Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Conner Chen and Version 1 by Cortney Steele.
Obesity indirectly causes strain on the kidneys by increasing blood pressure, intensifying renal tubular sodium reabsorption, and weakening pressure natriuresis. These events lead to volume expansion by stimulation of the sympathetic nervous system and the renin-angiotensin-aldosterone system (RAAS). Physical compression of the kidneys from surplus visceral adipose tissue also impacts kidney health and function. Obesity also can lead to renal vasodilation and glomerular hyperfiltration that initially serve as compensatory mechanisms to maintain a sodium balance in the face of increased tubular reabsorption. These potential mechanisms may make obesity a risk for the development and progression of chronic kidney disease (CKD).
- adipose tissue
- chronic kidney disease
- weight loss
1. Introduction
The definition of obesity simplified is excessive body weight relative to height; however, the phenotype draws complex alterations metabolically and has detrimental effects on an individual’s overall health [1]. The World Health Organization (WHO), International Obesity Task Force (IOTF), among other reputable organizations, recognize that for those ≥20 years of age, a body mass index (BMI) ranging from 18.50 to 24.99 kg/m2 is normal, ≥25.00 to 29.99 kg/m2 is overweight, and ≥30.00 kg/m2 is obese [2].
The prevalence of obesity continues to rise and is a major public health concern in industrialized countries globally [3][4][5]. Individuals with obesity are at risk for developing comorbid conditions including cardiovascular disease (CVD), hypertension, gastrointestinal disorders, chronic kidney disease (CKD), type 2 diabetes (T2D), as well as other diseases that may indirectly increase mortality risk [6][7].
Obesity indirectly causes strain on the kidneys by increasing blood pressure, intensifying renal tubular sodium reabsorption, and weakening pressure natriuresis [8][9][10]. These events lead to volume expansion by stimulation of the sympathetic nervous system and the renin-angiotensin-aldosterone system (RAAS) [11][12][13][14]. Physical compression of the kidneys from surplus visceral adipose tissue also impacts kidney health and function [11][15][16]. Obesity also can lead to renal vasodilation and glomerular hyperfiltration that initially serve as compensatory mechanisms to maintain a sodium balance in the face of increased tubular reabsorption [17]. These potential mechanisms may make obesity a risk for the development and progression of chronic kidney disease (CKD) [11][17][18][19][20].
Similar to the general population, evidence suggests obesity is on the rise in those with CKD [21]. The average BMI from 1995 to 2002 has increased from 25.7 to 27.5 kg/m2 in patients with end-stage kidney disease (ESKD) [22]. The incidence of total obesity and obesity stage 2 (BMI and >35 kg/m2) increased by 33 and 63%, respectively, in this ESKD cohort [22]. In a large cohort study consisting of 3334 CKD patients from Queensland, Australia in 2011, 18.9% had a normal BMI (18.5–24.9 kg/m2), 29.9% were overweight (BMI 25–29.9 kg/m2), 25.1% were mildly obese (BMI 30–34.9 kg/m2), and 26.1% were moderately obese+ (BMI ≥ 35 kg/m2). Thus, in this cohort, 81.1% of the CKD patients were either overweight or obese [23].
Polycystic kidney disease (PKD), a form of CKD, is the most common genetic cause of kidney failure affecting >10 million people worldwide [24]. The genetic disorder is characterized by progressive development and enlargement of multiple renal cysts that ultimately lead to loss of kidney function in the majority of afflicted patients [25]. Autosomal dominant PKD (ADPKD) is the most common form of PKD and is primarily caused by mutations in the PKD1 and PKD2 genes, encoding the polycystin 1 and polycystin 2 proteins (Figure 1) [24]. Decreases in kidney function typically do not occur until adulthood in those with ADPKD [24]. The prevalence of overweight and obesity has also increased in the ADPKD community.
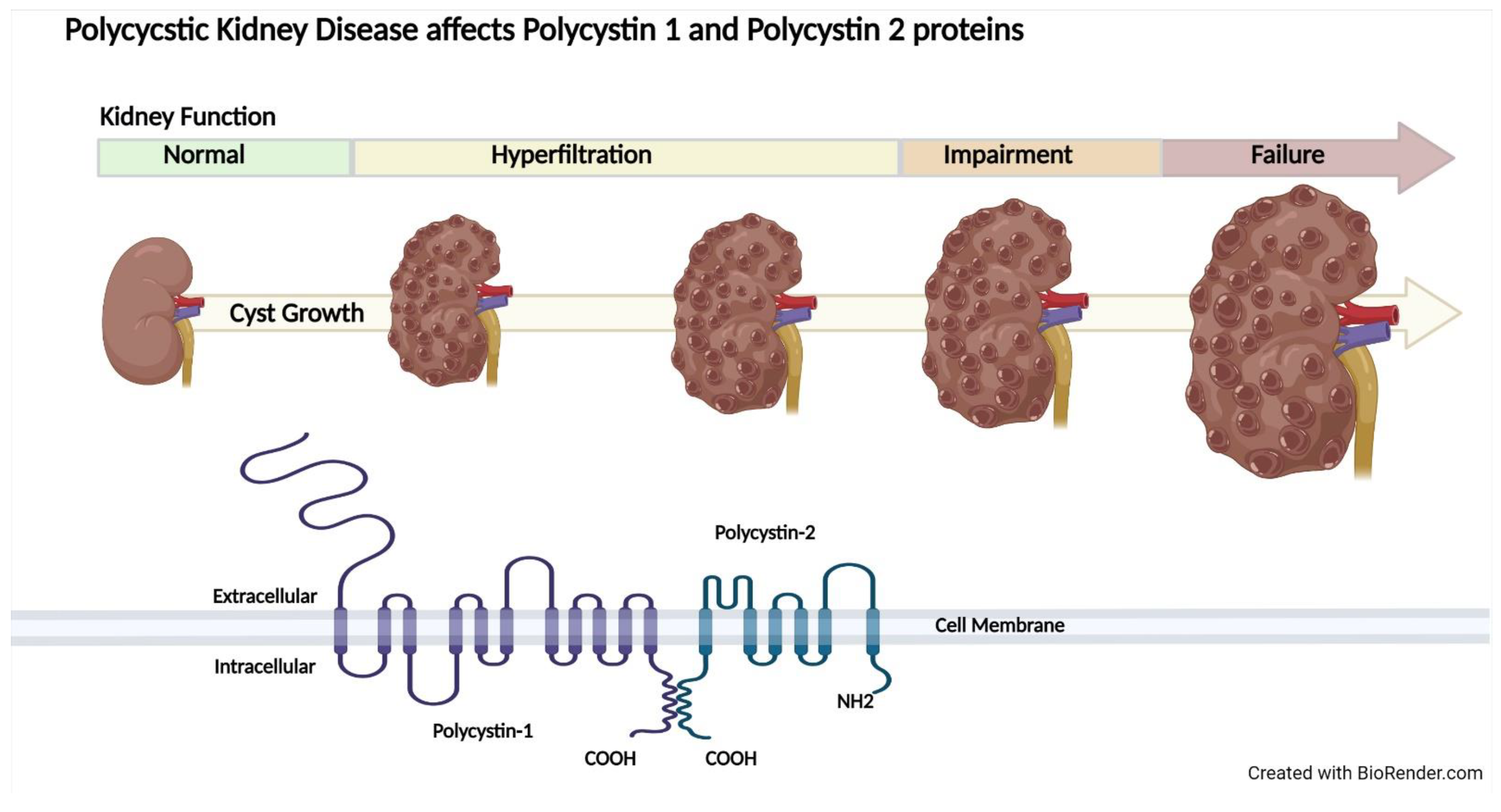
Figure 1. Autosomal polycystic kidney disease (ADPKD) progression and genetic mutations. ADPKD increases total kidney volume from the initiation and proliferation of kidney cysts, causing reductions in kidney function leading to end-stage kidney disease. Polycystin 1 and Polycystin 2 proteins are affected in ADPKD.
In the HALT Progression of Polycystic Kidney Disease Study A (HALT-PKD Study A), which included individuals in the United States averaging 37 years of age with early-stage ADPKD, 62.7% of participants were overweight or obese [26][27]. The average BMI in this trial was 27.1 kg/m2 [26][27]. The prevalence of overweight and obesity continue to rise, impacting many populations, including those with CKD and ADPKD.
2. Epidemiological Data on BMI and Kidney Disease
2.1. General Population
Obesity increases the risk for kidney disease in the general population [28]. Obesity classified by BMI, increased waist circumference, and increased visceral adipose tissue are associated with elevated albuminuria in the general population [29][30][31][32]. After adjusting for potential confounders, higher BMI is associated with increased risk of CKD [18][33][34], reduced estimated glomerular filtration rate (eGFR) [35], decline in kidney function (eGFR slope) [36], and incidence of ESKD [19][20][37] in the general population. A higher BMI at the baseline and increases in BMI over 14 years are associated with a greater risk of CKD [33]. Larger waist circumference is also associated with ESKD, even after adjustment for BMI [22]. Pinto-Sietsma et al. found lean, overweight, and obese subjects with central fat distribution were all at risk for diminished filtration [29]. Central fat distribution has been defined as a waist-hip ratio of ≥0.9 for men and ≥0.8 for women [29][38]. Collectively, this evidence supports that fat distribution may elevate the risk for kidney disease even more than BMI.
2.2. Chronic Kidney Disease
A greater prevalence of overweight and obesity has been observed in males aged 45–64 years with CKD stages 3b and 4 (≤44 mL/min/1.73 m2) when compared to females and to CKD stages 1–3a (≥45 mL/min/1.73 m2) [39]. Higher BMI is associated with increased risk for incident of CKD and advanced CKD (Stage 4–5; eGFR ≤ 29 mL/min/1.73 m2) [18][33][34][40]. A male-sex-specific association between increased BMI and CKD has been noted in several studies [19][39][41][42]. Notably, BMI may reflect visceral fat more effectively in males when compared to females [43][44]. In addition, the occurrence of CKD progression, as measured by the rate of eGFR decline per year (>1 mL/min/1.73 m2/year), was greater in those with overweight and obese when compared to normal-weight CKD patients [45].
However, there have been several studies that have found no association between BMI and progression of disease in individuals with CKD [23][46][47][48][49]. Commonly referred to as the “obesity paradox”, epidemiological studies have demonstrated a lower relative risk of death in patients who are overweight or obese with ESKD, stroke, and heart failure, among other conditions [50][51][52][53][54][55][56]. Specifically, dialysis patients who are overweight or obese have a decreased mortality risk [53]. Lu et al. identified a U-shaped association between BMI and risk of kidney disease progression in a large cohort of United States Veterans, demonstrating that those with overweight and mild obesity (BMI 25–35 kg/m2) had more favorable clinical outcomes [36]. This phenomenon might be explained by the inherent complexity of chronic diseases, unmeasured risk factors, or bias related to participant selection. There are constraints to using BMI in that it does not account for muscle mass, peripheral and abdominal adipose tissue mass, and bone; consequently, the results should be considered under these limitations [36]. However, globally BMI is the primary measurement to evaluate and define obesity [2]. Molnar et al. found hemodialysis patients with lower BMI or muscle mass and/or unintentional weight or muscle loss had higher mortality [54]. Interestingly, the waist to hip ratio and waist circumference, but not BMI, was associated with mortality in a cohort of patients with CKD and ESKD [43][44]. Additionally, those with CKD who were in the normal BMI category with central obesity had an increased risk of coronary artery calcification [57]. Collectively, these observations again underscore that central obesity might be key in disease development and progression.
2.3. Autosomal Dominant Polycystic Kidney Disease
Distinct from other etiologies of CKD, total kidney volume (TKV), often adjusted by height, has been identified as the best biomarker for ADPKD progression, particularly in early-stage disease [58][59]. In addition, Mayo imaging classification helps predict loss of kidney function based on TKV, age, height, and sex [59]. HALT-PKD Study A was a randomized, double-blind, placebo-controlled study in non-diabetic patients with early-stage ADPKD [26]. In HALT-PKD study A, baseline BMI was significantly associated with baseline height-adjusted total kidney volume (htTKV) in men only [60]. Body-surface area was also an independent predictor of baseline htTKV and baseline eGFR in the HALT Studies [60].
In a fully adjusted model accounting for age, sex, race/ethnicity, group randomization, systolic blood pressure, eGFR, urinary albumin excretion, baseline TKV, baseline liver volume, serum class, and mutation class, a higher BMI was associated with a greater annual percent change in TKV in patients with early-stage ADPKD participating in HALT study A [61]. Obesity was also associated with a faster decline in eGFR [61]. These results were subsequently confirmed in individuals with early-stage ADPKD participating in the Tolvaptan Efficacy and Safety in the Management of Autosomal Dominant Polycystic Kidney Disease and Its Outcomes (TEMPO 3–4) trial. After adjustment for age, sex, race/ethnicity, group randomization, systolic blood pressure, serum glucose, baseline eGFR, urinary microalbumin, plasma copeptin, and mutation class, a higher BMI was again associated with a greater annual change in TKV [27]. Notably, the efficacy of tolvaptan was independent of BMI [27]. Of importance, in those with ADPKD, enlarged kidneys may contribute considerably to overall body weight, which may impact BMI calculations, expanding the limitations of BMI discussed previously [62]. However, in the analyses from HALT study A and TEMPO 3:4, BMI was calculated after subtracting the contribution of the kidneys to total body weight, thus controlling for this factor.
The epidemiological data present a strong case overall that overweight and obesity, as measured by BMI, may increase the risk of incident kidney disease and progression, although these studies are observational and there are inherent limitations. Specifically, the ADPKD studies present strong evidence that overweight and obesity are risk factors for disease progression measured by TKV. The mixed evidence in the CKD population, particularly involving the association of BMI with eGFR, may be due to the inability to account for body composition, fat distribution, and other unmeasured risk factors in the CKD population. This underscores the importance that central body fatness is a stronger predictor of overall disease risk when compared to overall body size [63][64].
3. Potential Role of Adipose Tissue
Adipose tissue is important in helping to maintain lipid and glucose homeostasis [65]. However, obesity and increased accumulation of adipose tissue result in a pro-inflammatory, hyperlipidemic, and insulin-resistant environment. This dysfunctional adipose tissue can contribute to type 2 diabetes and promote cardiovascular disease [66]. Excessive adipose tissue has the potential to be even more harmful to individuals with ADPKD because of the known metabolic alterations linked to the genetic disease [67].
3.1. Types and Distribution of Adipose Tissue
Obesity increases total adipose tissue. When in excess, adipose tissue becomes displaced, producing fat deposits not only surrounding the kidneys but also other vital organs. Visceral adipose tissue is hormonally active and has distinct biochemical attributes that impact various normal and pathological processes in the human body [68]. In humans, the only measurements that can produce direct measures of cross-sectional areas or volumetric measures of visceral adipose tissue are through a computerized tomography (CT) scan or magnetic resonance imaging [68]. Visceral adipose tissue is metabolically active and stimulates the release of fatty acids into circulation. Accumulation of visceral fat or visceral obesity leads to a cascade of negative events that promote metabolic syndrome including hyperinsulinemia, systematic inflammation, and dyslipidemia [69]. Both increases in visceral and subcutaneous adipose tissue were associated with a decrease in eGFR (cystatin-based equation) in the individuals from the Framingham Offspring Study (general population) who underwent abdominal CT scans [70]. The location of the adipose tissue, as well as the type of adipose tissue, determines the impact it will have on biochemical processes.
Adipose tissue can be classified into three subsets: white, brown, and beige adipose tissue. About eighty percent of adipose tissue found in lean healthy subjects is subcutaneous white adipose tissue (WAT) [71]. In humans, brown fat found near the regions of the spine accounts for about 2% of total fat [72]. Beige adipose tissue comprises both white and brown adipose tissue. Genetics may also influence WAT distribution [72]. Recently, Fas Binding Factor 1 (FBF1) deficiency has been shown to stimulate beiging and beneficial growth of WAT [73]. Interestingly, FBF1 controlled the beiging program via a cilia-specific, A-kinase anchoring protein (AKAP9)-dependent, protein kinase A (PKA) signaling, supporting a central role for primary cilia in the fate determination of preadipocytes and the generation of metabolically healthy adipose tissue [73].
In those without obesity, WAT is a vital energy source in that it acts as a lipid storage reserve. However, obesity causes WAT to become metabolically dysfunctional [74]. Perinephric adipose tissue (PAT) is a type of WAT that encircles the kidney and supports kidney function [75]. In the Framingham Heart Study, individuals with higher PAT had a higher risk of hypertension, even with adjustment for BMI and visceral fat [76]. During tumorigenesis of clear cell renal cell carcinoma (ccRCC), cells preferentially invade PAT, a process associated with poor prognosis. The cells secrete a parathyroid-hormone-related protein (PTHrP), which promotes the browning of PAT by PKA activation, and the excess release of lactate mediated by thermogenesis, enhancing ccRCC growth. Inhibiting the ccRCC-adipocyte feedback prevents cell growth, invasion, and metastasis [77]. This evidence could potentially be applied to an ADPKD model to suppress the proliferation of kidney cysts.
3.2. Harmful Effects of Adipose Tissue
Adipose tissue releases adipokines, growth factors, pro-inflammatory cytokines, and chemotactic cytokines [78]. Adipokines secrete hormones such as leptin [79], omentin [80], adiponectin [81], resistin [82][83], and fibroblast growth factor 21 [84], which are influenced by weight gain and increased adipose tissue accumulation (Figure 2).
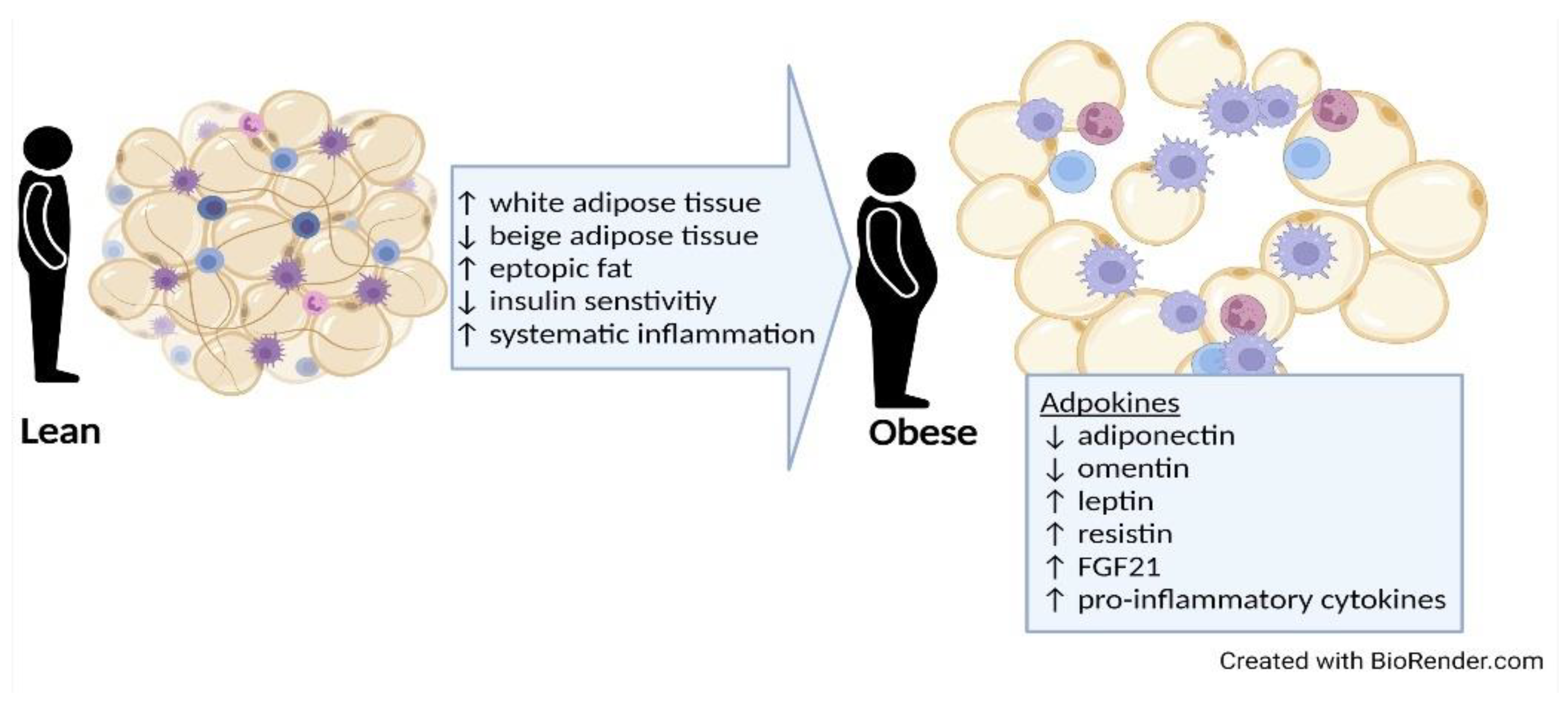
Figure 2. Harmful effects of increased adipose tissue with weight gain. With weight gain there is an increase in total adipose tissue (white and brown adipose tissue); excessive accumulation of adipose tissue causes insulin sensitivity and systematic inflammation. The increase in adipokines leads to altered hormone secretion and pro-inflammatory cytokine production. Abbreviation: FGF21, fibroblast growth factor 2.
Evidence suggests that the elevations in pro-inflammatory cytokines observed in obesity, including interleukin 6 (IL-6), tumor necrosis factor-alpha (TNF-α), monocyte chemoattractant protein-1 (MCP-1), and serum amyloid, can be reduced via weight loss [85][86][87][88]. Epicardial adipose tissue thickness measured via echocardiography was independently associated with highly sensitive C-reactive protein (hs-CRP) concentrations in normotensive ADPKD patients with preserved renal function [89]. In general, reductions in adipose tissue in individuals with ADPKD who are overweight and obese could potentially induce a shift in cytokines and hormones, reducing the effects of ADPKD-associated metabolic dysfunction.
References
- Fruh, S.M. Obesity: Risk factors, complications, and strategies for sustainable long-term weight management. J. Am. Assoc. Nurse Pract. 2017, 29, S3–S14.
- Hruby, A.; Hu, F.B. The Epidemiology of Obesity: A Big Picture. Pharmacoeconomics 2015, 33, 673–689.
- Stevens, G.A.; Singh, G.M.; Lu, Y.; Danaei, G.; Lin, J.K.; Finucane, M.M.; Bahalim, A.N.; McIntire, R.K.; Gutierrez, H.R.; Cowan, M.; et al. National, regional, and global trends in adult overweight and obesity prevalences. Popul. Health Metr. 2012, 10, 22.
- Baskin, M.L.; Ard, J.; Franklin, F.; Allison, D.B. Prevalence of obesity in the United States. Obes. Rev. 2005, 6, 5–7.
- Flegal, K.M.; Carroll, M.D.; Ogden, C.L.; Curtin, L.R. Prevalence and Trends in Obesity Among US Adults, 1999–2008. J. Am. Med. Assoc. 2010, 303, 235–241.
- Valderas, J.M.; Starfield, B.; Sibbald, B.; Salisbury, C.; Roland, M. Defining comorbidity: Implications for understanding health and health services. Ann. Fam. Med. 2009, 7, 357–363.
- Chalmers, L.; Kaskel, F.J.; Bamgbola, O. The Role of Obesity and Its Bioclinical Correlates in the Progression of Chronic Kidney Disease. Adv. Chronic Kidney Dis. 2006, 13, 352–364.
- Hall, J.E.; Brands, M.W.; Dixon, W.N.; Smith, M.J., Jr. Obesity-induced hypertension. Renal function and systemic hemodynamics. Hypertension 1993, 22, 292–299.
- Hall, J.E.; Crook, E.D.; Jones, D.W.; Wofford, M.R.; Dubbert, P.M. Mechanisms of obesity-associated cardiovascular and renal disease. Am. J. Med. Sci. 2002, 324, 127–137.
- Vaes, B.; Beke, E.; Truyers, C.; Elli, S.; Buntinx, F.; Verbakel, J.Y.; Goderis, G.; Van Pottelbergh, G. The correlation between blood pressure and kidney function decline in older people: A registry-based cohort study. British Med. J. Open. 2015, 5, e007571.
- Hall, M.E.; do Carmo, J.M.; da Silva, A.A.; Juncos, L.A.; Wang, Z.; Hall, J.E. Obesity, hypertension, and chronic kidney disease. Int. J. Nephrol. Renov. Dis. 2014, 7, 75–88.
- Alvarez, G.E.; Beske, S.D.; Ballard, T.P.; Davy, K.P. Sympathetic Neural Activation in Visceral Obesity. Circ. 2002, 106, 2533–2536.
- Esler, M.; Rumantir, M.; Wiesner, G.; Kaye, D.; Hastings, J.; Lambert, G. Sympathetic nervous system and insulin resistance: From obesity to diabetes. Am. J. Hypertens. 2001, 14, 304S–309S.
- Abate, N.I.; Mansour, Y.H.; Tuncel, M.; Arbique, D.; Chavoshan, B.; Kizilbash, A.; Howell-Stampley, T.; Vongpatanasin, W.; Victor, R.G. Overweight and sympathetic overactivity in black Americans. Hypertens. 2001, 38, 379–383.
- Bloomfield, G.L.; Sugerman, H.J.; Blocher, C.R.; Gehr, T.W.; Sica, D.A. Chronically increased intra-abdominal pressure produces systemic hypertension in dogs. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 819–824.
- Dwyer, T.M.; Banks, S.A.; Alonso-Galicia, M.; Cockrell, K.; Carroll, J.F.; Bigler, S.A.; Hall, J.E. Distribution of renal medullary hyaluronan in lean and obese rabbits. Kidney Int. 2000, 58, 721–729.
- Hall, J.E.; Henegar, J.R.; Dwyer, T.M.; Liu, J.; da Silva, A.A.; Kuo, J.J.; Tallam, L. Is obesity a major cause of chronic kidney disease? Adv. Ren. Replace. Ther. 2004, 11, 41–54.
- Fox, C.S.; Larson, M.G.; Leip, E.P.; Culleton, B.; Wilson, P.W.; Levy, D. Predictors of new-onset kidney disease in a community-based population. J. Amer. Med. Assoc. 2004, 291, 844–850.
- Iseki, K.; Ikemiya, Y.; Kinjo, K.; Inoue, T.; Iseki, C.; Takishita, S. Body mass index and the risk of development of end-stage renal disease in a screened cohort. Kidney Int. 2004, 65, 1870–1876.
- Hsu, C.Y.; McCulloch, C.E.; Iribarren, C.; Darbinian, J.; Go, A.S. Body mass index and risk for end-stage renal disease. Ann. Intern. Med. 2006, 144, 21–28.
- Tanner, R.M.; Brown, T.M.; Muntner, P. Epidemiology of Obesity, the Metabolic Syndrome, and Chronic Kidney Disease. Curr. Hypertens. Rep. 2012, 14, 152–159.
- Kramer, H.J.; Saranathan, A.; Luke, A.; Durazo-Arvizu, R.A.; Guichan, C.; Hou, S.; Cooper, R. Increasing body mass index and obesity in the incident ESRD population. J. Am. Soc. Nephrol. 2006, 17, 1453–1459.
- Wang, Z.; Zhang, J.; Chan, S.; Cameron, A.; Healy, H.G.; Venuthurupalli, S.K.; Tan, K.-S.; Hoy, W.E. BMI and its association with death and the initiation of renal replacement therapy (RRT) in a cohort of patients with chronic kidney disease (CKD). BMC Nephrol. 2019, 20, 329.
- Bergmann, C.; Guay-Woodford, L.M.; Harris, P.C.; Horie, S.; Peters, D.J.M.; Torres, V.E. Polycystic kidney disease. Nat. Rev. Dis. Primers. 2018, 4, 50.
- Cornec-Le Gall, E.; Alam, A.; Perrone, R.D. Autosomal dominant polycystic kidney disease. Lancet 2019, 393, 919–935.
- Schrier, R.W.; Abebe, K.Z.; Perrone, R.D.; Torres, V.E.; Braun, W.E.; Steinman, T.I.; Winklhofer, F.T.; Brosnahan, G.; Czarnecki, P.G.; Hogan, M.C.; et al. Blood Pressure in Early Autosomal Dominant Polycystic Kidney Disease. N. Engl. J. Med. 2014, 371, 2255–2266.
- Nowak, K.L.; Steele, C.; Gitomer, B.; Wang, W.; Ouyang, J.; Chonchol, M.B. Overweight and Obesity and Progression of ADPKD. Clin. J. Am. Soc. Nephrol. 2021, 16, 908–915.
- Wang, Y.; Chen, X.; Song, Y.; Caballero, B.; Cheskin, L.J. Association between obesity and kidney disease: A systematic review and meta-analysis. Kidney Int. 2008, 73, 19–33.
- Pinto-Sietsma, S.-J.; Navis, G.; Janssen, W.M.T.; de Zeeuw, D.; Gans, R.O.B.; de Jong, P.E. A central body fat distribution is related to renal function impairment, even in lean subjects. Am. J. Kidney Dis. 2003, 41, 733–741.
- Chang, A.; Van Horn, L.; Jacobs, D.R., Jr.; Liu, K.; Muntner, P.; Newsome, B.; Shoham, D.A.; Durazo-Arvizu, R.; Bibbins-Domingo, K.; Reis, J.; et al. Lifestyle-related factors, obesity, and incident microalbuminuria: The CARDIA (Coronary Artery Risk Development in Young Adults) study. Am. J. Kidney Dis. 2013, 62, 267–275.
- Thoenes, M.; Reil, J.C.; Khan, B.V.; Bramlage, P.; Volpe, M.; Kirch, W.; Böhm, M. Abdominal obesity is associated with microalbuminuria and an elevated cardiovascular risk profile in patients with hypertension. Vasc. Health Risk Manag. 2009, 5, 577–585.
- Foster, M.C.; Hwang, S.J.; Massaro, J.M.; Hoffmann, U.; DeBoer, I.H.; Robins, S.J.; Vasan, R.S.; Fox, C.S. Association of subcutaneous and visceral adiposity with albuminuria: The Framingham Heart Study. Obesity 2011, 19, 1284–1289.
- Gelber, R.P.; Kurth, T.; Kausz, A.T.; Manson, J.E.; Buring, J.E.; Levey, A.S.; Gaziano, J.M. Association between body mass index and CKD in apparently healthy men. Am. J. Kidney Dis. 2005, 46, 871–880.
- Kramer, H.; Luke, A.; Bidani, A.; Cao, G.; Cooper, R.; McGee, D. Obesity and prevalent and incident CKD: The Hypertension Detection and Follow-Up Program. Am. J. Kidney Dis. 2005, 46, 587–594.
- de Boer, I.H.; Katz, R.; Fried, L.F.; Ix, J.H.; Luchsinger, J.; Sarnak, M.J.; Shlipak, M.G.; Siscovick, D.S.; Kestenbaum, B. Obesity and change in estimated GFR among older adults. Am. J. Kidney Dis. 2009, 54, 1043–1051.
- Lu, J.L.; Molnar, M.Z.; Naseer, A.; Mikkelsen, M.K.; Kalantar-Zadeh, K.; Kovesdy, C.P. Association of age and BMI with kidney function and mortality: A cohort study. Lancet Diabetes Endocrinol. 2015, 3, 704–714.
- Vivante, A.; Golan, E.; Tzur, D.; Leiba, A.; Tirosh, A.; Skorecki, K.; Calderon-Margalit, R. Body mass index in 1.2 million adolescents and risk for end-stage renal disease. Arch. Intern. Med. 2012, 172, 1644–1650.
- Bray, G.A. Overweight is risking fate. Definition, classification, prevalence, and risks. Ann. N. Y. Acad. Sci. 1987, 499, 14–28.
- Chang, T.-J.; Zheng, C.-M.; Wu, M.-Y.; Chen, T.-T.; Wu, Y.-C.; Wu, Y.-L.; Lin, H.-T.; Zheng, J.-Q.; Chu, N.-F.; Lin, Y.-M.; et al. Relationship between body mass index and renal function deterioration among the Taiwanese chronic kidney disease population. Sci. Rep. 2018, 8, 6908.
- Herrington, W.G.; Smith, M.; Bankhead, C.; Matsushita, K.; Stevens, S.; Holt, T.; Hobbs, F.D.R.; Coresh, J.; Woodward, M. Body-mass index and risk of advanced chronic kidney disease: Prospective analyses from a primary care cohort of 1.4 million adults in England. PLoS ONE 2017, 12, e0173515.
- Iseki, K. Body mass index and the risk of chronic renal failure: The Asian experience. Contrib. Nephrol. 2006, 151, 42–56.
- Shankar, A.; Leng, C.; Chia, K.S.; Koh, D.; Tai, E.S.; Saw, S.M.; Lim, S.C.; Wong, T.Y. Association between body mass index and chronic kidney disease in men and women: Population-based study of Malay adults in Singapore. Nephrol. Dial. Transplant. 2008, 23, 1910–1918.
- Horber, F.F.; Gruber, B.; Thomi, F.; Jensen, E.X.; Jaeger, P. Effect of sex and age on bone mass, body composition and fuel metabolism in humans. Nutrition 1997, 13, 524–534.
- Kuk, J.L.; Lee, S.; Heymsfield, S.B.; Ross, R. Waist circumference and abdominal adipose tissue distribution: Influence of age and sex. Am. J. Clin. Nutr. 2005, 81, 1330–1334.
- Othman, M.; Kawar, B.; El Nahas, A.M. Influence of obesity on progression of non-diabetic chronic kidney disease: A retrospective cohort study. Nephron. Clin. Pract. 2009, 113, c16–c23.
- MacLaughlin, H.L.; Pike, M.; Selby, N.M.; Siew, E.; Chinchilli, V.M.; Guide, A.; Stewart, T.G.; Himmelfarb, J.; Go, A.S.; Parikh, C.R.; et al. Body mass index and chronic kidney disease outcomes after acute kidney injury: A prospective matched cohort study. BMC Nephrol. 2021, 22, 200.
- Khedr, A.; Khedr, E.; House, A.A. Body mass index and the risk of progression of chronic kidney disease. J. Ren. Nutr. 2011, 21, 455–461.
- Mohsen, A.; Brown, R.; Hoefield, R.; Kalra, P.A.; O’Donoghue, D.; Middleton, R.; New, D. Body mass index has no effect on rate of progression of chronic kidney disease in subjects with type 2 diabetes mellitus. J. Nephrol. 2012, 25, 384–393.
- Brown, R.N.K.L.; Mohsen, A.; Green, D.; Hoefield, R.A.; Summers, L.K.M.; Middleton, R.J.; O’Donoghue, D.J.; Kalra, P.A.; New, D.I. Body mass index has no effect on rate of progression of chronic kidney disease in non-diabetic subjects. Nephrol. Dial. Transplant. 2012, 27, 2776–2780.
- Lowrie, E.G.; Lew, N.L. Death risk in hemodialysis patients: The predictive value of commonly measured variables and an evaluation of death rate differences between facilities. Am. J. Kidney Dis. 1990, 15, 458–482.
- Kalantar-Zadeh, K.; Block, G.; Humphreys, M.H.; Kopple, J.D. Reverse epidemiology of cardiovascular risk factors in maintenance dialysis patients. Kidney Int. 2003, 63, 793–808.
- Kalantar-Zadeh, K.; Block, G.; Horwich, T.; Fonarow, G.C. Reverse epidemiology of conventional cardiovascular risk factors in patients with chronic heart failure. J. Am. Coll. Cardiol. 2004, 43, 1439–1444.
- Leavey, S.F.; McCullough, K.; Hecking, E.; Goodkin, D.; Port, F.K.; Young, E.W. Body mass index and mortality in ‘healthier’ as compared with ‘sicker’ haemodialysis patients: Results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol. Dial. Transplant. 2001, 16, 2386–2394.
- Molnar, M.Z.; Streja, E.; Kovesdy, C.P.; Bunnapradist, S.; Sampaio, M.S.; Jing, J.; Krishnan, M.; Nissenson, A.R.; Danovitch, G.M.; Kalantar-Zadeh, K. Associations of body mass index and weight loss with mortality in transplant-waitlisted maintenance hemodialysis patients. Am. J. Transplant. 2011, 11, 725–736.
- Horwich, T.B.; Fonarow, G.C.; Hamilton, M.A.; MacLellan, W.R.; Woo, M.A.; Tillisch, J.H. The relationship between obesity and mortality in patients with heart failure. J. Am. Coll. Cardiol. 2001, 38, 789–795.
- Fung, F.; Sherrard, D.J.; Gillen, D.L.; Wong, C.; Kestenbaum, B.; Seliger, S.; Ball, A.; Stehman-Breen, C. Increased risk for cardiovascular mortality among malnourished end-stage renal disease patients. Am. J. Kidney Dis. 2002, 40, 307–314.
- Lee, M.J.; Park, J.T.; Park, K.S.; Kwon, Y.E.; Han, S.H.; Kang, S.-W.; Choi, K.H.; Oh, K.-H.; Park, S.K.; Chae, D.W.; et al. Normal body mass index with central obesity has increased risk of coronary artery calcification in Korean patients with chronic kidney disease. Kidney Int. 2016, 90, 1368–1376.
- Grantham, J.J.; Torres, V.E.; Chapman, A.B.; Guay-Woodford, L.M.; Bae, K.T.; King, B.F.; Wetzel, L.H.; Baumgarten, D.A.; Kenney, P.J.; Harris, P.C.; et al. Volume Progression in Polycystic Kidney Disease. N. Engl. J. Med. 2006, 354, 2122–2130.
- Irazabal, M.V.; Rangel, L.J.; Bergstralh, E.J.; Osborn, S.L.; Harmon, A.J.; Sundsbak, J.L.; Bae, K.T.; Chapman, A.B.; Grantham, J.J.; Mrug, M.; et al. Imaging Classification of Autosomal Dominant Polycystic Kidney Disease: A Simple Model for Selecting Patients for Clinical Trials. J. Am. Soc. Nephrol. 2015, 26, 160–172.
- Torres, V.E.; Chapman, A.B.; Perrone, R.D.; Bae, K.T.; Abebe, K.Z.; Bost, J.E.; Miskulin, D.C.; Steinman, T.I.; Braun, W.E.; Winklhofer, F.T.; et al. Analysis of baseline parameters in the HALT polycystic kidney disease trials. Kidney Int. 2012, 81, 577–585.
- Nowak, K.L.; You, Z.; Gitomer, B.; Brosnahan, G.; Torres, V.E.; Chapman, A.B.; Perrone, R.D.; Steinman, T.I.; Abebe, K.Z.; Rahbari-Oskoui, F.F.; et al. Overweight and Obesity Are Predictors of Progression in Early Autosomal Dominant Polycystic Kidney Disease. J. Am. Soc. Nephrol. 2018, 29, 571–578.
- Freise, J.; Tavakol, M.; Gao, Y.; Klein, O.; Lee, B.K.; Freise, C.; Park, M. The Effect of Enlarged Kidneys on Calculated Body Mass Index Categorization in Transplant Recipients With ADPKD. Kidney Int. Rep. 2019, 4, 606–609.
- Barberio, A.M.; Alareeki, A.; Viner, B.; Pader, J.; Vena, J.E.; Arora, P.; Friedenreich, C.M.; Brenner, D.R. Central body fatness is a stronger predictor of cancer risk than overall body size. Nat. Commun. 2019, 10, 383.
- Pi-Sunyer, F.X. The epidemiology of central fat distribution in relation to disease. Nutr. Rev. 2004, 62, S120–S126.
- Choe, S.S.; Huh, J.Y.; Hwang, I.J.; Kim, J.I.; Kim, J.B. Adipose Tissue Remodeling: Its Role in Energy Metabolism and Metabolic Disorders. Front. Endocrinol. 2016, 7, 30.
- Chait, A.; den Hartigh, L.J. Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease. Front. Cardiovasc. Med. 2020, 7, 22.
- Nowak, K.L.; Hopp, K. Metabolic Reprogramming in Autosomal Dominant Polycystic Kidney Disease: Evidence and Therapeutic Potential. Clin. J. Am. Soc. Nephrol. 2020, 15, 577–584.
- Shuster, A.; Patlas, M.; Pinthus, J.H.; Mourtzakis, M. The clinical importance of visceral adiposity: A critical review of methods for visceral adipose tissue analysis. Br. J. Radiol. 2012, 85, 1–10.
- Burhans, M.S.; Hagman, D.K.; Kuzma, J.N.; Schmidt, K.A.; Kratz, M. Contribution of Adipose Tissue Inflammation to the Development of Type 2 Diabetes Mellitus. Compr. Physiol. 2018, 9, 1–58.
- Young, J.A.; Hwang, S.-J.; Sarnak, M.J.; Hoffmann, U.; Massaro, J.M.; Levy, D.; Benjamin, E.J.; Larson, M.G.; Vasan, R.S.; O’Donnell, C.J.; et al. Association of visceral and subcutaneous adiposity with kidney function. Clin. J. Am. Soc. Nephrol. CJASN 2008, 3, 1786–1791.
- Reddy, P.; Lent-Schochet, D.; Ramakrishnan, N.; McLaughlin, M.; Jialal, I. Metabolic syndrome is an inflammatory disorder: A conspiracy between adipose tissue and phagocytes. Clin. Chim. Acta 2019, 496, 35–44.
- Kahn, C.R.; Wang, G.; Lee, K.Y. Altered adipose tissue and adipocyte function in the pathogenesis of metabolic syndrome. J. Clin. Investig. 2019, 129, 3990–4000.
- Zhang, Y.; Hao, J.; Tarrago, M.G.; Warner, G.M.; Giorgadze, N.; Wei, Q.; Huang, Y.; He, K.; Chen, C.; Peclat, T.R.; et al. FBF1 deficiency promotes beiging and healthy expansion of white adipose tissue. Cell Rep. 2021, 36, 109481.
- Reyes-Farias, M.; Fos-Domenech, J.; Serra, D.; Herrero, L.; Sánchez-Infantes, D. White adipose tissue dysfunction in obesity and aging. Biochem. Pharmacol. 2021, 192, 114723.
- Okhunov, Z.; Mues, A.C.; Kline, M.; Haramis, G.; Xu, B.; Mirabile, G.; Vira, M.; Landman, J. Evaluation of perirenal fat as a predictor of cT 1a renal cortical neoplasm histopathology and surgical outcomes. J. Endourol. 2012, 26, 911–916.
- Foster, M.C.; Hwang, S.J.; Porter, S.A.; Massaro, J.M.; Hoffmann, U.; Fox, C.S. Fatty kidney, hypertension, and chronic kidney disease: The Framingham Heart Study. Hypertens 2011, 58, 784–790.
- Wei, G.; Sun, H.; Dong, K.; Hu, L.; Wang, Q.; Zhuang, Q.; Zhu, Y.; Zhang, X.; Shao, Y.; Tang, H.; et al. The thermogenic activity of adjacent adipocytes fuels the progression of ccRCC and compromises anti-tumor therapeutic efficacy. Cell Metab. 2021, 33, 2021–2039.e8.
- Ahima, R.S.; Lazar, M.A. Adipokines and the peripheral and neural control of energy balance. Mol. Endocrinol. 2008, 22, 1023–1031.
- Considine, R.V.; Sinha, M.K.; Heiman, M.L.; Kriauciunas, A.; Stephens, T.W.; Nyce, M.R.; Ohannesian, J.P.; Marco, C.C.; McKee, L.J.; Bauer, T.L.; et al. Serum immunoreactive-leptin concentrations in normal-weight and obese humans. N. Engl. J. Med. 1996, 334, 292–295.
- de Souza Batista, C.M.; Yang, R.Z.; Lee, M.J.; Glynn, N.M.; Yu, D.Z.; Pray, J.; Ndubuizu, K.; Patil, S.; Schwartz, A.; Kligman, M.; et al. Omentin plasma levels and gene expression are decreased in obesity. Diabetes 2007, 56, 1655–1661.
- Samaras, K.; Botelho, N.K.; Chisholm, D.J.; Lord, R.V. Subcutaneous and visceral adipose tissue gene expression of serum adipokines that predict type 2 diabetes. Obesity 2010, 18, 884–889.
- Degawa-Yamauchi, M.; Bovenkerk, J.E.; Juliar, B.E.; Watson, W.; Kerr, K.; Jones, R.; Zhu, Q.; Considine, R.V. Serum resistin (FIZZ3) protein is increased in obese humans. J. Clin. Endocrinol. Metab. 2003, 88, 5452–5455.
- McTernan, P.G.; McTernan, C.L.; Chetty, R.; Jenner, K.; Fisher, F.M.; Lauer, M.N.; Crocker, J.; Barnett, A.H.; Kumar, S. Increased resistin gene and protein expression in human abdominal adipose tissue. J. Clin. Endocrinol. Metab. 2002, 87, 2407–2410.
- Zhang, X.; Yeung, D.C.; Karpisek, M.; Stejskal, D.; Zhou, Z.G.; Liu, F.; Wong, R.L.; Chow, W.S.; Tso, A.W.; Lam, K.S.; et al. Serum FGF21 levels are increased in obesity and are independently associated with the metabolic syndrome in humans. Diabetes. 2008, 57, 1246–1253.
- Bastard, J.P.; Jardel, C.; Bruckert, E.; Blondy, P.; Capeau, J.; Laville, M.; Vidal, H.; Hainque, B. Elevated levels of interleukin 6 are reduced in serum and subcutaneous adipose tissue of obese women after weight loss. J. Clin. Endocrinol. Metab. 2000, 85, 3338–3342.
- Pickup, J.C.; Chusney, G.D.; Thomas, S.M.; Burt, D. Plasma interleukin-6, tumour necrosis factor alpha and blood cytokine production in type 2 diabetes. Life Sci. 2000, 67, 291–300.
- Christiansen, T.; Richelsen, B.; Bruun, J.M. Monocyte chemoattractant protein-1 is produced in isolated adipocytes, associated with adiposity and reduced after weight loss in morbid obese subjects. Int. J. Obes. 2005, 29, 146–150.
- Yang, R.Z.; Lee, M.J.; Hu, H.; Pollin, T.I.; Ryan, A.S.; Nicklas, B.J.; Snitker, S.; Horenstein, R.B.; Hull, K.; Goldberg, N.H.; et al. Acute-phase serum amyloid A: An inflammatory adipokine and potential link between obesity and its metabolic complications. PLoS Med. 2006, 3, e287.
- Sag, S.; Yildiz, A.; Gullulu, S.; Gungoren, F.; Ozdemir, B.; Cegilli, E.; Oruc, A.; Ersoy, A.; Gullulu, M. Early atherosclerosis in normotensive patients with autosomal dominant polycystic kidney disease: The relation between epicardial adipose tissue thickness and carotid intima-media thickness. Springerplus. 2016, 5, 211.
More