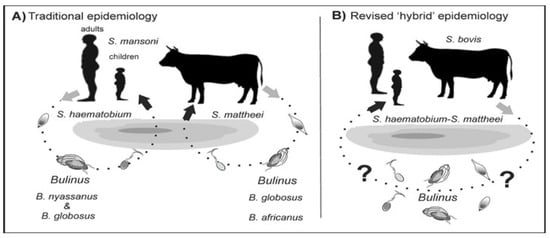
[13][28][13,28]. These species are naturally shared between humans and other animal hosts as a result of extensive mixed interactions at transmission sites
[29][30][29,30] (
Figure 1).
Figure 1. Alternative models of schistosome transmission. (
A) = conventional model of urogenital schistosomiasis transmission. (
B) = revised model of urogenital schistosomiasis with overlapping transmission potentials between multi-specific schistosomes.
? = putative but unconfirmed transmission involving known intermediate hosts of several
Schistosoma species. Modified from
[5].
Hybridization could also be established in areas where schistosome species are explicitly endemic or exhibit greater geographical overlap across potential hosts
[31][32][31,32]. These inter-host interactions between schistosomes can be bidirectional, whereby both the male and female schistosome pairs with the female or male of another pair to produce viable hybridized offspring
[28], or unidirectional in which pairing is between either the male or female schistosomes
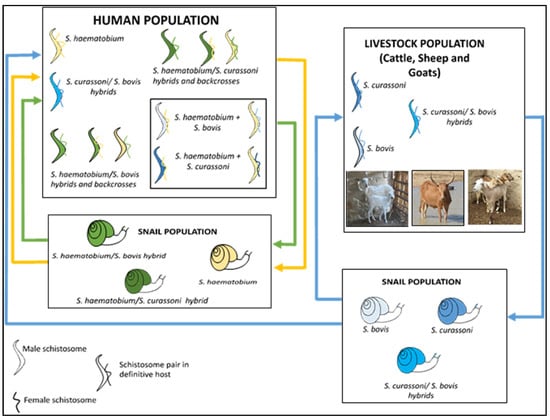
[33][34][33,34] (
Figure 2).
Figure 2. Zoonotic hybrid schistosome system proposed to occur in West Africa, including Nigeria
[34]. Human schistosome species are shown as yellow, animal schistosome species are shown as blue, and hybrids between animal and human schistosome species are shown as green, with infected snails also represented with corresponding colours.
4. Schistosomiasis Control Programme in Nigeria
The National Control Schistosomiasis Programme was established by the Federal Government of Nigeria in 1988, following which epidemiological surveying revealed that an estimated 20 million people were infected. Five pilot control projects were initiated in the states of Borno, Ebonyi, Katsina, Kwara, and Ondo, which have varying ecological predispositions to schistosomiasis. However, due to limited funds, the successes of these pilot projects have fallen short of initially planned targets. In 2020, the Carter Center incorporated schistosomiasis control activities into an ongoing onchocerciasis eradication programme in Plateau and Nasarawa states
[35]. A decade before this, mass administration of praziquantel (MDA) commenced in other states with the support of the WHO, UNICEF, and other non-governmental development organizations. To date, planning and implementation of MDA occur within implementation units (IUs), which may be a district, province, or local government area
[9]. In common with policy for combatting soil-transmitted helminth infections
[36], disease prevalence and other population data generated at the community level are usually aggregated at IUs. For schistosomiasis, this information is used to determine praziquantel thresholds to be implemented
[37].
MDA takes place biannually for all school-age children in districts where schistosomiasis prevalence is above 50%. MDA occurs annually when the prevalence is between 10 and 49.9%, and biennially when the prevalence is between 1 and 10%
[9]. However, recent WHO guidelines on schistosomiasis risk classification have revised these recommendations as follows. In endemic communities with the prevalence of
Schistosoma spp. infection ≥ 10%, in order to control schistosomiasis morbidity and advance towards eliminating the disease as a public health problem, the WHO recommends annual preventive chemotherapy with a single dose of praziquantel at ≥75% treatment coverage in all age groups from 2 years old, including adults, pregnant women after the first trimester, and lactating women
[9]. In endemic communities with a prevalence of
Schistosoma spp. infection ≥ 10% that demonstrate a lack of an appropriate response to annual preventive chemotherapy, despite adequate treatment coverage (≥75%), the WHO suggests consideration of preventive chemotherapy biannually (twice a year) instead of annually
[38].
The review of schistosomiasis treatment data over recent years (2014–2021) shows that the number of districts treated is significantly lower than those requiring treatment. Treatment coverage was significantly lower in 2021 (during the height of the COVID-19 pandemic) than experienced in the previous 7 years. In addition, less than half of the districts met the 75% effective coverage threshold in the last 3 successive years (2019–2021). By endemicity, the proportion of districts with high prevalence (>50%) reduced from (n = 15, 3%) in 2014 to (n = 10, 2%) in 2021, and those with moderate prevalence (10–49%) reduced from (n = 305, 52%) in 2014 to (n = 294, 50%) in 2021. However, the proportion of districts with low prevalence (<10%) increased from (n = 263, 48%) in 2014 to (n = 279, 48%) in 2021
[39]. The poor coverage of praziquantel across the years is most likely connected to the availability of medicines and logistics required to drive mass treatment campaigns
[40]. This is particularly worsened by the myriad of issues surrounding the availability, motivation and retention of drug distributors/health workers who are major stakeholders in the campaign
[41]. These observations are in line with a 2021 global report on schistosomiasis treatment, as only 30% of people (i.e., 75.3 million of the 251.4 million Nigerians requiring praziquantel) were treated
[40].
The ongoing pandemic and efforts targeted at mitigating its impacts have decreased the provision of NTD interventions, particularly praziquantel medicines for schistosomiasis. Nevertheless, there is a need for more concerted efforts towards increasing coverage of medicines in line with achieving the 2030 global targets of the WHO NTD elimination roadmap. These include: (1) reducing the proportion of moderate and heavy intensity infections to <1% in 78 countries; (2) reducing by 50% the number of tablets required during MDA; and (3) increasing domestic financial support for MDA
[3][4][3,4]. Meeting these targets is largely dependent on increased community participation during MDA, with absolute geographical reach and high programme coverage
[42][43][44][45][42,43,44,45].
5. Implication of Hybridization for Schistosomiasis Control Efforts
The existence of hybrid schistosomes is of great concern to the schistosomiasis control programme in Nigeria, with possible implications for widening host range, increased transmission potential, altered pathology, and drug resistance
[46]. Interactions between different
Schistosoma species are known to improve reproductive capacity, as manifested by an increased number of parasite offspring, a faster maturation time, and a larger intermediate host range
[47][48][47,48]. A major concern is that with the emergence of hybrid schistosomes, the efficacy of praziquantel treatment might be lowered
[49]. This has been reported under both field and laboratory conditions for
S. mansoni [50][51][52][50,51,52] and was linked to the cryptic role played by hybridization. The success achieved by using this drug is therefore threatened by the outbreak of
Schistosoma hybrids
[5]. Furthermore, genetic diversity among the progeny of zoonotic schistosomes offers better phenotypic characteristics compared to those of either parent
[53], thereby enhancing the exploitation of the host. Certain genotypic traits of the zoonotic hybrid parasite show refined adaptations to better avoid recognition and to resist the host’s adaptive immune system, potentially giving rise to greater infectivity and unusual pathologies
[54]. Infection of multiple animal reservoir hosts by zoonotic hybrid schistosomes makes the elimination of the disease more challenging
[15][16][15,16]. The difficulty to control and prevent
Schistosoma hybrid infections in some endemic areas may be due to the ubiquitous presence of rodents, which serve as the reservoir host for many schistosome species, thereby readily enabling co-infection
[55]. The magnitude of the contribution of non-human mammalian hosts to the transmission of schistosomiasis remains understudied, especially for species other than
S. japonicum. This has been highlighted by the WHO, which recommends testing for
Schistosoma infections in non-human mammalian hosts
[38].