Vaccination has been identified as a critical method of disease control in the context of the current COVID-19 pandemic. The goal of this review is to search updated information on vaccine development and to identify areas of concern that require further research. WeThe researchers reviewed the literature on the development of COVID-19 vaccines, their efficacy, and use in special populations, as well as current vaccination strategies. To date, 170 vaccines are in clinical development, with 41 being already approved for use in various countries. The majority of vaccines approved for human use are vector-, subunit-, DNA-, or mRNA-based vaccines, or inactivated viruses. Because of the ongoing mutation of the SARS-CoV-2 virus, well-studied vector vaccines are losing relevance due to the ability of new virus strains to bypass neutralizing antibodies. Simultaneously, PS-based vaccines are becoming more popular. There is mounting evidence that the immunogenicity of COVID-19 vaccines is linked to their clinical efficacy. This has resulted in a shift in vaccination strategies, as well as the use of booster doses and revaccination. Furthermore, vaccination restrictions for children, pregnant women, the elderly, and people with chronic immunosuppressive diseases have been lifted, allowing more people to be vaccinated. New data on vaccine safety, including the incidence of serious adverse events, have been collected. Despite significant advances in the development of and research on COVID-19 vaccines, many questions remain that require further investigation.
- immunization
- prevention
- vector
- mRNA
- protein subunits
- COVID-19
- Introduction
1. Introduction
According to the World Health Organization (WHO), more than 628 million confirmed cases of coronavirus disease 2019 (COVID-19) and approximately 6.5 million COVID‑19 deaths had been reported worldwide as of 1 November 2022 [1].
As of 30 August 2022, Gibraltar (355.75 vaccine doses per 100 people), Chile (321.87 vaccine doses per 100 people), and Cuba (328.82 vaccine doses per 100 people) ranked first in terms of vaccine doses per person. According to WHO statistics, Gibraltar had 107 COVID‑19 deaths; Chile had 60,435; and Cuba had 8530 [5].
The vaccination of children and adolescents, the elderly, and pregnant women becomes increasingly important as time passes, as do determining the most effective vaccines and monitoring their efficacy to keep up with new virus mutations. This review discusses existing vaccine platforms and the main data available on the clinical use of vaccines in order to prioritize research.
This is an update to our previous review, which was published in December 2021 [6].
2. COVID-19 Vaccine Platforms and Their Characteristics
- COVID-19 Vaccine Platforms and Their Characteristics
As of 30 August 2022, the WHO reported that 198 vaccines were in preclinical trials and 170 vaccines were in clinical trials. Forty-five vaccines are currently in phase 3 clinical trials, with eleven being already in phase 4. In total, 23% are single-dose vaccines, while 56% are double-dose vaccines, and 1% are triple-dose vaccines. In total, 3% of vaccines are intended for oral administration, 8% for subcutaneous and intradermal administration, 7% for intranasal administration, and 1% for use as aerosols or inhalers. The intramuscular route is the most commonly used (82%) for vaccine administration [7].
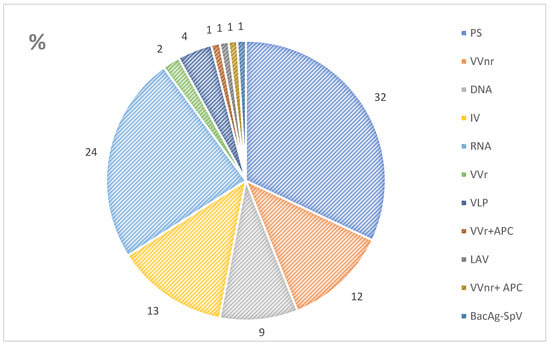
This review focuses solely on vaccines in clinical development. Figure 1 shows vaccine development platforms [7]. The most common vaccines in development are protein subunit (PS) vaccines, followed by ribonucleic acid (RNA) vaccines. These are followed by inactivated virus (IV) and non-replicating viral vector (VVnr) vaccines. Furthermore, replicating viral vector (VVr), virus‑like particle (VLP), live attenuated virus (LAV), and bacterial antigen-spore expression vector (BacAg-SpV) vaccines are being developed (Figure 1) [7].
- Immunogenicity and Safety of Vaccines
3. Immunogenicity and Safety of Vaccines
Vaccine effectiveness is determined by the induction of both humoral and cellular immune responses. As a result, quantifying neutralizing antibodies and the activity of specific T cells is recommended to assess vaccine efficacy and post-vaccination immunity [56,67,68]. According to mathematical modeling, post-vaccination neutralizing antibody titers are linearly related to vaccine efficacy [69]. The level of expression of each SARS-CoV-2 protein correlates with the prevalence and extent of CD4+ T cell responses to SARS-CoV-2 [70].
The ELISPOT platform is used by many researchers to assess the response of T cells induced by vaccination. T cell immune response was formed as early as 10 days after Sputnik Light vaccination, according to ELISPOT technology [54]. The ELISPOT-based Tigra Test SARS‑CoV-2 kit detected T cell immune response 90 and 120 days after Sputnik V immunization, including in seronegative individuals [71].
The efficacy of the main vaccines against the Omicron strain is of interest in light of the ongoing mutation of the SARS-CoV-2 virus [72]. Omicron (B.1.1.529) avoids many of the neutralizing antibody responses elicited by vaccines due to multiple mutations. In contrast to humoral immunity, vaccine-induced cellular immunity is highly reactive against the Omicron strain [73].
Immunogenicity can have a direct impact on vaccine safety and tolerability. In clinical trials, the incidence of adverse events was significantly higher after mRNA and vector vaccine administration (local reactions in 40–89% of cases and systemic reactions in 44–86% of cases) than after inactivated vaccine administration (injection-site reactions in 5–23% of cases and systemic reactions in 4–18% of cases) [74].
According to a meta-analysis, adverse events such as fever are more common after receiving inactivated vaccines, while headache and muscle pain are more common after receiving adenovirus vector-based vaccines, and 56% of people who received mRNA vaccines reported fatigue [75].
When the incidence of serious adverse events associated with BNT162b2, Ad26.COV2.S, and mRNA-1273 vaccinations was examined, the BNT162b2 vaccine had the highest reported incidence of myocarditis. The Ad26.COV2.S vaccine was more frequently linked to the development of Guillain–Barré syndrome. Thrombotic complications occurred more frequently with BNT162b2 and Ad26.COV2.S vaccination than with mRNA-1273 vaccination [43].
- Vaccinations of Various Populations
4. Vaccinations of Various Populations
6.1. General Population
4.1. General Population
COVID-19 mRNA vaccines (BNT162b2 and mRNA-1273) are recommended by the US Centers for Disease Control and Prevention (CDC) for primary and booster vaccinations in all populations. Currently, primary vaccination with one type of vaccine is recommended [76][19]. The WHO considers the following vaccines to be safe and effective: AZD1222; Ad26.COV2.S; mRNA-1273; BNT162b2; BBIBP-CorV; COVID-19 Vaccine (Vero Cell), Inactivated; BBV152; and NVX-CoV2373 (all trade names). In a clinical setting, these vaccines are equivalent, and healthcare professionals should use whichever option is available [55][20]. In patients under 60 years old, Australian guidelines prefer BNT162b2, mRNA-1273, or Novavax vaccines over AZD1222 [77][21]. As of July 2022, ten vaccines had been approved for use in Russia. A long-acting combination monoclonal antibody (tixagevimab + cilgavimab) can be used for pre-exposure prophylaxis of COVID-19 in adults and children (aged 12 years and older weighing at least 40 kg) who are not infected with SARS-CoV‑-2, have not been in contact with a person infected with SARS-CoV-2, and have contraindications for vaccination against COVID-19 [78][22].
6.2. Use in Pregnancy
4.2. Use in Pregnancy
The CDC and the WHO recommend any approved COVID-19 vaccination for those pregnant, breastfeeding, trying to get pregnant now, or planning to get pregnant in the future [55][20]. Russian national guidelines recommend Sputnik V vaccination for pregnant women if the benefit outweighs the risk. Vaccination is contraindicated while breastfeeding [79][23].
6.3. Children and Adolescents
4.3. Children and Adolescents
The CDC recommends the COVID-19 vaccination for anyone aged 6 months and older. BNT162b2 and mRNA-1273 are approved for use in children [76][19]. The WHO recommends starting the BNT162b2 vaccine at the age of five, and the mRNA-1273 vaccine at the age of twelve [62][24]. Vaccination is recommended for everyone over the age of five in Australia, [63][25] and over the age of twelve in Canada [80][26]. In Russia, the Gam-COVID-Vac-M vaccine is administered to children aged 12 to 17 [78][22].
6.4. People Who Have Had COVID-19
4.4. People Who Have Had COVID-19
The CDC recommends vaccination for all people over the age of six months, regardless of whether they have a history of symptomatic or asymptomatic SARS-CoV-2 infection [76][19]. The WHO also supports this strategy [55][20]. In Australia, vaccination is recommended no sooner than three months after infection confirmation [63][25]. In Russia, vaccination is recommended 6 months after the disease, based on epidemic indications (including in previously vaccinated individuals) [81][27].
6.5. Immunocompromised Patients
4.5. Immunocompromised Patients
For immunocompromised patients, the CDC recommends COVID-19 mRNA vaccines (BNT162b2 or mRNA-1273) for primary and booster vaccinations [76][19]. In this population, the WHO and Australian guidelines recommend additional doses of the BNT162b2 or mRNA-1273 vaccine [55,77][20][21]. Given the risk of more severe infection, Canadian guidelines recommend vaccinating patients with primary immunodeficiency with mRNA vaccines [82][28]. In Russia, the Sputnik V vaccine is recommended in this population. People with immunodeficiency who have had COVID-19 may receive Sputnik Light [81][27].
6.6. Booster Vaccination
4.6. Booster Vaccination
Booster vaccination and revaccination (seasonal vaccination) against COVID-19 are used to maintain active immunity against COVID-19 for a longer period of time after primary immunization. A booster is the administration of a vaccine with the same or a different antigenic composition before the previous vaccine’s immunogenic effect has worn off. The next booster dose of the vaccine should increase the intensity and duration of post-vaccination immunity. The timing of the booster vaccination ranges from three to six months, depending on the country’s legislative framework [77,81–84]. Revaccination (seasonal vaccination) against COVID-19 is performed 12 months after the main (primary) or booster vaccination [85].
As recently as late 2021, the need for booster doses of COVID-19 vaccines was debatable [6]. Lately, public opinion on vaccine booster administration has shifted in favor of mandatory administration of booster doses, as this increases immunity duration and resistance to the Omicron strain [40,86]. The CDC recommends a booster injection for patients over the age of 12, with the first booster being administered three months after primary immunization. In patients over the age of 50, the second booster should be administered four months after the first [76]. According to WHO recommendations, one booster dose is sufficient [55]. In Australia, a single dose of a COVID-19 vaccine booster is recommended for people aged 16 and older who have completed their primary course three months ago or more. The second booster is recommended for people over the age of 50, nursing-home residents, people with severe immunosuppression, people with significant disabilities, and people at risk of severe COVID-19 infection [77]. In Canada, booster doses are recommended from 18 years of age [82]. In the United Kingdom, booster immunization with BNT162b2 or mRNA-1273 is currently recommended three months after primary vaccination [84]. In Russia, vaccination with Sputnik Light, EpiVacCorona, and AURORA-CoV is recommended [81].
Some vaccines have only been approved for use as boosters. Only a booster dose of the BNT162b2 vaccine is recommended for adolescents aged 12 to 17 years [87]. In August 2022, the mRNA-1273.214/Moderna
TX vaccine was registered (Moderna, USA (mRNA-1273.214)). This is a bivalent mRNA vaccine containing sequences encoding SARS-CoV-2 and Omicron variant spike proteins [88]. A systematic review as of May 2022 found that three doses of RNA vaccines provided the best efficacy for vaccination and booster vaccination (96% vaccine efficacy; 95% CI, 72% to 99%). The combination of two adenovirus vector vaccines and one RNA vaccine has an efficiency of 88% (range: 59–97%). The homologous two-dose regimen of RNA vaccines results in 99% (79% to 100%) vaccine efficacy in preventing severe COVID-19. Triple-dose RNA vaccines are the most effective in reducing COVID-19-related hospitalizations (95% CI, 90% to 97%). Three-dose regimens of homologous and heterologous strains have been shown to be effective in preventing infection with the Alpha, Delta, and Omicron strains [89].
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 1 November 2022).
- Starshinova, A.; Malkova, A.; Zinchenko, U.; Kudlay, D.; Glushkova, A.; Dovgalyk, I.; Yablonskiy, P.; Shoenfeld, Y. Efficacy of Different Types of Therapy for COVID-19: A Comprehensive Review. Life 2021, 11, 753.
- Interim Statement on the Composition of Current COVID-19 Vaccines. Available online: https://www.who.int/news/item/17-06-2022-interim-statement-on--the-composition-of-current-COVID-19-vaccines (accessed on 30 August 2022).
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; Ortiz-Ospina, E.; et al. Coronavirus Pandemic (COVID-19). 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 30 August 2022).
- Available online: https://covid19.who.int/table (accessed on 31 August 2022).
- COVID-19 Vaccine Tracker and Landscape. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 1 November 2022).
- Kozlov, V.A.; Tikhonova, E.P.; Savchenko, A.A.; Kudryavtsev, I.V.; Andronova, N.V.; Anisimova, E.N.; Golovkin, A.S.; Demina, D.V.; Zdzitovetsky, D.E.; Kalinina, Y.U.S.; et al. Borisov. Clinical Immunology. In A Practical Guide for Infectious Disease Specialists; Polikor: Krasnoyarsk, Russia, 2021; p. 563.
- EMA. Clinical Evaluation of New Vaccines. European Medicines Agency. 2018. Available online: https://www.ema.europa.eu/en/clinical-evaluation-new-vaccines (accessed on 31 August 2022).
- Guidelines on Clinical Evaluation of Vaccines: Regulatory Expectations. Available online: https://www.who.int/publications/m/item/WHO-TRS-1004-web-annex-9 (accessed on 31 August 2022).
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211.
- Kudlay, D.; Kofiadi, I.; Khaitov, M. Peculiarities of the T Cell Immune Response in COVID-19. Vaccines 2022, 10, 242.
- The CanSino Biologics Ad5-nCoV-S COVID-19 Vaccine: What You Need to Know. Available online: https://www.who.int/news-room/feature-stories/detail/the--cansino-biologics-ad5-ncov-s--recombinant---covid-19-vaccine--what-you-need-to-know (accessed on 18 August 2022).
- Martynova, E.; Hamza, S.; Garanina, E.E.; Kabwe, E.; Markelova, M.; Shakirova, V.; Khaertynova, I.M.; Kaushal, N.; Baranwal, M.; Rizvanov, A.A.; et al. Long Term Immune Response Produced by the SputnikV Vaccine. Int. J. Mol. Sci. 2021, 22, 11211.
- Lapa, D.; Grousova, D.M.; Matusali, G.; Meschi, S.; Colavita, F.; Bettini, A.; Gramigna, G.; Francalancia, M.; Garbuglia, A.R.; Girardi, E.; et al. Retention of Neutralizing Response against SARS-CoV-2 Omicron Variant in Sputnik V-Vaccinated Individuals. Vaccines 2022, 10, 817.
- Liu, J.; Chandrashekar, A.; Sellers, D.; Barrett, J.; Lifton, M.; McMahan, K.; Sciacca, M.; VanWyk, H.; Wu, C.; Yu, J.; et al. Vaccines Elicit Highly Cross-Reactive Cellular Immunity to the SARS-CoV-2 Omicron Variant. medRxiv 2022, preprint.
- He, Q.; Mao, Q.; Zhang, J.; Bian, L.; Gao, F.; Wang, J.; Xu, M.; Liang, Z. COVID-19 Vaccines: Current Understanding on Immunogenicity, Safety, and Further Considerations. Front. Immunol. 2021, 12, 669339.
- Ashmawy, R.; Hamdy, N.A.; Elhadi, Y.A.M.; Alqutub, S.T.; Esmail, O.F.; Abdou, M.S.M.; Reyad, O.A.; El-Ganainy, S.O.; Gad, B.K.; El-Deen, A.E.-S.N.; et al. A Meta-Analysis on the Safety and Immunogenicity of COVID-19 Vaccines. J. Prim. Care Community Health 2022, 13, 21501319221089256.
- Guo, W.; Deguise, J.; Tian, Y.; Huang, P.C.E.; Goru, R.; Yang, Q.; Peng, S.; Zhang, L.; Zhao, L.; Xie, J.; et al. Profiling COVID-19 Vaccine Adverse Events by Statistical and Ontological Analysis of VAERS Case Reports. Front. Pharmacol. 2022, 13, 870599.
- Clinical Guidance for COVID-19 Vaccination|CDC. Available online: https://www.cdc.gov/vaccines/covid-19/clinical-considerations/interim-considerations-us.html (accessed on 31 August 2022).
- Coronavirus Disease (COVID-19): Vaccines. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-vaccines (accessed on 31 August 2022).
- Care AGD of H and A. ATAGI Clinical Guidance for COVID-19 Vaccine Providers. Australian Government Department of Health and Aged Care; 2021. Available online: https://www.health.gov.au/initiatives-and-programs/covid-19-vaccines/advice-for-providers/clinical-guidance (accessed on 31 August 2022).
- Temporary Guidelines for Prevention, Diagnosis and Treatment of Novel Coronavirus Disease (COVID-19) Version 16.pdf. Available online: https://static-0.minzdrav.gov.ru/system/attachments/attaches/000/060/193/original/%D0%92%D0%9C%D0%A0_COVID-19_V16.pdf (accessed on 30 August 2022).
- 05072021_MR_Preg_v4.pdf. Available online: https://static-0.minzdrav.gov.ru/system/attachments/attaches/000/057/333/original/05072021_MR_Preg_v4.pdf (accessed on 20 July 2022).
- Vaxart. A Phase 2, Double-Blind, Multi-Center, Randomized, Placebo-Controlled, Dose-Ranging Trial to Determine the Safety, Immunogenicity and Efficacy of an Adenoviral-Vector Based Vaccine Expressing Severe Acute Respiratory Syndrome (SARS-CoV-2) and dsRNA Adjuvant Administered Orally. clinicaltrials.gov; Report No.: NCT05067933. May 2022. Available online: https://clinicaltrials.gov/ct2/show/NCT05067933 (accessed on 14 August 2022).
- Vaxart COVID-19 Oral Vaccine. Available online: https://www.precisionvaccinations.com/vaccines/vaxart-covid-19-oral-vaccine (accessed on 15 August 2022).
- Public Health Agency of Canada. Archive 38: COVID-19 Vaccine Guidance Updates: Canadian Immunization Guide: June 21 2022. Available online: https://www.canada.ca/en/public-health/services/immunization/national-advisory-committee-on-immunization-naci/summary-updates-canadian-immunization-guide-june-21-2022-covid-19-vaccines.html (accessed on 31 August 2022).
- Temporary Guidelines. The Procedure for Vaccination against a New Coronavirus Infection (COVID-19). 2022. Available online: https://static-0.minzdrav.gov.ru/system/attachments/attaches/000/060/087/original/%D0%9C%D0%B5%D1%82%D0%BE%D0%B4%D0%B8%D1%87%D0%B5%D1%81%D0%BA%D0%B8%D0%B5_%D1%80%D0%B5%D0%BA%D0%BE%D0%BC%D0%B5%D0%BD%D0%B4%D0%B0%D1%86%D0%B8%D0%B8_02062022_%282%29.pdf?1655803717 (accessed on 18 August 2022).
- Public Health Agency of Canada. COVID-19 Vaccine: Canadian Immunization Guide. 2021. Available online: https://www.canada.ca/en/public-health/services/publications/healthy-living/canadian-immunization-guide-part-4-active-vaccines/page-26-covid-19-vaccine.html (accessed on 31 August 2022).
- Letter of the Ministry of Health of Russia. Dated December 22 2021 N 30-4/I/2-21694. On the Submission of Updated Temporary Guidelines. The Procedure for Vaccination against a New Coronavirus Infection (COVID-19). Available online: https://spboms.ru/sites/default/files/pismo_minzdrava_rossii_ot_22_12_2021_n_30-4_i_2-21694_o.pdf (accessed on 31 August 2022).
- COVID-19 Vaccination: Booster Dose Resources—GOV.UK. Available online: https://www.gov.uk/government/publications/covid-19-vaccination-booster-dose-resources (accessed on 31 August 2022).
- About Clarification of the Procedure for Re-Vaccination against COVID-19. Available online: http://www.7gsp.by/polezno-znat/stati/558-o-razyasnenii-poryadka-provedeniya-povtornoj-vaktsinatsii-protiv-covid-19 (accessed on 14 August 2022).
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546.
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; AlMukdad, S.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Tang, P.; Hasan, M.R.; Coyle, P.; et al. Effect of mRNA Vaccine Boosters against SARS-CoV-2 Omicron Infection in Qatar. N. Engl. J. Med. 2022, 386, 1804–1816.
- CDC. Coronavirus Disease 2019 (COVID-19). Centers for Disease Control and Prevention; 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-classifications.html (accessed on 31 August 2022).
- UK Grants World’s First Approval for Moderna’s Omicron Covid Vaccine. Bloomberg.com. 2022. Available online: https://www.bloomberg.com/news/articles/2022-08-15/uk-takes-world-s-first-step-toward-omicron-tailored-covid-shot (accessed on 25 August 2022).
- Au, W.Y.; Cheung, P.P.H. Effectiveness of heterologous and homologous COVID-19 vaccine regimens: Living systematic review with network meta-analysis. BMJ 2022, 377, e069989.