Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Vivi Li and Version 1 by Chandra Mohan.
Epigallocatechin-3-gallate (EGCG) is a polyphenol green tea catechin with potential health benefits and therapeutic effects in non-alcoholic fatty liver disease (NAFLD), a common liver disorder that adversely affects liver function and lipid metabolism.
- non-alcoholic fatty liver disease
- epigallocatechin-3-gallate
- green tea extracts
1. Introduction
Non-alcoholic fatty liver disease (NAFLD) is a chronic hepatic disorder characterized by excessive lipid accumulation in the liver, which is not secondary to alcohol consumption. NAFLD can progress to non-alcoholic steatohepatitis (NASH), fibrosis, and eventual liver cirrhosis, hepatocellular carcinoma, and liver failure [1]. Patients in certain risk categories, including obesity, type II diabetes, hyperlipidemia, insulin resistance, and those who consume high-fat diets (HFDs) are particularly prone to NAFLD. Approximately 20–33% of adults in the United States have NAFLD, resulting in an estimated annual economic burden of $103 billion in direct costs [2,3].
Non-alcoholic fatty liver disease (NAFLD) is a chronic hepatic disorder characterized by excessive lipid accumulation in the liver, which is not secondary to alcohol consumption. NAFLD can progress to non-alcoholic steatohepatitis (NASH), fibrosis, and eventual liver cirrhosis, hepatocellular carcinoma, and liver failure [1]. Patients in certain risk categories, including obesity, type II diabetes, hyperlipidemia, insulin resistance, and those who consume high-fat diets (HFDs) are particularly prone to NAFLD. Approximately 20–33% of adults in the United States have NAFLD, resulting in an estimated annual economic burden of $103 billion in direct costs [2][3].
Although there are no Food and Drug Administration-approved medications for NAFLD or NASH, some treatment strategies may reduce the manifestations of NAFLD. Diet and lifestyle modifications aid in limiting caloric intake, increasing physical activity, and improving liver histology. Various pharmacologic therapies regulate enzymatic activities in the liver, limit lipid formation, and prevent excessive inflammation and oxidative stress. However, most medications have had limited success or have substantial limitations, such as being unsustainable in long-term administration. Clinical trials of some medications failed to demonstrate high efficacy, whereas other studies evaluated only a small number of participants [4].
Green tea catechins are supplements that were widely studied over the past two decades for NAFLD. Green tea extracts (GTEs) are rich in flavonoids and possess prominent anti-inflammatory, antioxidative, and antilipidemic properties [5]. Epigallocatechin-3-gallate (EGCG) is the most commonly studied flavonoid because of its high abundance in green tea. Potential benefits of EGCG have been demonstrated in various in vitro and in vivo studies of animal models, and in various clinical trials of patients with NAFLD. In addition to its substantial benefits in NAFLD, EGCG also has positive effects in cancer, cardiovascular diseases, type II diabetes, and metabolic health, among others [6].
2. Findings from Rodent Studies
A wide range of analyses were performed in studies examining the effects of EGCG in rodent models. These studies explored clinicopathologic effects, lipid metabolism, carbohydrate metabolism, inflammatory markers, oxidative stress markers, and liver enzymes associated with EGCG treatment. In most studies, EGCG was delivered in the rodent chow.
2. Findings from Rodent Studies
A wide range of analyses were performed in studies examining the effects of EGCG in rodent models. These studies explored clinicopathologic effects, lipid metabolism, carbohydrate metabolism, inflammatory markers, oxidative stress markers, and liver enzymes associated with EGCG treatment. In most studies, EGCG was delivered in the rodent chow.Table 1 summarizes the characteristics and findings of the 30 rodent studies included in this review.
summarizes the characteristics and findings of the 30 rodent studies included in this entry.
Table 1.
Clinical Efficacy of EGCG Supplementation in Rodent Models.
| Study [Ref] | Model | EGCG Intake | Duration | Clinical/Pathological Outcome | Lipid Metabolism | Carbohydrate Metabolism | Inflammatory Markers | Oxidative Stress Markers | Liver Injury Enzymes | |
|---|---|---|---|---|---|---|---|---|---|---|
| Raederstorff 2003 [9] | Raederstorff 2003 [7] | HFD (R) | 0.25–1% (CD) | 4 weeks | ↑ Fecal fat/cholesterol/lipid excretion; ↔ Body weight, liver weight, food intake |
↓ TC, LDL, HDL, TG | ||||
| Fiorini 2005 [10] | Fiorini 2005 [8] | I/R (M) | 85 mg/kg (DW/IP) |
5 days | ↓ Body weight, steatosis; ↔ Food intake |
↓ FAS | ↑ GSH; ↔ UCP |
↓ ALT | ||
| Kuzu 2007 [11] | Kuzu 2007 [9] | HFD (R) | 1 g/L (DW) | 6 weeks | ↓ Body weight, liver weight, steatosis, inflammation; ↔ Degeneration, necrosis |
↓ TG; ↔ TC |
↓ Insulin, IR | ↓ MDA, CYP2E1; ↑ GSH |
↓ ALT; ↔ ALP, AST |
|
| Bose 2008 [12] | Bose 2008 [10] | HFD (M) | 3.2 g/kg (CD) | 16 weeks | ↓ Body weight, liver weight, MAT, VAT, EAT, RAT | ↓ TG; ↑ Fecal lipids |
↓ Glucose, insulin, IR | ↓ ALT | ||
| Lee 2008 [13] | Lee 2008 [11] | HFD (M) | 0.2–0.5% (CD) | 8 weeks | ↓ Body weight, EAT, VAT, RAT; ↔ Liver weight, energy intake |
↓ TC, LDL, PPAR-γ, FAS, LPL; ↑ CPT-I, HSL, ATGL |
↑ UCP-II | ↔ ALT, AST | ||
| Ueno 2009 [14] | Ueno 2009 [12] | NASH (M) | 0.05–0.1% (DW) | 42 weeks | ↓ Steatosis, intralobular fibrosis, ballooning; ↔ Body weight |
↓ TC, TG; ↔ FFA |
↓ Glucose | ↓ pAkt, pIKKß, pNF-κB | ↓ 8-OhdG | ↓ ALT; ↔ AST |
| Chen 2009 [15] | Chen 2009 [13] | HFD (R) | 1 mg/kg (DW) | 23 weeks | ↓ WAT;↑ Body weight; ↔ Food intake |
↑ PPAR-γ; ↔ TC, LDL, HDL, TG, SREBP-1C, PPAR-α, CPT-II, FAS, ACC |
↓ Glucose | ↑ UCP-II; ↔ ACO, MCD |
||
| Chen 2011 [16] | Chen 2011 [14] | HFD (M) | 0.32% (CD) | 17 weeks | ↓ Body weight, BAT, steatosis; ↔ Food intake |
↓ TG; ↑ Fecal lipids |
↓ Glucose, insulin, IR | ↓ ALT, HSL | ||
| Sae-tan 2011 [17] | Sae-tan 2011 [15] | HFD (M) | 0.32% (CD) | 15 weeks | ↓ Body weight, liver weight; ↔ Food intake |
↓ TG | ↓ Glucose, insulin | ↓ ALT | ||
| Sugiura 2012 [18] | Sugiura 2012 [16] | HFD (M) | 0.1% (DW) | 4 weeks | ↔ Body weight, liver weight, food intake, IPAT | ↔ TC, TG, FAS, CPT-II | ↔ ACO | |||
| Sumi 2013 [19] | Sumi 2013 [17] | HFD (R) | 0.01–0.1% (DW) | 7 weeks | ↓ Liver fibrosis, steatosis; ↔ Body weight, liver weight | ↓ TG | ↑ TNF-α, IL-6 | ↓ GPx-1, GST-P+, 8-OHdG, d-ROM; ↑ CAT |
↓ ALT | |
| Kochi 2013 [20] | Kochi 2013 [18] | HFD (R) | 0.1% (DW) | 9 weeks | ↓ Steatosis; ↑ Body weight |
↓ MDA, 8-OHdG, GST-P+, d-ROM, CYP2E1; ↑ GPx, CAT |
||||
| Xiao 2013 [21] | Xiao 2013 [19] | HFD (R) | 50 mg/kg (IP) | 8 weeks | ↓ Body weight, food intake, steatosis, fibrosis | ↓ TNF-α, COX-2 | ↑ GPx, CAT; ↔ SOD |
|||
| Krishnan 2014 [22] | Krishnan 2014 [20] | HFD (R) | 100 mg/kg (OG) | 30 days | ↓ Steatosis, inflammation | ↓ NF-κB, TNF-α | ||||
| Gan 2015 [23] | Gan 2015 [21] | HFD (M) | 10–40 mg/kg (IP) | 24 weeks | ↓ Energy intake, body weight, liver weight, steatosis, VAT; ↑ Hepatic cells |
↓ TC, TG, LDL; ↑ HDL |
↓ Glucose, insulin, IR, glucose intolerance | |||
| Ding 2015 [24] | Ding 2015 [22] | MCDD (M) | 25–100 mg/kg (IP) | 4 weeks | ↓ Body weight, liver weight, food intake | ↓ IL-1β, IL-6, TNF-α, MCP-1 | ↓ MDA; ↑ SOD |
↓ AST, ALT | ||
| Santamarina 2015 [25] | Santamarina 2015 [23] | HFD (M) | 50 mg/kg (DW) | 16 weeks | ↓ Body weight, WAT, ectopic fat, MAT; ↔ Liver weight, EAT, RAT |
↓ Glucose, insulin, IR | ↔ TNF-α, IL-6, IL-10, IL-6R, IL-10Rα | |||
| Mi 2017 [26] | Mi 2017 [24] | HFD (M) | 2 g/L (DW) | 16 weeks | ↓ Body weight, liver weight, BAT | ↓ TG, TC, LDL; ↑ HDL, PPAR-γ, ACC, SIRT-I, FAS, SREBP-1C, CPT-II, CPT-Iα |
↓ Glucose, insulin, IR; ↑ Glucose tolerance, insulin sensitivity |
|||
| Huang 2018 [27] | Huang 2018 [25] | HFD (M) | 3.2 g/kg (CD) | 33 weeks | ↔ Body weight, liver weight, food intake | ↓ LDL; ↑ HDL, HMGCR, PPARα; ↔ TG, FAS |
↓ Glucose | ↑ CYP7A1, CYP27A1 | ↓ ALT | |
| Yang 2018 [28] | Yang 2018 [26] | HFD (R) | 160 mg/kg (OG) | 11 weeks | ↓ Body weight, WAT, energy intake | ↓ TC, LDL, HDL, TG, NEFA | ↓ ALT, AST | |||
| Li 2018 [29] | Li 2018 [27] | HFD (R) | 25–100 mg/kg (CD) | 4 weeks | ↓ Liver weight | ↓ TC, LDL, TG, FFA, SREBP-II; ↑ HDL, SIRT-I, FOXO-I; ↔ HMGCR |
↓ MDA | ↓ ALT, AST | ||
| Sheng 2018 [30] | Sheng 2018 [28] | HFD (M) | 100 μg/g (CD) | 8 weeks | ↓ Body weight | ↓ TC, TG; ↔ LPL |
↓ ALP, ALT | |||
| Li 2018 [31] | Li 2018 [29] | HFD (m) | 50–100 mg/kg (IG) | 20 weeks | ↓ EAT; ↔ Body weight |
↓ LDL, TC, TG, CPT1α; ↑ HDL, ACC, FAS, ATGL |
↓ PPARα, ACO2; ↑ PPARγ, SREBP1 |
↓ UCP2 | ↑ HSL | |
| Ushiroda 2019 [32] | Ushiroda 2019 [30] | HFD (M) | 0.32% (CD) | 24 weeks | ↓ Body weight; ↔ Food intake |
↓ TG; ↔ LDL, HDL, TC, NEFA |
↓ ALT, AST | |||
| Hou 2020 [33] | Hou 2020 [31] | HFD (R) | 0.32% (CD) | 16 weeks | ↔ Body weight | ↓ FFA, TG, IR | ↓ IR | ↓ TNF-α, p-NF-κb, TRAF6, IKKβ, p-IKKβ, TLR4 | ||
| Dey 2020 [34] | Dey 2020 [32] | HFD (M) | 0.3% (CD) | 8 weeks | ↓ Body weight, liver weight, steatosis, ballooning; ↑ Energy intake |
↓ TC, TG; ↔ NEFA |
↓ Glucose, insulin, IR | ↓ TLR4, NF-κb, MCP-1, TNF-α | ↓ MDA | ↓ ALT |
| Ning 2020 [35] | Ning 2020 [33] | MCDD (M) | 50 mg/kg (IP/OG) | 2 weeks | ↔ Body weight | ↔ LDL, HDL, TC, TG | ↓ Glucose | ↓ ALT; ↔ AST |
||
| Yuan 2020 [36] | Yuan 2020 [34] | HFD (R) | 50 mg/kg (DW) | 92 weeks | ↓ Body weight; ↔ Food intake |
↓ TC, TG, LDL, FFA; ↔ HDL; ↑ CPT-II, FOXO1, SIRT1, FAS, ACC |
↓ Glucose, insulin | ↓ IL-6, TNF-α; ↑ NF-κB |
↓ ROS; ↑ CAT, SOD; ↔ MDA |
↓ ALT, AST |
| Huang 2020 [37] | Huang 2020 [35] | HFD (M) | 0.4% (CD) | 14 weeks | ↓ Body weight, EAT, PAT, MAT; ↔ Food intake |
↓ TC, LDL | ↓ Glucose | ↓ TNF-α, IL-6, LPS, MMP-3, COX-2, TLR4 | ↓ ALT, AST | |
| Du 2021 [38] | Du 2021 [36] | HFD (M) | 25–50 mg/kg (CD) | 16 weeks | ↓ Body weight, liver weight, steatosis | ↓ TG, HDL, TC; ↔ LDL |
↓ AST, ALT |
↑↓ indicates an increase or decrease in the value of the respective variable.
↔
indicates that no change occurred in that respective variable. Green font represents parameters that were increased; red font represents parameters that were decreased; blue font represents parameters that did not change, following EGCG treatment.
Abbreviations: 8-OHdG:
8-hydroxy-2’-deoxyguanosine;
ACC:
acetyl CoA carboxylase;
ACO:
acyl-CoA oxidase;
AKT:
protein kinase B;
ALP:
alkaline phosphatase;
ALT:
alanine aminotransferase;
AST:
aspartate aminotransferase;
ATGL:
adipose triglyceride lipase;
BAT:
brown adipose tissue;
CAT:
catalase;
CD:
chow diet;
COX:
cyclooxygenase;
CPT:
carnitine palmitoyl transferase;
CYP:
cytochrome;
d-ROM:
derivatives of reactive oxygen metabolites;
DW:
drinking water;
EAT:
epididymal adipose tissue;
EGCG:
epigallocatechin-3-gallate;
ET:
endotoxin;
FAS:
fatty acid synthase;
FFA:
free fatty acid;
FOXO1:
fork-head box O1;
GLUT4:
insulin-regulated glucose transporter;
GPx:
glutathione peroxidase;
GSH:
glutathione;
GST-P+:
glutathione S-transferase–positive;
HDL:
high-density lipoprotein;
HFD:
high-fat diet;
HMGCR:
3-hydroxy-3-methylglutaryl coenzyme A reductase;
HSL:
hormone-sensitive lipase;
IG:
intragastric;
IKK:
inhibitor of nuclear factor-κB kinase;
IL:
interleukin;
IP:
intraperitoneal;
IPAT:
intraperitoneal adipose tissue;
IR:
insulin resistance;
I/R:
ischemia/reperfusion;
LDL:
low-density lipoprotein;
LPL:
lipoprotein lipase;
LPS:
lipopolysaccharide;
M:
mouse;
MAT:
mesenteric adipose tissue;
MCD:
malonyl CoA decarboxylase;
MCDD:
methionine-and choline-deficient diet;
MCP:
monocyte chemoattractant protein;
MDA:
malondialdehyde;
MMP:
matrix metalloproteinases;
NASH:
non-alcoholic steatohepatitis;
NEFA:
non-esterified fatty acid;
NF:
nuclear factor;
OG:
oral gavage;
PAT:
peritoneal adipose tissue;
PPAR:
peroxisome proliferator receptor;
R:
rat;
RAT:
retroperitoneal adipose tissue;
SIRT:
sirtuin;
SOD:
superoxide dismutase;
SREBP:
sterol regulatory element binding protein;
TC:
total cholesterol;
TG:
triglycerides;
TLR:
toll-like receptor;
TNF:
tumor necrosis factor;
TRAF:
tumor necrosis factor receptor-associated factor;
UCP:
uncoupling protein;
VAT:
visceral adipose tissue;
WAT: white adipose tissue.
2.1. Clinicopathologic Effects
Body weight, liver weight, food intake, water intake, energy intake, and steatosis are common clinicopathologic metrics and metabolic risk factors. The majority of the studies reported a significant decrease in body weight after EGCG treatment [10,11,12,13,16,17,21,23,24,25,26,28,30,32,34,36,37,38] (
white adipose tissue.
2.1. Clinicopathologic Effects
Body weight, liver weight, food intake, water intake, energy intake, and steatosis are common clinicopathologic metrics and metabolic risk factors. The majority of the studies reported a significant decrease in body weight after EGCG treatment [8][9][10][11][14][15][19][21][22][23][24][26][28][30][32][34][35][36] (Table 1). A total of nine studies reported a reduction in liver weight [11,12,17,23,24,26,29,34,38]. In 10 of 11 studies, EGCG supplementation was associated with a significant decrease in the mass of various types of adipose tissue [12,13,15,16,23,25,26,28,31,37]. Lee et al. reported that EGCG led to dose-dependent suppression of genes associated with adipogenesis, such as peroxisome proliferator receptor-γ (PPAR-γ) and CCAAT enhancer-binding protein-α (C/EBP-α) [13].
All studies examining the effects of EGCG on steatosis found that EGCG significantly reduced steatosis, ballooning, and inflammation scores (
). A total of nine studies reported a reduction in liver weight [9][10][15][21][22][24][27][32][36]. In 10 of 11 studies, EGCG supplementation was associated with a significant decrease in the mass of various types of adipose tissue [10][11][13][14][21][23][24][26][29][35]. Lee et al. reported that EGCG led to dose-dependent suppression of genes associated with adipogenesis, such as peroxisome proliferator receptor-γ (PPAR-γ) and CCAAT enhancer-binding protein-α (C/EBP-α) [11].
All studies examining the effects of EGCG on steatosis found that EGCG significantly reduced steatosis, ballooning, and inflammation scores (
Table 1) [10,11,14,16,19,20,21,22,23,34,38]. Kuzu et al. reported decreases in steatosis and necrosis, associated with reduced α-smooth muscle actin (α-SMA) and cytochrome P450 2E1 (CYP2E1) levels [11]. Sumi et al. found that improvement of steatosis with EGCG was associated with inhibition of glutathione S-transferase-A placental form (GST-P)-positive foci, preneoplastic lesions associated with NAFLD [19]. Moreover, Gan et al. reported reduced steatosis accompanied by prominent hepatic cell regeneration, following EGCG administration [23].
2.2. Lipid Metabolism
Many studies reported significant decreases in total cholesterol (TC), triglycerides (TG), and low-density lipoprotein (LDL) (
) [8][9][12][14][17][18][19][20][21][32][36]. Kuzu et al. reported decreases in steatosis and necrosis, associated with reduced α-smooth muscle actin (α-SMA) and cytochrome P450 2E1 (CYP2E1) levels [9]. Sumi et al. found that improvement of steatosis with EGCG was associated with inhibition of glutathione S-transferase-A placental form (GST-P)-positive foci, preneoplastic lesions associated with NAFLD [17]. Moreover, Gan et al. reported reduced steatosis accompanied by prominent hepatic cell regeneration, following EGCG administration [21].
2.2. Lipid Metabolism
Many studies reported significant decreases in total cholesterol (TC), triglycerides (TG), and low-density lipoprotein (LDL) (Table 1). Significant decreases in TC were observed in 13 of 18 studies [9,13,14,23,26,28,29,30,31,34,36,37,38]; significant decreases in TG were reported in 18 of 22 studies [9,11,12,14,16,17,19,23,26,28,29,30,31,32,33,34,36,38]; and significant decreases in LDL were reported in 10 of 14 studies [9,13,23,26,27,28,29,31,36,37]. Thus, there is ample evidence indicating that EGCG exerts anti-hyperlipidemic effects.
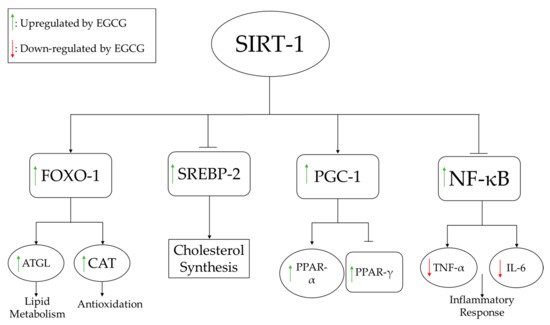
To understand the mechanisms underlying these lipid profile alterations, several pathways directly associated with lipid synthesis were evaluated at the molecular level. For example, Lee et al. examined the dose-dependent effects of EGCG on adipocyte differentiation genes and found that mRNA expression of PPARγ, C/EBP-α, lipoprotein lipase (LPL), and fatty acid synthase (FAS) decreased markedly following EGCG treatment and was highly correlated with a reduction of adipose tissue deposits [13]. Li et al. examined the effects of EGCG on several pathways, including the silent information regulator-1/forkhead box protein O1 (SIRT-1/FOXO1) pathway in conjunction with the regulatory gene, sterol regulatory element binding protein-2 (SREBP-2), which is responsible for regulating cholesterol synthesis [29]. As shown in
). Significant decreases in TC were observed in 13 of 18 studies [7][11][12][21][24][26][27][28][29][32][34][35][36]; significant decreases in TG were reported in 18 of 22 studies [7][9][10][12][14][15][17][21][24][26][27][28][29][30][31][32][34][36]; and significant decreases in LDL were reported in 10 of 14 studies [7][11][21][24][25][26][27][29][34][35]. Thus, there is ample evidence indicating that EGCG exerts anti-hyperlipidemic effects.
To understand the mechanisms underlying these lipid profile alterations, several pathways directly associated with lipid synthesis were evaluated at the molecular level. For example, Lee et al. examined the dose-dependent effects of EGCG on adipocyte differentiation genes and found that mRNA expression of PPARγ, C/EBP-α, lipoprotein lipase (LPL), and fatty acid synthase (FAS) decreased markedly following EGCG treatment and was highly correlated with a reduction of adipose tissue deposits [11]. Li et al. examined the effects of EGCG on several pathways, including the silent information regulator-1/forkhead box protein O1 (SIRT-1/FOXO1) pathway in conjunction with the regulatory gene, sterol regulatory element binding protein-2 (SREBP-2), which is responsible for regulating cholesterol synthesis [27]. As shown in
Figure 3, EGCG supplementation activates SIRT-1, which increases the expression of FOXO1 and decreases the expression of SREBP-2. Increased FOXO1 expression induces lipid metabolism and increases antioxidant (catalase) activity, whereas decreased SREBP-2 expression reduces fatty acid synthesis.
1, EGCG supplementation activates SIRT-1, which increases the expression of FOXO1 and decreases the expression of SREBP-2. Increased FOXO1 expression induces lipid metabolism and increases antioxidant (catalase) activity, whereas decreased SREBP-2 expression reduces fatty acid synthesis.
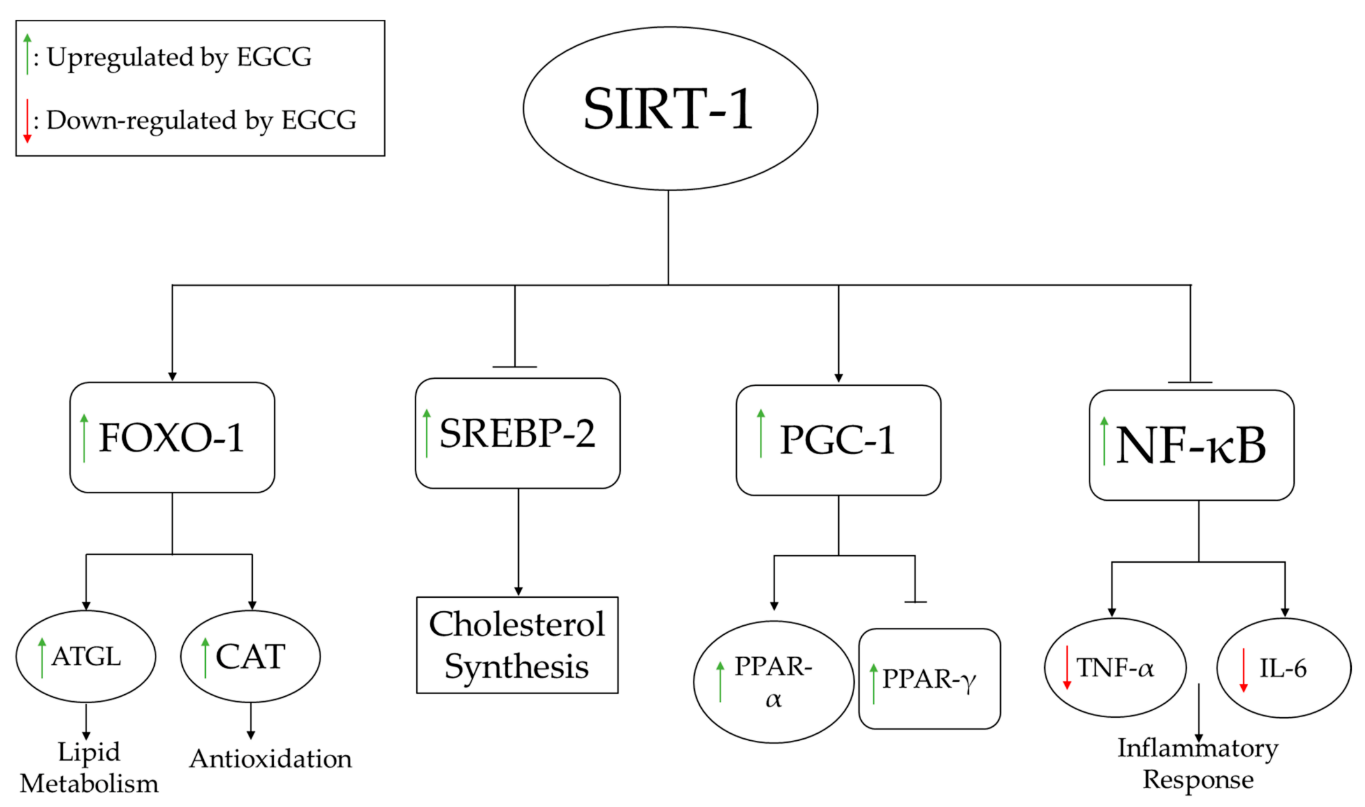
Figure 31.
EGCG-induced SIRT-1 modulation of lipid metabolism, antioxidant pathways, inhibition of fatty acid synthesis, and inflammatory response pathways. ATGL increases lipolysis of fats, while increased CAT boosts the antioxidant status. NF-kB regulates several pro-inflammatory pathways, including the production of inflammatory cytokines such as IL-6 and TNFα.
Abbreviations: ATGL:
adipose triglyceride lipase;
CAT:
catalase;
FOXO-1:
fork-head box O1;
IL:
interleukin;
NF-κB:
nuclear factor-κB;
PGC:
peroxisome proliferator-activated receptor-gamma coactivator;
PPAR:
peroxisome proliferator receptor;
SREBP:
sterol regulatory element binding protein;
TNF: tumor necrosis factor.
2.3. Carbohydrate Metabolism
It is important to consider the effects of EGCG on carbohydrate metabolism, as carbohydrate accumulation has detrimental effects on obesity and liver disease. Interestingly, all studies addressing the impact of EGCG on carbohydrate metabolism reported significant decreases in glucose and insulin levels, as well as insulin resistance (IR), with EGCG treatment [11,12,14,15,16,17,23,24,25,26,27,33,34,35,36,37] (
tumor necrosis factor.
2.3. Carbohydrate Metabolism
It is important to consider the effects of EGCG on carbohydrate metabolism, as carbohydrate accumulation has detrimental effects on obesity and liver disease. Interestingly, all studies addressing the impact of EGCG on carbohydrate metabolism reported significant decreases in glucose and insulin levels, as well as insulin resistance (IR), with EGCG treatment [9][10][12][13][14][15][21][22][23][24][25][31][32][33][34][35] (Table 1). Gan et al. showed in their study that intraperitoneal administration of EGCG dose-dependently alleviates hyperinsulinemia, hyperglycemia, and IR [23]. The improvement of these parameters can be related to the weight loss reported by these authors.
2.4. Inflammatory Markers
EGCG administration was shown to improve inflammatory profiles associated with liver damage. As shown in
). Gan et al. showed in their study that intraperitoneal administration of EGCG dose-dependently alleviates hyperinsulinemia, hyperglycemia, and IR [21]. The improvement of these parameters can be related to the weight loss reported by these authors.
2.4. Inflammatory Markers
EGCG administration was shown to improve inflammatory profiles associated with liver damage. As shown inTable 1, 11 studies examined changes in inflammatory markers with EGCG administration [14,19,21,22,24,25,31,33,34,36,37], 7 of which reported that EGCG reduced inflammation by decreasing pro-inflammatory cytokines [21,22,24,33,34,36,37]. Yuan et al. found that EGCG improved inflammation by decreasing tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6) in obese rats, which extended the lifespan of the animals [36]. As shown in
, 11 studies examined changes in inflammatory markers with EGCG administration [12][17][19][20][22][23][29][31][32][34][35], 7 of which reported that EGCG reduced inflammation by decreasing pro-inflammatory cytokines [19][20][22][31][32][34][35]. Yuan et al. found that EGCG improved inflammation by decreasing tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6) in obese rats, which extended the lifespan of the animals [34]. As shown in
Figure 3, activation of SIRT-1 by EGCG leads to inhibition of NF-κB, thereby inhibiting production of TNF-α and IL-6.
2.5. Oxidative Stress Markers
Oxidative stress, a common feature in NAFLD, is facilitated by the accumulation of visceral fat, and contributes to lipid peroxidation that induces systemic oxidative damage [39]. Thus, assaying oxidative stress markers is useful for assessing NAFLD treatment effectiveness. Several important oxidative stress markers were investigated in the studies included in this review, as listed in
1, activation of SIRT-1 by EGCG leads to inhibition of NF-κB, thereby inhibiting production of TNF-α and IL-6.
2.5. Oxidative Stress Markers
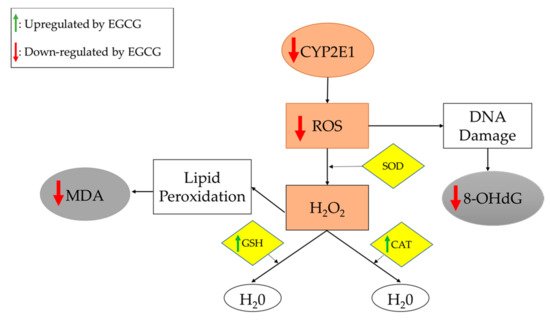
Oxidative stress, a common feature in NAFLD, is facilitated by the accumulation of visceral fat, and contributes to lipid peroxidation that induces systemic oxidative damage [37]. Thus, assaying oxidative stress markers is useful for assessing NAFLD treatment effectiveness. Several important oxidative stress markers were investigated in the studies included in this entry, as listed inTable 1. In 8 of 15 studies, EGCG administration was associated with significant decreases in pro-oxidants, such as CYP2E1 and reactive oxidative species (ROS), as well as oxidative end-products, such as 8-hydroxy-2’-deoxyguanosine (8-OHdG) and malondialdehyde (MDA) [11,14,19,20,24,29,34,36]. Furthermore, 6 of 10 studies reported significant increases in molecules involved in oxidation/reduction or detoxification reactions, including catalase (CAT), GST, and glutathione (GSH), upon EGCG administration [10,11,19,20,21,22]. Superoxide dismutase (SOD) is an enzyme that was evaluated in three studies in this review [21,24,36]. One study reported no changes in SOD [21], and the other two studies reported a significant increase in SOD [24,36], prompting the need for further studies. In this context, it should be pointed out that increased SOD may help remove superoxide radicals, while reduced SOD may also help by generating less H2O2 (see
. In 8 of 15 studies, EGCG administration was associated with significant decreases in pro-oxidants, such as CYP2E1 and reactive oxidative species (ROS), as well as oxidative end-products, such as 8-hydroxy-2’-deoxyguanosine (8-OHdG) and malondialdehyde (MDA) [9][12][17][18][22][27][32][34]. Furthermore, 6 of 10 studies reported significant increases in molecules involved in oxidation/reduction or detoxification reactions, including catalase (CAT), GST, and glutathione (GSH), upon EGCG administration [8][9][17][18][19][20]. Superoxide dismutase (SOD) is an enzyme that was evaluated in three studies in this entry [19][22][34]. One study reported no changes in SOD [19], and the other two studies reported a significant increase in SOD [22][34], prompting the need for further studies. In this context, it should be pointed out that increased SOD may help remove superoxide radicals, while reduced SOD may also help by generating less H2O2 (see
Figure 4).
2).
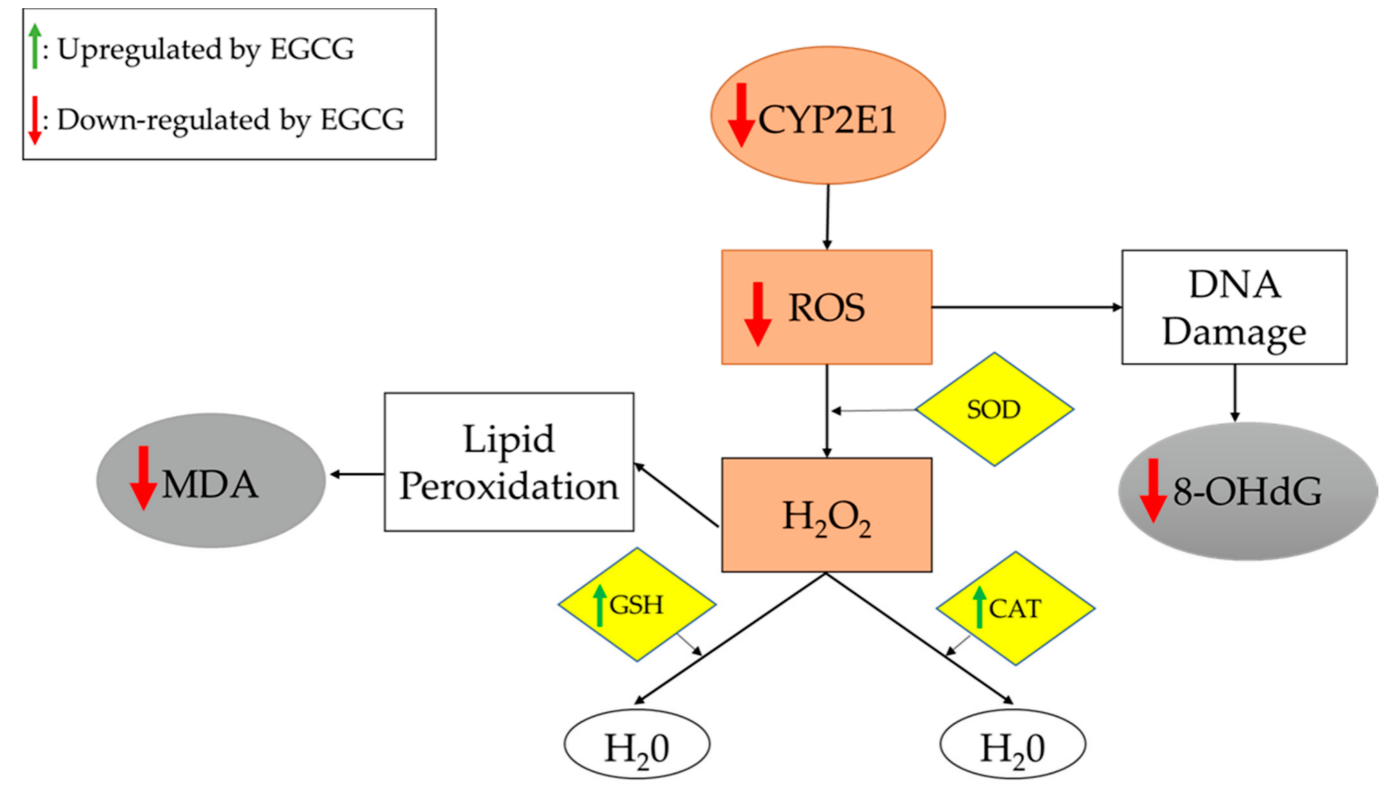
Figure 42.
Oxidative stress and antioxidation pathways. Gray boxes represent pro-oxidation end-products. Brown boxes represent pro-oxidation molecules. Yellow boxes represent antioxidation molecules. Reducing the production of H2O2 or increasing its breakdown will reduce the oxidant stress. EGCG appears to act via both mechanisms. The end result is reduced oxidative damage, as is evidenced by the reduced levels of MDA and 8-OHdG.
Abbreviations: 8-OHdG:
8-hydroxy-2’-deoxyguanosine;
CAT:
catalase;
CYP2E1:
cytochrome-2E1;
GSH:
glutathione;
MDA:
malondialdehyde;
ROS:
reactive oxidative species;
SOD: superoxide dismutase.
Kuzu et al. examined the effects of EGCG on oxidative stress associated with the CYP2E1 enzyme. These authors concluded that EGCG potentially suppresses CYP2E1-associated oxidative stress, as it decreases lipid peroxidation and increases GSH levels [11]. As shown in
superoxide dismutase.
Kuzu et al. examined the effects of EGCG on oxidative stress associated with the CYP2E1 enzyme. These authors concluded that EGCG potentially suppresses CYP2E1-associated oxidative stress, as it decreases lipid peroxidation and increases GSH levels [9]. As shown in
Figure 4, EGCG treatment reduces the expression of CYP2E1, leading to decreased synthesis of ROS (which damage DNA) and increased expression of antioxidants, which alleviate oxidative stress.
2.6. Biochemical Markers of Liver Damage
2, EGCG treatment reduces the expression of CYP2E1, leading to decreased synthesis of ROS (which damage DNA) and increased expression of antioxidants, which alleviate oxidative stress.
2.6. Biochemical Markers of Liver Damage
EGCG treatment also improves liver damage biomarkers [8][9][10][12][14][15][17][22][25][26][27][28][30][32][33][34][35][36]. As shown inTable 1, EGCG decreases levels of enzymes associated with liver damage, such as alanine aminotransferase (ALT), aspartate aminotransferase (AST), and alkaline phosphatase (ALP). Reductions in levels of these enzymes were associated with decreased steatosis.
3. Findings from Human Studies
As summarized in
, EGCG decreases levels of enzymes associated with liver damage, such as alanine aminotransferase (ALT), aspartate aminotransferase (AST), and alkaline phosphatase (ALP). Reductions in levels of these enzymes were associated with decreased steatosis.
3. Findings from Human Studies
As summarized inTable 2
, 21 studies evaluating catechins, green tea, and EGCG or GTE in humans with NAFLD also evaluated clinicopathologic findings, lipid and carbohydrate metabolism, inflammation, oxidative stress, and liver damage. The majority of these studies conducted their clinical trials over a 12-week period, designed as randomized, double-blind, and placebo-controlled trials (
Table 2
).
Table 2.
Clinical Efficacy of Green Tea in Human Studies.
| Study (Ref) | Study Design | Duration (Number of Participants) | Green Tea Component Daily Intake | Clinical/Pathological Outcome | Lipid Metabolism | Carbohydrate Metabolism | Inflammatory Markers | Oxidative Stress Markers | Liver Injury Enzymes | |
|---|---|---|---|---|---|---|---|---|---|---|
| Chantre 2002 [40] | Chantre 2002 [38] | Open study | 12 weeks (70) | 375 mg catechin | ↓ Body weight, WC | ↔TC | ||||
| Kovacs 2003 [41] | Kovacs 2003 [39] | (R/P/PC) | 13 weeks (104) | 323 mg EGCG | ↔ Body weight, BMI, REE, RQ | ↔ TG, NEFA | ↔ Glucose, insulin | |||
| Nagao 2004 [42] | Nagao 2004 [40] | (DB) | 12 weeks (38) | 690 mg catechin | ↓ Body weight, BMI, WC, HC | ↓ LDL; ↑ FFA; ↔ HDL, TG |
↑ Glucose, insulin | ↓ MDA | ||
| Nagao 2006 [43] | Nagao 2006 [41] | (R/DB) | 12 weeks (240) | 583 mg catechin | ↓ Body weight, BMI, WC, HC; ↔ Energy intake |
↓ LDL; ↔ HDL, TC, TG, FFA |
↔ Glucose | ↔ ALP | ||
| Auvichayapat 2007 [44] | Auvichayapat 2007 [42] | (R) | 12 weeks (60) | 750 mg green tea | ↓ Body weight, BMI; ↑ REE; ↔ Food intake, physical activity, RQ |
|||||
| Hill 2007 [45] | Hill 2007 [43] | (R/PC) | 12 weeks (38) | 300 mg EGCG | ↓ Total body fat, WC; ↔ Body weight, energy intake, EE, BMI, HC |
↔ Glucose, insulin | ||||
| Hsu 2008 [46] | Hsu 2008 [44] | (R/DB/PC) | 12 weeks (78) | 1200 mg GTE | ↓ WC, HC; ↔ Body weight, BMI |
↓ LDL, TG; ↑ HDL; ↔ TC |
↔ Insulin, IR | ↔ AST | ||
| Matsuyama 2008 [47] | Matsuyama 2008 [45] | (R/DB) | 36 weeks (40) | 75–576 mg catechins | ↔ Body weight, BMI, HC | ↓ TG, FFA | ↓ Glucose | ↑ CRP | ↓ AST, ALT | |
| Maki 2008 [48] | Maki 2008 [46] | (R/DB/C) | 12 weeks (107) | 625 mg EGCG | ↓ Body weight; ↔ Physical activity, energy intake, WC |
↓ TG, FFA; ↔ LDL, HDL |
↔ Glucose, insulin | ↔ CRP | ↔ MDA | |
| Brown 2009 [49] | Brown 2009 [47] | (R/DB/PC/P) | 8 weeks (88) | 800 mg EGCG | ↔ BMI, WC | ↔ TC, HDL, LDL, TG | ↔ Insulin, IR | |||
| Pierro 2009 [50] | Pierro 2009 [48] | (R) | 90 days (100) | 300 mg GTE | ↓ Body weight, BMI | ↓ TG, LDL, TC; ↑ HDL | ↓ Glucose, insulin | |||
| Basu 2010 [51] | Basu 2010 [49] | (R/C) | 8 weeks (35) | 440 mg EGCG | ↔ WC | ↔ TG, HDL | ↔ Glucose | ↔ IL-6, IL-1β, sVCAM-1, CRP | ↔ AST, ALT | |
| Basu 2010 [52] | Basu 2010 [50] | (R/C/SB) | 8 weeks (35) | 900 mg EGCG in capsule | ↔ Body weight, BMI, WC | ↓ TC, LDL; ↔ TG |
↔ Glucose, IR | ↓ MDA | ||
| Thielecke 2010 [53] | Thielecke 2010 [51] | (R/DB/PC/X) | 3 days (12) | 300–600 mg EGCG in capsule | ↔ EE, RQ | ↔ NEFA | ↔ Glucose, insulin | |||
| Brown 2011 [54] | Brown 2011 [52] | (R/PC/X) | 6 weeks (70) | 800 mg catechins | ↑ Energy intake; ↔ Body weight |
↓ LDL; ↔ HDL, TG |
↔ Glucose, insulin | |||
| Bogdanski 2011 [55] | Bogdanski 2011 [53] | (DB/PC) | 3 months (56) | 379 mg GTE | ↔ BMI, WC | ↓ TC, LDL, TG; ↑ HDL |
↓ Glucose, insulin, IR | ↓ CRP, TNF-α | ↑ TAS | |
| Suliburska 2012 [56] | Suliburska 2012 [54] | (R/DB/PC/C) | 3 months (46) | 379 mg GTE | ↓ BMI, WC | ↓TC, LDL, TG; ↔ HDL |
↔ Glucose | ↑ TAS | ||
| Mielgo-Ayuso 2013 [57] | Mielgo-Ayuso 2013 [55] | (R/DB/PC) | 12 weeks (88) | 300 mg EGCG | ↓ Body weight, BMI, WC | ↓ TC, LDL, HDL; ↔ TG |
↓ Insulin, IR | ↓ AST; ↔ ALT |
||
| Pezeshki 2016 [58] | Pezeshki 2016 [56] | (R/DB/PC) | 90 days (80) | 500 mg GTE | ↓ Body weight, BMI | ↓ AST, ALT, ALP | ||||
| Hussain 2017 [59] | Hussain 2017 [57] | (R/PC) | 91 days (80) | 500 mg GTE | ↓ Body weight, BMI | ↓ TC, LDL, TG; ↑ HDL |
↓ IR | ↓ CRP | ↓ AST, ALT | |
| Roberts 2021 [60] | Roberts 2021 [58] | (R/DB/PC) | 8 weeks (27) | 580 mg GTE | ↔ Body weight, BMI, EE, WC | ↔ TC, TG, LDL, HDL, FFA | ↔ALT, AST, ALP |
↑↓
indicates an increase or decrease in the value of the respective variable.
↔
indicates that no change occurred in that respective variable. Green font represents the parameters that were increased; red font represents the parameters that were decreased; blue font represents parameters that did not change, following EGCG treatment.
Abbreviations: ALP:
alkaline phosphatase;
ALT:
alanine aminotransferase;
AST:
aspartate aminotransferase;
BMI:
body mass index;
C:
controlled;
CRP:
C-reactive protein;
DB:
double-blind;
EE:
energy expenditure;
EGCG:
epigallocatechin-3-gallate;
FFA:
free fatty acid;
GTE:
green tea extract;
HC:
hip circumference;
HDL:
high-density lipoprotein;
IL:
interleukin;
IR:
insulin resistance;
LDL:
low-density lipoprotein;
MDA:
malondialdehyde;
NEFA:
non-esterified fatty acid;
P:
parallel;
PC:
placebo controlled;
R:
randomized;
REE:
resting energy expenditure;
RQ:
respiratory quotient;
sVCAM:
circulating vascular adhesion molecule;
TAS:
total antioxidant status;
TC:
total cholesterol;
TG:
triglycerides;
TNF:
tumor necrosis factor;
WC:
waist circumference;
X: cross-over trial.
3.1. Clinicopathologic Effects
cross-over trial.
3.1. Clinicopathologic Effects
Administration of EGCG, GTE, and catechins was associated with a significant decrease in body weight in 9 of 15 studies [38][40][41][42][46][48][55][56][57] and a significant decrease in body mass index (BMI) in 7 of these 9 studies [40][41][42][48][55][56][57] (Table 2). Maki et al. examined the effects of green tea catechins on the body composition with obese adults and noted direct effects, similar to the findings in rodent studies [48].
Waist circumference (WC) was frequently evaluated as a surrogate for changes in body weight and fat loss. Five studies reported decreases in WC with catechins, EGCG, and GTE, concurrent with decreases in body weight [40,42,43,56,57]. Moreover, it is important to consider other possible mechanisms that may explain the decreases in body weight. For example, Chantre et al. found that GTE supplementation can inhibit gastric and pancreatic lipases, stimulate thermogenesis, increase energy expenditure (EE), and lower body weight; these changes can have substantial health benefits in obese patients [40]. In general, most studies did not find a change in energy intake or expenditure following treatment with EGCG/GTE (
). Maki et al. examined the effects of green tea catechins on the body composition with obese adults and noted direct effects, similar to the findings in rodent studies [46].
Waist circumference (WC) was frequently evaluated as a surrogate for changes in body weight and fat loss. Five studies reported decreases in WC with catechins, EGCG, and GTE, concurrent with decreases in body weight [38][40][41][54][55]. Moreover, it is important to consider other possible mechanisms that may explain the decreases in body weight. For example, Chantre et al. found that GTE supplementation can inhibit gastric and pancreatic lipases, stimulate thermogenesis, increase energy expenditure (EE), and lower body weight; these changes can have substantial health benefits in obese patients [38]. In general, most studies did not find a change in energy intake or expenditure following treatment with EGCG/GTE (
Table 2).
3.2. Lipid Metabolism
Similar to the rodent studies, the human studies focused on LDL, TG, TC, and high-density lipoprotein (HDL) to evaluate the lipid metabolism effects of GTE (
).
3.2. Lipid Metabolism
Similar to the rodent studies, the human studies focused on LDL, TG, TC, and high-density lipoprotein (HDL) to evaluate the lipid metabolism effects of GTE (Table 2). Significant decreases in LDL were reported in 10 of 12 studies [42,43,46,50,52,54,55,56,57,59], and significant decreases in TC were reported in 6 of 12 studies [50,52,54,55,56,59]. For HDL, 4 of 12 studies reported a significant increase [46,50,55,59], but 7 of 12 studies reported no change [42,43,48,49,50,52,54,55,56]. Brown et al. reported no changes in LDL, HDL, TG, or TC in obese males who received 800 mg/day of oral EGCG [49]. When considering the results of other studies, these authors attributed the lack of improvement to the relatively low dosage of EGCG. They also noted that the peak EGCG plasma concentration was approximately 1 μM, suggesting low oral bioavailability. In general, adequate EGCG/GTE dosages appear to exert salubrious effects on lipid profiles, in resonance with findings from murine studies.
3.3. Carbohydrate Metabolism
Human studies focused on investigating changes in glucose, insulin, and IR to evaluate the effectiveness of GTE in obese patients (
). Significant decreases in LDL were reported in 10 of 12 studies [40][41][44][48][50][52][53][54][55][57], and significant decreases in TC were reported in 6 of 12 studies [48][50][52][53][54][57]. For HDL, 4 of 12 studies reported a significant increase [44][48][53][57], but 7 of 12 studies reported no change [40][41][46][47][48][50][52][53][54]. Brown et al. reported no changes in LDL, HDL, TG, or TC in obese males who received 800 mg/day of oral EGCG [47]. When considering the results of other studies, these authors attributed the lack of improvement to the relatively low dosage of EGCG. They also noted that the peak EGCG plasma concentration was approximately 1 μM, suggesting low oral bioavailability. In general, adequate EGCG/GTE dosages appear to exert salubrious effects on lipid profiles, in resonance with findings from murine studies.
3.3. Carbohydrate Metabolism
Human studies focused on investigating changes in glucose, insulin, and IR to evaluate the effectiveness of GTE in obese patients (Table 2). There were no significant changes in glucose levels in 8 of 12 studies [41,43,45,48,51,52,53,54], insulin levels in 7 of 11 studies [41,45,46,48,49,53,54], and IR in 3 of 6 studies [46,49,52]. Thus, these parameters were not significantly altered by tea catechins in most human studies, although they were significantly reduced in the rodent studies. Of note, the study duration may be important when considering alterations in metabolic syndrome markers. In reviewing the studies in
). There were no significant changes in glucose levels in 8 of 12 studies [39][41][43][46][49][50][51][52], insulin levels in 7 of 11 studies [39][43][44][46][47][51][52], and IR in 3 of 6 studies [44][47][50]. Thus, these parameters were not significantly altered by tea catechins in most human studies, although they were significantly reduced in the rodent studies. Of note, the study duration may be important when considering alterations in metabolic syndrome markers. In reviewing the studies in
Table 2, it appears that short-term studies reported no change in glucose and insulin, where treatment was administered for less than 6 weeks [53,54]. On the other hand, longer study durations were associated with changes in glucose, insulin, and IR [47,50,55,57]. Taken together, treatment with GTE should preferably be continued for at least 12 weeks, to observe effects on carbohydrate metabolites.
3.4. Inflammatory Markers
As can be seen from
, it appears that short-term studies reported no change in glucose and insulin, where treatment was administered for less than 6 weeks [51][52]. On the other hand, longer study durations were associated with changes in glucose, insulin, and IR [45][48][53][55]. Taken together, treatment with GTE should preferably be continued for at least 12 weeks, to observe effects on carbohydrate metabolites.
3.4. Inflammatory Markers
As can be seen fromTable 2, only five studies assayed inflammatory markers, with no conclusive trends [47,48,51,55,59]. Others reported that catechins have anti-inflammatory properties that suppress leukocyte adhesion to endothelium and inhibit transcription factors for cytokines and adhesion molecules, in other disease contexts. In contrast to rodent studies, few studies have examined the effects of EGCG on inflammatory markers in NAFLD, highlighting the need for more research examining inflammatory profiles in patients with NAFLD.
3.5. Oxidative Stress Markers
An insufficient number of studies evaluated the effects of EGCG or GTE on oxidative stress markers. MDA and total antioxidant status (TAS) were the only oxidative stress markers assayed. MDA is the most frequently used biomarker of oxidative stress in various diseases [61]. TAS has an inverse relationship with other oxidative stress markers, such as MDA, as it represents antioxidative capacity [62]. Two of three studies reported significant decreases in MDA [42,52], and both studies investigating the effects of GTE on TAS reported significant increases [55,56]. Basu et al. reported a significant decrease in MDA, confirming the antioxidant properties of GTE, and Bogandaski et al. reported a significant increase in TAS after 3-month supplementation with GTE, indicating that GTE improved oxidative stress [52,55].
The antioxidative properties of green tea catechins are best appreciated by understanding the structural properties of EGCG. These properties have been attributed to the presence of dihydroxyl or trihydroxyl groups on the B-ring and meta-5,7-dihydroxyl groups on the A-ring. The polyphenolic structure of green tea catechins allows delocalization of electrons, which promotes the elimination of reactive oxygen and nitric radicals [56].
Although limited studies have examined the effects of EGCG or GTE in humans, the available data suggest that EGCG or GTE supplementation is a promising strategy for alleviating oxidative stress. The results of human studies are consistent with those of rodent studies, which clearly demonstrates the antioxidant effects of EGCG. Nevertheless, more research is necessary to confirm the efficacy of these supplements in reducing oxidative stress in humans.
3.6. Liver Enzymes
Similar to rodent studies, serum AST and ALT were common metrics used for assessing liver damage in human studies, and both markers were decreased with EGCG and GTE treatment (
, only five studies assayed inflammatory markers, with no conclusive trends [45][46][49][53][57]. Others reported that catechins have anti-inflammatory properties that suppress leukocyte adhesion to endothelium and inhibit transcription factors for cytokines and adhesion molecules, in other disease contexts. In contrast to rodent studies, few studies have examined the effects of EGCG on inflammatory markers in NAFLD, highlighting the need for more research examining inflammatory profiles in patients with NAFLD.
3.5. Oxidative Stress Markers
An insufficient number of studies evaluated the effects of EGCG or GTE on oxidative stress markers. MDA and total antioxidant status (TAS) were the only oxidative stress markers assayed. MDA is the most frequently used biomarker of oxidative stress in various diseases [59]. TAS has an inverse relationship with other oxidative stress markers, such as MDA, as it represents antioxidative capacity [60]. Two of three studies reported significant decreases in MDA [40][50], and both studies investigating the effects of GTE on TAS reported significant increases [53][54]. Basu et al. reported a significant decrease in MDA, confirming the antioxidant properties of GTE, and Bogandaski et al. reported a significant increase in TAS after 3-month supplementation with GTE, indicating that GTE improved oxidative stress [50][53]. The antioxidative properties of green tea catechins are best appreciated by understanding the structural properties of EGCG. These properties have been attributed to the presence of dihydroxyl or trihydroxyl groups on the B-ring and meta-5,7-dihydroxyl groups on the A-ring. The polyphenolic structure of green tea catechins allows delocalization of electrons, which promotes the elimination of reactive oxygen and nitric radicals [54]. Although limited studies have examined the effects of EGCG or GTE in humans, the available data suggest that EGCG or GTE supplementation is a promising strategy for alleviating oxidative stress. The results of human studies are consistent with those of rodent studies, which clearly demonstrates the antioxidant effects of EGCG. Nevertheless, more research is necessary to confirm the efficacy of these supplements in reducing oxidative stress in humans.3.6. Liver Enzymes
Similar to rodent studies, serum AST and ALT were common metrics used for assessing liver damage in human studies, and both markers were decreased with EGCG and GTE treatment (Table 2). Following EGCG or GTE administration, significant decreases in AST were reported in four of six studies [47,57,59], and significant decreases in ALT were reported in three of five studies [47,58,59]. Pezeshki et al. reported significant decreases in AST and ALT following 12-week treatment with 500 mg/day of GTE [58]. This result was confirmed by Hussain et al., who found similar results using the same GTE dosage and treatment duration [59].
). Following EGCG or GTE administration, significant decreases in AST were reported in four of six studies [45][55][57], and significant decreases in ALT were reported in three of five studies [45][56][57]. Pezeshki et al. reported significant decreases in AST and ALT following 12-week treatment with 500 mg/day of GTE [56]. This result was confirmed by Hussain et al., who found similar results using the same GTE dosage and treatment duration [57].