Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Matteo Ponzoni and Version 2 by Vivi Li.
Current treatment paradigms for end-stage dilated cardiomyopathy (DCM) in children include heart transplantation and mechanical support devices. However, waitlist mortality, shortage of smaller donors, time-limited durability of grafts, and thrombo-hemorrhagic events affect long-term outcomes. Moreover, both these options are noncurative and cannot preserve the native heart function. Pulmonary artery banding (PAB) has been reinvented as a possible “regenerative surgery” to retrain the decompensated left ventricle in children with DCM. The rationale is to promote positive ventricular–ventricular interactions that result in recovery of left ventricular function in one out of two children, allowing transplantation delisting.
- pulmonary artery banding
- dilated cardiomyopathy
1. Introduction
Pediatric heart failure (HF) represents an important cause of morbidity and mortality in childhood, with various causes (congenital, genetic, or acquired early in utero or after birth). Management of end-stage HF in infants and children remains challenging. The ultimate therapy for end-stage HF is heart transplantation (HTX). However, the survival rates after HTX are suboptimal since the patient’s prognosis drastically decreases with time, with the overall 25-year survival as low as 37% [1]. This makes pediatric HTX a not-so-appealing option, especially for infants or smaller children affected by end-stage HF, whose expectancy of life, given currently available treatment options, is drastically limited with respect to healthy peers.
2. Bedside: The Clinical Efficacy of PAB
After fifteen years from the first case report of the successful application of PAB in a 2-month-old baby with DCM [2][25], less than 20 centers worldwide have published their clinical results [3][4][5][6][28,29,30,31]. From these findings, what rwesearchers have learned is that PAB has a concrete potential to improve LV function in 30% to 80% of treated patients, when RV function is preserved. Early mortality is low (10%), comparable, or even inferior to that associated with HTX or MCS in infants [1][7][8][1,32,33]. No directly PAB-related deaths have been described so far. The most common causes of exitus in PAB nonresponders are progressive deterioration of LV function or lethal complications following MCS implantation, which has been implanted as a rescue strategy [3][4][28,29]. This is in keeping with the natural history of DCM, where one-year survival after diagnosis drops to 80% in high-risk profiles [9][34], regardless of medical and surgical therapies. The international experience with PAB was consolidated in a multicenter study, for a total of 70 patients from 15 institutions worldwide [4][29]. In this cohort, PAB was adopted as part of different surgical strategies. In nine children, PAB served as a recovery strategy to wean patients with DCM following major open-heart procedures, with eight out of nine patients experiencing recovery. In the remaining 61 cases, PAB was performed as an isolated short open-chest approach. Among the latter, 8 patients underwent PAB as a bridge to HTX as an alternative to MCS, while in 53 children, PAB was intended as a true potential “regenerative surgery”. Focusing on the 61 patients who received PAB as the sole operation, outcomes are encouraging. Overall medium-term mortality is confirmed to be modest (8/61, 13%), and the rate of complete LV recovery is brilliant (34/61, 56%). In addition, 8 patients (13%) experienced a partial improvement in LV function, while 13 patients (21%) required an HTX, as a planned strategy or because of PAB nonresponders. Updates regarding these numbers are expected to further support the promising early results. More recently, a multicenter US study enrolling 14 children banded at a median of 5 months of age highlighted some differences with respect to the German experience [5][30]. Functional recovery was achieved in 29% of cases (4/14 patients), while 8 patients underwent HTX and 2 expired. The authors hypothesized that the more compromised preoperative status of patients in the US cohort, as well as the substantial differences in HF etiologies (myocarditis in 40% of patients in the German registry vs. 0% in the US study), contributed to the lower observed recovery rate. In fact, PAB was attempted as a rescue strategy to prevent committing to high-risk ventricular assist device implantation [5][30]. In this view, it is not surprising that a supposed regenerative strategy (PAB) that relies on the residual repair potential of the native heart and organism would be less beneficial when performed “too late”. Moreover, LV noncompaction, which rwesearchers found as a possible contributing factor to PAB failure in researchers'our experience [6][31], was unusually frequent in the US cohort (5/14 patients, 39% vs. 8/61 cases, 13% in the world network report [4][29]), revealing the presence of a structural detrimental substrate, traditionally associated with relevant irreversible myocardial fibrosis [10][35], in a consistent quote of patients. Since 2015, rwesearchers have embarked on a surgical protocol alternative to HTX to treat pediatric end-stage HF [6][31], including PAB. So far, rwesearchers have treated with PAB a total of eight patients affected by DCM (four males, 50%) at a median age of 8 (5–10) months. In two cases (25%), the PAB strategy failed, and both patients required MCS with the Berlin Heart, followed by a successful HTX [6][31]. In one case (with a diagnosis of LV noncompaction and a known heterozygous mutation of the TPM1 gene and the ABCC9 gene), the PAB strategy was initially successful, allowing home discharge, but 3 months after PAB, the patient developed severe RV failure after acute pneumonia. Data regarding genetic testing in patients with DCM undergoing PAB are sparse in the scientific literature. The Giessen group never reported known mutations affecting their patients, nor gave specific recommendations on genetic testing before PAB. From the multicenter US cohort [5][30], only two patients were known to have genetic syndromes (including one patient with Leigh Syndrome and one patient with 12p duplication). In ouresearchers' center, genetic testing is always performed as part of the diagnostic protocol for patients with DCM. However, the decision to pursue the PAB strategy cannot benefit from such information, since the results of genetic tests require time, and patients usually necessitate a rapid treatment decision. The results of genetic testing are used to better guide the follow-up of patients and possibly predict the probabilities of recurrence of HF. As stated, only one patient in researchers'our cohort was found to possess a heterozygous mutation of the TPM1 gene (de novo) and the ABCC9 gene (parental). In four patients (50%) in ouresearchers' cohort, LV performance improved significantly, allowing transplantation delisting. In the remaining two patients (the most recent ones), LV function is still depressed, but clinical conditions are stable, and the patients are kept on an active transplantation waitlist (Figure 1). At a median follow-up time of 4.4 (1–5.4) years from PAB, all patients are alive and followed up regularly.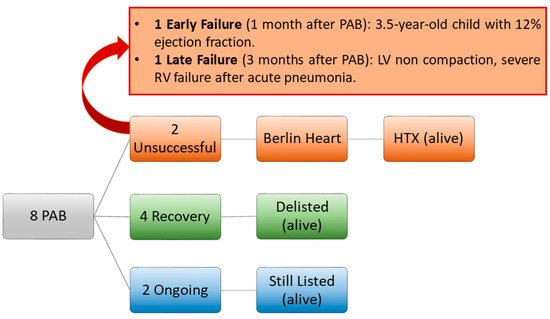
Figure 1.
Padova experience with PAB for LV rehabilitation in DCM since 2015. HTX: heart transplantation. PAB: pulmonary artery banding. RV: right ventricle.
3. Bedside: Caveats from Clinical Experience
3.1. Age
The neonatal heart is demonstrated to possess a robust capacity for myocardial tissue regeneration, through the presence of highly active cardiac progenitor cells [11][36]. In fact, the cardiac tissue harvested from patients with congenital heart diseases can spontaneously generate mesenchymal stem cells in vitro [12][37], which is indicative of a preserved endogenous capacity of myocardial repair. Unfortunately, this repair potential is age-dependent, with a progressive and marked reduction beyond one year of age [12][37]. There is evidence that the regeneration capacity of the adult mammalian heart is very limited, due to the incapacity of cardiomyocytes to proliferate in adulthood. However, this is not true in neonates and infants, where a residual or reversible potential for proliferation has been reported [11][36]. Clinical experience with infants with complex congenital heart disease (i.e., anomalous left coronary artery from the pulmonary artery) has shown that after early surgical repair (i.e., coronary reimplantation), a full myocardial recovery with normalization of LV function is possible even after myocardial ischemia [13][14][38,39]. In addition, experience with rapid two-stage arterial switch in infants affected by transposition of the great arteries, who are too old to undergo a successful arterial switch operation, has shown the possibility of LV myocardial recovery after PAB, which has been able to induce an increase in cardiac mass to allow an uneventful late repair [15][16][40,41]. While cardiomyocytes show robust replicative activity during embryonic and fetal development, with subsequent waves of proliferation [17][42], replication stops after birth, never to resume again, at least not significantly. Further cardiac enlargement occurs by cell hypertrophy. The withdrawal of cardiomyocytes from the cell cycle after birth profoundly impacts on the capacity of the mammalian heart to undergo repair after damage: in the mouse, loss of myocardial tissue in the fetal or early neonatal life is healed through the generation of new contractile tissue [18][43], while fibrosis and scarring predominate later. The reason why cardiomyocyte proliferation stops irreversibly after birth seems to be linked to biochemical and mechanical events occurring after birth, such as the increase in oxygen tension and oxidative stress [19][44], the lack of maternal factors [20][45], the changes in hormonal stimulation [21][46], and, most notably, pressure overload [22][47], as the hydrodynamic modifications occurring in the newborn circulation result in a significant increase in cardiac afterload. All these observations may suggest that the beneficial effects of PAB in young patients are related to the specific induction of acute afterload increase, with consequent cardiomyocytes proliferation and cardiac regeneration. An ancient organ size control pathway (Hippo signaling) specifically inhibits cardiomyocyte proliferation in the adult heart [23][24][48,49]. Regulating the balance between cell differentiation, proliferation, and apoptosis, the Hippo signaling pathway also governs cardiac fibroblasts’ function and, subsequently, heart fibrosis [25][50], together with the endothelial response to oxidative stress, inflammation, and angiogenesis [26][51]. For these reasons, the inactivation of the Hippo pathway has been proposed as part of the putative strategies to promote myocardial regeneration after an injury [27][52]. If proven, PAB might act on these molecular pathways, modifying intracardiac pressure parameters that are detected by the cardiac mechano-sensing apparatus, which can regulate the Hippo signaling [28][29][53,54]. In fact, the dystrophin–glycoprotein complex, which links the cytoskeleton of myocardial fibers to the extracellular matrix, can regulate the Hippo pathway by binding its principal effector YAP (Yes-associated protein), modulating cardiomyocyte proliferation in mice [28][53]. This protein is regulated by the mechanical stress and the extracellular matrix stiffness, which are obliviously affected by the pressure overload imposed by PAB on the RV chamber. In ouresearchers' experience, a possible cause of PAB failure is the age of patients [6][31]. Schranz et al. suggested a 6-year-old age limit for PAB in DCM [30][55]. However, reswearchers believe that a lower threshold should be applied. Relying on the repair ability of the young heart and the antiregenerative pathways that aging activates in the myocardium, researcherswe now consider PAB as a surgical option only in children under 1 year of age (Figure 2) [6][31]. A similar philosophy has emerged in the setting of retraining of the morphological LV in congenitally corrected transposition of the great arteries, where the maximal age threshold for patients to be considered for PAB has been lowered across the years. In 2005, Winlaw et al. observed that patients >16 years at PAB were unlikely to achieve a definitive anatomical repair [31][56]. Eight years later, Myers et al. described an increased risk of LV dysfunction when PAB was performed after 2 years of age [32][57]. In the most recent series, the median age at PAB is even below 1 year [33][58], reflecting a trend toward the anticipation of PAB in early infancy.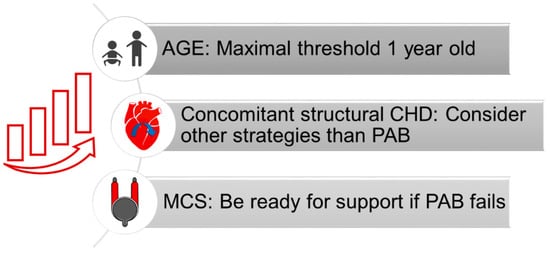
Figure 2.
Proposed strategies to improve patients’ outcomes. CHD: congenital heart defect. MCS: mechanical support device. PAB: pulmonary artery banding.