Arterial dysfunction is major risk factor for cardiovascular complications, and arterial stiffness is an independent risk factor in end-stage renal disease patients. As the distance from the heart increases, arterial stiffness (pulse wave velocity) becomes progressively more marked. This generates a centrifugal stiffness gradient, which leads to partial, continuous local wave reflections, which in turn attenuate the transmission of pulsatile pressure into the microcirculation, thus limiting the potentially deleterious outcomes both upstream (on the heart: left-ventricular hypertrophy and coronary perfusion) and downstream (on the renal and cerebral microcirculation: reduced glomerular filtration and impaired cognitive functions). The impact of arterial aging is greater on the aorta and central capacitive arteries, and it is characterized by a loss or reversal of the physiological stiffness gradient between central and peripheral arteries.
- arterial aging
- arterial stiffness
- elastic arteries
- muscular arteries
1. Introduction
2. Aging and Arterial Stiffness
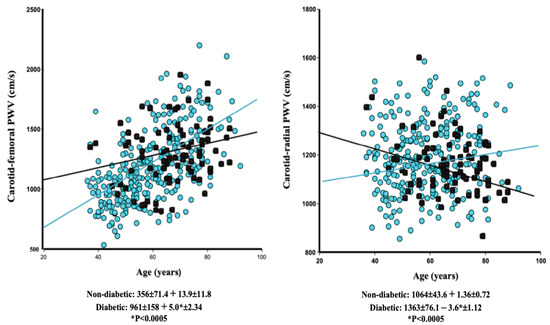
The characteristic physiologic, histologic, and molecular changes to aging arteries have been widely described and reviewed elsewhere [2][3][4][14][18][27][28][29][30][31][32][33][34][35][2,3,4,14,18,32,34,35,36,37,38,39,40,41]. The vessel wall is subjected to lifelong exposure to biomechanical and biochemical stressors. Biomechanical stress is, therefore, the consequence of a lifetime of continuous cycles of stretching and recoiling, during which shear stress and changes in wall tension lead to biomaterial fatigue, arterial remodeling, and deterioration of the vascular extracellular matrix (fragmentation and loss of elastin, accumulation and crosslinking of collagen, and an increased collagen/elastin ratio) [4][5][14][18][28][30][4,5,14,18,34,36]. VSMCs exhibit a high degree of plasticity, are prone to phenotype switching, and play a key role in arterial remodeling [4][5][18][29][31][4,5,18,35,37]. In physiologic conditions, VSMCs have a contractile phenotype that, with time, shifts toward a senescence-associated secretory phenotype. This activates microinflammation and oxidative stress, renews collagen synthesis, and triggers production of metalloproteinases, collagenases, and elastases, which in turn instigates an osteogenic program resulting in arterial wall calcification, as well as a decrease in VSMC division and numbers [28][29][30][31][32][33][34][35][34,35,36,37,38,39,40,41]. The age-related changes that come about in both elastic aortic segments and in muscular peripheral arteries are contingent on the specific properties of the arterial wall. Aortic stiffness increases steadily with age [12][13][14][15][16][20][21][22][25][12,13,14,15,16,20,21,22,25]. In younger individuals, stiffening of the aorta is significantly lower than that of peripheral arteries, thus explaining the significant ‘stiffness gradient’. However, with aging, stiffness of the aorta increases, while stiffening in the peripheral arteries remains unchanged or diminishes. This reduces the normal gradient—increasing stiffness as the distance from the heart increases—and leads to a progressively reduced or inversed stiffness gradient and, consequently, potential damage to the microcirculation (decline in kidney function, cognitive dysfunction, and vascular dementia) [15][16][17][18][19][22][23][24][25][15,16,17,18,19,22,23,24,25]. The progression of age-related stiffness is not uniform and varies with different clinical conditions, as well as environmental and genetic factors [4][11][23][25][26][4,11,23,25,26]. Certain individuals exhibit ‘accelerated arterial aging’ or ‘early vascular aging’, defined as arterial stiffness that is abnormally high for a given chronological age [36][42]. This is calculated from the intercept and slope of the age/arterial stiffness (typically cfPWV) correlation. Accelerated arterial aging is observed in several disease states (arterial hypertension, chronic kidney disease/ESRD, diabetes mellitus, and inflammatory diseases), and it is a reliable predictor of cardiovascular complications. ESRD is probably the most characteristic clinical hallmark of accelerated vascular aging [6][19][20][21][22][25][37][6,19,20,21,22,25,30]. This is illustrated by the significantly steeper slope (β coefficient) of the non-adjusted age–cfPWV correlation (Figure 1A) and confirmed by multiple stepwise regression (Table 1).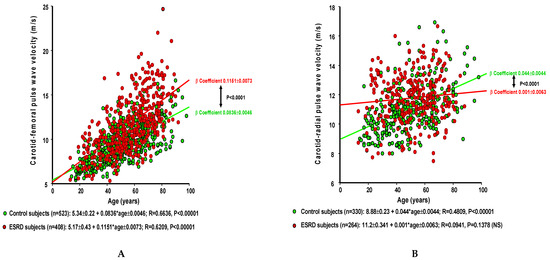
| A. Carotid–Femoral PWV (cm/s ± SEM) Multiple Regression Report in Control and ESRD Populations | |||||||
| Control Group (n = 526) 9.63 ± 2.13 |
ESRD Patients (n = 412) 11.67 ± 3.15 |
||||||
| A. Carotid–Femoral PWV (cm/s ± SEM) | |||||||||||||||||||||||
| Nondiabetic (n = 326) |
Diabetic (n = 83) |
||||||||||||||||||||||
| β Coefficient | p-Value | R2 | β Coefficient | p-Value | R2 | p-Value 1 vs. 2 |
|||||||||||||||||
| β Coefficient | p-Value | R2 | β Coefficient | p-Value | R2 | p | Age (years) | 6.4 ± 0.38 | <0.00001 | 0.2149 | 11.5 ± 0.65 | <0.00001 | 0.400 | <0.00001 | Mean BP (mmHg) | 3.45 ± 0.26 | <0.00001 | 0.130 | 3.7 ± 0.44 | <0.00001 | 0.09 | NS | |
| -Value | 1 vs. 2 | ||||||||||||||||||||||
| Age (years) | 14.80 ± 1.14 | <0.00001 | 0.3782 | 8.10 ± 2.50 | 0.0017 | 0.1131 | 0.0149 | ||||||||||||||||
| Mean BP (mmHg) | 4.48 ± 0.95 | <0.00001 | 0.0539 | 4.90 ± 1.75 | 0.0068 | 0.0833 | NS | Gender (female) | −44.20 ± 11.9 | 0.0002 | 0.0002 | ||||||||||||
| −1.1 ± 23.2 | 0.4830 p < 0.0001 |
0.0780 | 0.004 | NS | |||||||||||||||||||
| 0.1403 | p | < 0.001 | Heart period (ms) | −0.15 ± 0.04 | 0.0201 | 0.011 | −0.19 ± 0.008 | 0.0137 | 0.008 | NS | |||||||||||||
| 0.6140 p < 0.0001 |
|||||||||||||||||||||||
| B. Carotid–Radial PWV (cm/s ± SEM) | 0.4958 | ||||||||||||||||||||||
| Nondiabetic (n = 264) | Diabetic (n = 83) | p | < 0.0001 | ||||||||||||||||||||
| p | B. Carotid–Radial Pulse Wave Velocity (cm/s ± SEM) Multiple Regression Report in Control and ESRD Populations | ||||||||||||||||||||||
| β Coefficient | p-Value | R2 | β Coefficient | p-Value | R2 | p-Value 1 vs. 2 |
Control (n = 410) | ESRD (n = 343) |
|||||||||||||||
| Age (years) | 2.15 ± 0.66 | 0.0016 | 0.032 | −0.02 ± 1.00 | NS | 0.00005 | NS (0.0696) | β Coefficient | T Value | pValue | β Coefficient | T Value | pValue | pValue 1 vs. 2 |
|||||||||
| Age (years) | 3.05 ± 0.38 | 7.831 | <0.00001 | 1.73 ± 0.46 | 3.795 | 0.0002 | 0.0389 | ||||||||||||||||
| Mean BP (mmHg) | 3.85 ± 0.39 | 9.831 | <0.00001 | 5.00 ± 0.46 | 10.774 | <0.00001 | NS (0.056) | ||||||||||||||||
| Gender (female) | −42.9 ± 13.0 | −12.70 | 0.0073 | −34.42 ± 15.58 | −2.309 | 0.0205 | NS | ||||||||||||||||
| R2 = 0.4126 p < 0.00001 |
R2 = 0.2783 p < 0.00001 |
||||||||||||||||||||||
| Mean BP (mmHg) | |||||||
| 3.85 ± 0.53 | |||||||
| <0.00001 | |||||||
| 0.1656 | |||||||
| 4.70 ± 0.70 | |||||||
| <0.00001 | 0.3451 | NS | |||||
| 0.1792 p < 0.0001 |
0.4394 p < 0.0001 |