Hepatocellular carcinoma (HCC) causes many deaths worldwide, and current treatments have limitations. Immunotherapies have shown the most promising clinical outcomes for advanced HCC. However, there are many patients with HCC who still respond poorly to these treatments. Circulating biomarkers that can easily be obtained through blood sampling are promising in predicting treatment responses, since they are minimally invasive and enable us to constantly monitor disease progression.
- hepatocellular carcinoma (HCC)
- immunotherapies
- liquid biopsy
- circulating tumor DNA (ctDNA)
- circulating tumor cells (CTC)
1. Introduction
2. Liquid Biopsy in HCC
Liquid biopsy refers to all the non-solid biologic materials used for the diagnosis and monitoring of HCC and is mainly based on the detection of ctDNA [24][25][26][24,25,26], circulating RNAs (e.g., microRNAs) [27][28][29][27,28,29], CTCs [20][30][31][20,30,31] and extracellular vesicles (EVs) (e.g., exosomes) [32][33][34][32,33,34] (Figure 1). In the following paragraphs, we will focus on two of the most promising liquid biopsy types in HCC, ctDNA and CTCs.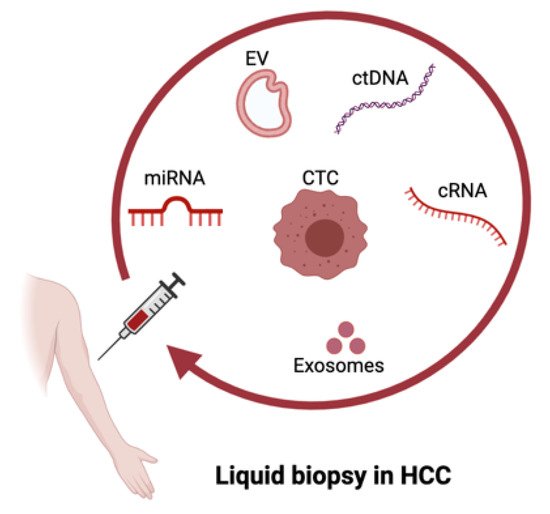
2.1. ctDNA in HCC
2.2. CTCs in HCC
CTCs are also emerging as a promising biomarker for the prediction of HCC treatment efficacies. CTCs arise in the circulation after detachment from primary or metastatic tumor lesions [44][49]. They differ from other types of cancer biomarkers as they represent viable tumor cells circulating in the patient’s bloodstream. Therefore, CTCs can also provide comprehensive genetic information about tumor heterogeneity and drug sensitivity [20]. CTCs have been approved by the FDA as diagnostic markers for specific epithelial cancers [16]. However, their diagnostic role in HCC still requires further studies. A widely known CTC biomarker is the epithelial cell adhesion molecule (EpCAM) [44][49], a pan-cancer biomarker which has also been observed in HCC patients [45][50].
Despite the highly promising role of CTCs as a biomarker for HCC [20], it remains challenging to detect HCC CTCs early and accurately because of the lack of specific markers. Another limitation is that the frequencies of CTCs are usually low in the circulation, especially at the early stages [16][20][16,20]. Thus, combinational strategies may be needed, in order to improve the prognostic and diagnostic value of HCC.
3. Liquid Biopsy as a Diagnostic and Prognostic Tool
Liquid biopsy has been explored as a way to monitor cancer prognosis and diagnosis in a non-invasive manner. This technology has shown promising results in early diagnosis [46][84], detection of minimal residual disease [47][85] and decision making for systemic therapies of different types of cancers, including HCC [8][48][49][8,43,86].
Among all liquid biopsy analytes, ctDNA plays an important role in HCC prognosis [17]. ctDNA maintains the same genomic signatures that are present in the matching tumor tissue, allowing for the quantitative and qualitative evaluation of the mutation burden in body fluids [50][87]. In this way, ctDNA has been considered as a good biomarker and can be utilized in disease monitoring. The data of ctDNA include quantitative changes, such as differences in the concentration of ctDNA, as well as qualitative changes, such as gene mutations, DNA copy number variations and DNA methylation [16]. Indicatively, studies based on the detection of somatic single-nucleotide mutations and methylation changes in ctDNA could closely correlate with tumor burden over time in HCC patients and could be used to predict recurrence after surgery [17][51][52][17,88,89].
As ctDNA represents only a very small proportion of cell-free DNA, very sensitive and reliable detection methods are required. Levels of ctDNA are measured mainly by real-time PCR (RT-PCR) [53][93], while digital PCR (dPCR) [54][94] or sequencing methods are used for the detection of point mutations [55][95]. In addition to TERT and TP53 mutations as the prognostic factors of poor survival [56][57][45,47], other mutations have been shown to have prognostic values for HCC. MLH1 mutation was specifically associated with lower survival [1], whereas mutations of genes from the PI3K/mTOR pathway were shown to be the predictors of non-responders to TKI treatments for patients with advanced HCC [49][86].
A number of studies have also shown the prognostic values of circulating miRNAs in HCC. Lower survival rates were associated with patients with low levels of miR-1, miR-122, miR-26a, miR-29a and miR-223-3p [58][59][60][61][96,97,98,99] or high levels of miR-155, miR-96 and miR-193-5p [62][63][100,101]. Furthermore, six additional miRNAs were identified as prognostic factors. Low levels of miR-424-5p or miR- 101-3p and high levels of miR-128, miR-139-5p, miR-382-5p and miR410 were associated with lower survival rates in HCC patients [17]. Alternatively, miRNAs have been studied in association with EVs [32][33][34][32,33,34]. In a cohort of 59 HCC patients, a correlation was found between tumor recurrences after liver transplantation and a high level of exosomal miR-718 [64][102]. Additionally, high levels of exosomal miR-665 or low levels of exosomal miR-638 and miR-320a were identified as predictors of poor survival [65][66][67][103,104,105].
Another cornerstone of liquid biopsy is the isolation and detection of CTCs, which have been described as a useful tool for the prognostication of HCC [68][106]. As introduced above, EpCAM-positive CTC cells have been intensively investigated in HCC [45][69][50,51]. However, since CTCs can lose their epithelial phenotype through epithelial-to-mesenchymal transition (EMT) in order to survive and metastasize [44][49], EpCAM cannot always be considered an optimal biomarker to detect HCC. Alternatively, other phenotypic markers have been explored, such as the hepatocyte-specific asialoglycoprotein receptor (ASGPR) [70][67], and the hepatocyte paraffin 1 [71][107], or incorporation of several markers simultaneously, as it has extensively been reviewed elsewhere [20]. Most recently, in a prospective study of 80 HCC patients, a multimarker assay combining cell surface markers EpCAM, ASGPR and GPC3 was able to detect HCC CTCs in 97% of the patients with high accuracy. Moreover, a phenotypic variant subset of CTCs was associated with aggressive disease progression and underlying metastasis, therefore highlighting the important implications of CTCs in treatment selection [72][108]. Another study showed that the detection of phosphorylated ERK (pERK) and pAkt in CTCs could predict the response to sorafenib efficacy in advanced HCC patients, similarly to tumor tissue biopsy [73][59].
4. Liquid Biopsy for Immunotherapy in HCC
The race towards the identification of immunotherapy predictive biomarkers is at the forefront of research in HCC. Among the biomarkers of interest, there are TMB and mutational signatures identified from ctDNA, and PD-L1 expression detected on CTCs [74][125]. TMB and PD-L1 expression are considered good predictors in several cancers, but the evidence in liver cancer has not been as established thus far [75][117]. In Table 1, we summarize the most recent literature in the field, and we highlight the key findings for each study.
| Type of Biomarker Analyzed | Key Findings | Reference |
|---|
| Changes in the ctDNA levels | Could significantly correlate with tumor size in cancer patients treated with anti-PD1 drugs and be a valuable prognostic factor of progression-free and overall survival. | [76] | [126] |
| Targeted gene analysis of ctDNA | Can be a better option to evaluate TMB prior to immunotherapy in cases of advanced primary liver cancers when tissue biopsy is not recommended. | [18] | |
| Mutational analysis of ctDNA | Could not be associated with response to ICI therapy but only to systemic treatment. | [36] | |
| Levels of ctDNA at baseline | Higher levels of ctDNA at baseline were associated with an increased baseline tumor burden, and ctDNA turned negative in 70%, 27%, 9% and 0% of patients achieving a complete response, partial response, stable disease and disease progression, respectively. | [77] | [128] |
| Undetectable ctDNA levels during treatment were linked to a longer progression-free survival. | |||
| Hyper-mutated ctDNA phenotype | Is associated with a favorable outcome in a cohort of 69 cancer patients with different histologies, including three HCC patients, treated with different immune checkpoint inhibitors. | [78] | [122] |
| Overall response rate, PFS and OS in high-alteration groups were significantly higher than in low-alteration groups. | |||
| Detection of Wnt/b-catenin-activating mutations | Wnt/b-catenin-activating mutations in HCC linked to potential tumor immunotherapy resistance in several studies. | [79][80][81][82] | [129,130,131,132] |
| Detection of Wnt/b-catenin-activating mutations | Demonstration that liquid biopsy is potentially able to detect Wnt/b-catenin-activating mutations in HCC. | [75] | [117] |
| Detection of Wnt/b-catenin-activating mutations | Detection of Wnt/b-catenin pathway-activating mutations might not be sufficient to identify advanced HCC patients with primary resistance to ICI. | [83] | [119] |
| Targeted mutational analysis of CTNNB1 p.T41A mutation | ctDNA liquid biopsy managed to reveal mutations that were not detected in single tumor biopsies, thus increasing the detection rate of CTNNB1 mutation in HCC patients. | [84] | [134] |
| PD-L1 expression on CTCs | Biomarker to assess ICI-based immunotherapy efficacy of advanced solid tumors. | [85] | [135] |
| CTCs expressing PD-L1 | PD-L1-positive CTCs are mainly found in advanced stages of disease, and they represent an independent prognostic factor for overall survival. 6 out of 10 patients receiving anti-PD-1 treatment had PD-L1-positive CTCs at baseline, and of these, 5 out of 6 had a favorable treatment response. 4 out of 10 patients receiving anti-PD-1 treatment did not have PD-L1+ CTCs and were non-responders. |
[86] | [136] |