Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Beatrix Zheng and Version 1 by Shuang-Qing Zhang.
Icaritin (ICT) is not only an enzyme-hydrolyzed product of icariin but also an intestinal metabolite of eight major flavonoids of the traditional Chinese medicinal plant Epimedium with extensive pharmacological activities, such as strengthening the kidney and reinforcing the bone. ICT displays several therapeutic effects, including osteoporosis prevention, neuroprotection, antitumor, cardiovascular protection, anti-inflammation, and immune-protective effect. ICT inhibits bone resorption activity of osteoclasts and stimulates osteogenic differentiation and maturation of bone marrow stromal progenitor cells and osteoblasts.
- icaritin
- antiosteoporosis
- pharmacokineticcs
- drug delivery systems
1. Introduction
Osteoporosis, a systemic skeletal disorder, is caused by excessive bone resorption over bone formation, characterized by decreased bone mineral density, microarchitectural deterioration, increased bone fragility and susceptibility to fracture [1,2][1][2]. Worldwide, over 200 million people are estimated to suffer from osteoporosis, in which women over the age of 50 or postmenopausal women are four times more likely to develop the disease than men [3]. Annually, osteoporosis causes more than 8.9 million fractures throughout the world, resulting in annual costs of more than 10 billion dollars [4].
Epimedium (Berberidaceae) is an important traditional Chinese medicinal plant and has long been used alone or in combination with other herbs for the treatment of various diseases, including osteoporosis, tendon health, cardiovascular diseases, sexual dysfunction, and menstrual irregularity [5]. There are more than 260 compounds identified from Epimedium including 141 flavonoids, 31 lignins, 12 ionones, 9 phenol glycosides, 6 phenylethanoid glycosides, 5 sesquiterpenes, and other types of moieties, of which flavonoids are the major components and important chemotaxonomic markers [6]. Icariin is the most abundant constituent and accounts for more than 5.0% of the dried weight of an alcoholic decoction of Epimedium [7]. Icaritin (ICT, Figure 1A) is not only a bioactive compound enzyme-hydrolyzed from icariin but also an intestinal metabolite of eight major flavonoids of Epimedium [8,9][8][9]. It exerts broad therapeutic capabilities such as osteoprotective effect [10], neuroprotective effect [11], cardiovascular protective effect [12], anti-cancer effect [13], anti-inflammation effect [14], and immune-protective effect [15]. Unfortunately, anhydroicaritin (Figure 1B) and wushanicaritin (Figure 1C) were regarded as ICT by mistake in some reports [6,16][6][16] possibly as they had similar chemical structures. On 10 January 2022, ICT was approved for the treatment of advanced hepatocellular carcinoma by China National Medical Products Administration. ICT is currently undergoing phase 1 clinical trial for the treatment of osteoporosis (ClinicalTrials.gov Identifier: NCT02931305). ICT targets osteogenesis pathways in mesenchymal stem cell, osteoblast, and osteoclast cell lineages, and displays beneficial effects on bone health in osteoporosis animal models [17]. Particularly, the prominent osteogenic effects of ICT made it a promising anti-osteoporotic drug candidate since ICT as a natural phytoestrogen may negate the high risks of hormone replacement therapy in clinic [8]. However, unfavorable intrinsic physicochemical and pharmacokinetic properties of ICT restrict its anti-osteoporotic effects, therefore, various novel drug delivery systems have been developed to dissolve the problems. Over the past decades, few literature reviews and book chapters have involved the topic. Therefore, osteogenic effects and mechanisms, pharmacokinetic properties and delivery systems of ICT are reviewed and discussed.
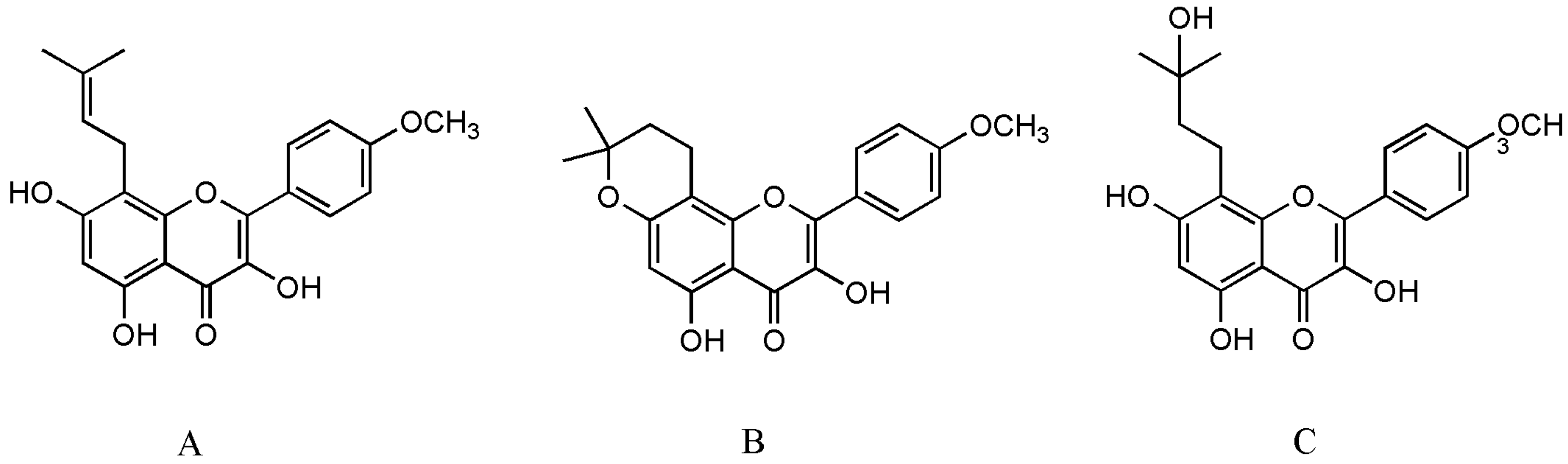
Figure 1.
The structure of ICT (
A
), anhydroicaritin (
B
) and wushanicaritin (
C
).
2. Effects of Icaritin on Osteoporosis
Healthy bone, a dynamic living tissue, is mainly composed of two distinct types of cells: (1) osteoblasts, derived from bone marrow mesenchymal stromal cells (MSCs), which are bone-forming cells, and (2) osteoclasts, derived from bone marrow hematopoietic progenitors, which are multinucleated bone-resorbing cells. If the dynamic balance between bone formation and resorption is destroyed, bone metabolism disorders occur such as osteoporosis and osteopetrosis [18]. There are many factors that promote the occurrence and progression of osteoporosis, but the fundamental mechanism is an imbalance between osteoblasts and osteoclasts, including: (1) decreased differentiation and activity of osteoblasts result in reduced bone deposition, and (2) increased osteoclasts differentiation and activity lead to excessive bone resorption [19]. Therefore, osteoporosis therapy focuses on rebuilding the balance between bone formation and resorption.
2.1. Mesenchymal Stromal Cells
In 1951, Lorenz and his coworkers first verified that bone marrow acted as a pool of hematopoietic stem cells (HSCs) to maintain blood cells homeostasis for lifespan in mice and guinea pigs experiments [20]. Further research found that adult bone marrow-derived multipotent stem cells contained not only HSCs but also non-hematopoietic cells, that is MSCs. Then, MSCs have also been isolated from several other parts of the body including the adipose tissue, umbilical cord blood, skin, and amniotic fluid [21,22][21][22]. A series of studies, both in vivo and in vitro, have shown that MSCs have distinct differentiation potential under special microenvironment [23,24][23][24]. Since 1995, MSCs have been used in clinically studied experimental cell therapy for a wide range of diseases, such as systemic sclerosis [25], neurodegenerative diseases [26], liver regeneration [27[27][28],28], osteoarthritis [29], osteonecrosis [30], angiogenesis [31], ischemic brain [32], etc.
Fundamentally, MSCs are precursors for both osteoblasts and adipocytes, between which an inverse relationship exists (Figure 2). Bone loss is commonly accompanied by increasing bone marrow adiposity, that means MSCs play an important role in the development of osteoporosis. Therefore, promoting MSCs to osteogenesis is beneficial to bone regeneration. Several research have shown some small molecules such as ascorbic acid, β-glycerophosphate, and dexamethasone can stimulate osteoblastogenesis of MSCs by increasing the activity of alkaline phosphatase (ALP), calcium deposition, and suppressing adipogenesis of MSCs [33,34,35][33][34][35]. In 2013, Sheng et al. first reported that the novel semisynthetic molecule ICT could promote osteogenic differentiation and suppress adipogenesis of MSCs [10].
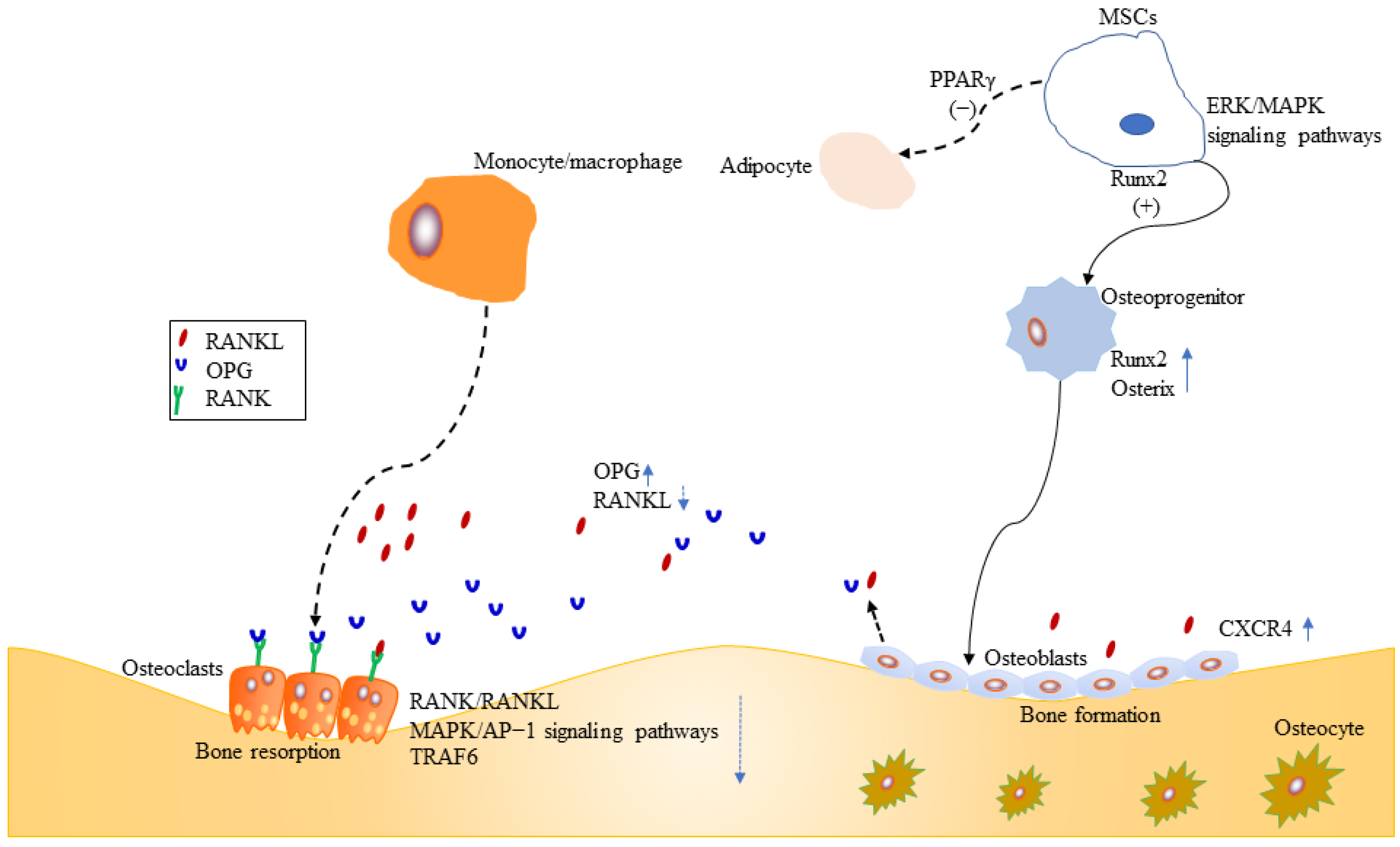
Figure 2.
Effects of ICT on MSCs, osteoblasts and osteoclasts.
Runx2 is a key transcription factor for skeletal mineralization due to its regulation of extracellular matrix genes such as ALP, osteopontin, and type I collagen [36,37][36][37]. PPARγ plays an essential role in regulating development of the adipose lineage [38], and the relative activities of two transcription factors Runx2 and PPARγ determine whether MSCs differentiate into osteoblasts or adipocytes [39] (Figure 2). Sheng et al. [10] further identified that ICT promoted osteogenic differentiation and maturation of MSCs through initiating activation of Runx2. Meanwhile, their investigation [10] showed that ICT inhibited adipogenesis of MSCs through suppressing PPARγ (Figure 2).
Runx2 is activated by estrogen receptor and mitogen-activated protein kinase (ERK/MAPK)-dependent phosphorylation [39,40][39][40]. ERK/MAPK signaling pathways are essential for cellular biochemical and physiological processes including cell proliferation, migration, and differentiation. Luo et al. demonstrated that ICT could activate ERK/MAPK signaling pathway and facilitate the orientation of osteogenic differentiation of bone marrow MSCs in vitro [41] (Figure 2).
Stromal cell-derived factor-1 (SDF-1)/cysteine I-X-C motif chemokine receptor 4 (CXCR4) axis is required for mobilization and recruitment of MSCs, as well as proliferation and survival of MSCs [42,43][42][43] (Figure 2). Using an in vitro cell culture model, Lim et al. demonstrated that ICT enhanced MSCs proliferation, chemotaxis to SDF-1, and osteogenic differentiation, through the activation of signal transduction activator transcription factor (STAT-3) [44].
2.2. Osteoblasts
Osteoblasts, originating from MSCs, mediate bone-formation of new bone tissue, which is coupled by osteoclast-mediated bone resorption of old bone tissue. Therefore, stimulation of osteoblasts proliferation and activation is a target for new bone-forming to prevent osteoporosis. Osteoprogenitors, osteoblasts, and osteocytes belong to osteoblast lineage cells. The mature osteoblasts, located on the bone surfaces, are responsible for the synthesis and mineralization of the organic matrix rich in type I collagen and osteocalcin in the initial bone formation phase [45,46][45][46]. Early osteoprogenitors express Runx2 and osterix which are two critical transcription factors for osteoblasts differentiation and function [45,47,48,49,50][45][47][48][49][50] (Figure 2). CXCR4 is critical for maintaining osteoblast anabolic function. ICT enhanced the differentiation of MC3T3-E1 preosteoblastic cells and subsequently resulted in mineralization, collagen synthesis, and bone formation, because ICT promoted mRNA and protein expression of bone-forming biomarkers, such as ALP, type I collagen, osteocalcin, OPN, and Runx2 [51]. Further study revealed the mechanisms might be associated with ERK/MAP signaling pathway activated by ICT [51]. Wei et al. found that ICT could promote maturation and mineralization of MC3T3-E1 cells through SDF-1/CXCR4 signaling pathway in a series of in vitro experiments [52]. Lim et al. examined whether ICT could increase human osteoblast anabolic function. Both cellular and animal experiments showed that ICT increased osteoblasts proliferation and function. The underlying mechanism was that ICT suppressed the phosphorylation of STAT-3 to upregulate CXCR4 expression [53]. Peng et al. performed a study to examine the relationship between ICT treatment initiation time and bone turnover markers in adult ovariectomized rats, and found that early ICT treatment (1 month post-operation), not late ICT treatment (3 months post-operation), exerted beneficial effects on osteoporotic bone in ovariectomized rats [54]. Meanwhile, they performed a series of experiments to evaluate the population of osteoblasts with colony formation assays, assess the expression levels of osteoblasts-related genes by real-time polymerase chain reaction. Late ICT treatment failed to increase bone-forming related parameters [54].
Osteoblasts play an important role in maintaining bone homeostasis. Mature osteoblasts produce type I collagen and osteocalcin, and regulate activity of osteoclasts through receptor activator of nuclear factor-κB ligand (RANKL) and osteoprotegerin (OPG) [45] (Figure 2). Currently, OPG/RANKL/RANK signaling pathway is a crucial signal pathway for bone remodeling for the interaction between osteoblasts and osteoclasts, as well as a major pathway for affecting bone metabolism and for preventing and treating osteoporosis [55,56,57][55][56][57]. The trimolecular complex belongs to the superfamily of tumor necrosis factor (TNF) [58]. The receptor activator of NF-κB (RANK) is located on the osteoclasts surface, and its major ligands are OPG and RANKL. OPG, a secreted glycoprotein, has been identified to regulate bone resorption [57,59][57][59]. RANKL is mainly derived from osteocytes, osteoblasts, and MSCs during bone remodeling [58], and RANK is the only known receptor for RANKL. OPG and RANKL compete for RANK, which determines the balance between bone remodeling and resorption [60]. Huang et al. demonstrated that Epimedium-derived prenylflavonoids including icariin, icariside II, and ICT could promote proliferation, alkaline phosphatase activity, osteocalcin secretion of osteoblasts, and matrix mineralization [61]. Furthermore, the experiment demonstrated that ICT was more potent than other extracts, because ICT increased mRNA expression of OPG, and inhibited mRNA expression of RANKL [61].
2.3. Osteoclasts
Osteoclasts, arose from bone marrow hematopoietic monocyte/macrophage progenitors, mediate bone resorption of old bone tissue. The regulation of osteoclasts differentiation and activation involve signaling induced by RANKL and its receptor RANK [62,63,64,65,66,67][62][63][64][65][66][67] (Figure 2). Once RANK is activated by RANKL, osteoclasts differentiate and promote bone resorption. However, excessive activation of RANK/RANKL signaling pathway leads to osteoporosis. Therefore, inhibition of the RANKL-induced osteoclasts formation is an effective therapy for osteoporosis. TNF receptor-associated factor6 (TRAF6), a critical adaptor protein, is necessary for bone resorption [68], which is supported by several studies that TRAF6-deficient mice generated osteopetrosis [69,70,71][69][70][71]. Liu et al. evaluated the growth inhibitory effect of ICT on preosteoclastic RAW264.7 cells, and found ICT suppressed osteoclastic differentiation and activity in a dose-dependent manner [72]. Furthermore, Tan et al. revealed that ICT suppressed osteoclastogenesis in two osteoclast precursor models, RAW 264.7 mouse monocyte cell line and human PBMC, through inhibition of RANK/RANKL and MAPK/AP-1 signaling pathways and promotion of proteasomal degradation of TRAF6 [73]. A randomized, double-blind, placebo-controlled trial showed that ICT increased the bone anabolism marker such as bone specific alkaline phosphatase and suppressed TRAF6 protein in peripheral blood osteoclast-precursor monocytes in post-menopausal women [74].
2.4. Inflammation and Osteoporosis
Recently, more attention has been paid on the relationship between inflammation and osteoporosis. Evidence has shown that inflammatory cytokines play an important role in the osteoporosis processing of hormonal deficiency-induced rat model [75,76][75][76]. Accumulating data suggested that pro-inflammatory cytokines such as interleukins (IL), tumor necrosis factor-alpha (TNF-α), chemokines, interferons could induce osteoclastic bone resorption [77,78][77][78]. In 2013, Lai et al. first demonstrated the anti-inflammatory effect of ICT in lipopolysaccharide (LPS)-induced mouse peritoneal macrophages in vitro and peritonitis model in vivo [14]. In this report, the researchers found pretreatment of ICT significantly could inhibit the inflammatory cytokines production, including IL-6, IL-10, MCP-1, IFN, TNF, and IL-12p70 [14]. Then anti-inflammatory activity of icariin and its metabolites have been widely reported in different areas of disease [79,80,81][79][80][81].
2.5. Animal Bone Defect Model
Based on the findings that ICT might be a therapeutic small molecule agent for bone reconstruction, a series of animal bone defect model experiments systematically evaluated bone regeneration of bioactive scaffolds incorporating phytomolecule ICT which served as exogenous growth factor [82,83,84][82][83][84]. Not only in the non-loading bearing mechanical stresses rat calvarial defects model, but also in a standard rabbit ulnar segmental defect model, the bioactive scaffold incorporating ICT enhanced newly mineralized bone and new vessel growth. In conclusion, as an exogenous growth factor, ICT is beneficial to bone regeneration.