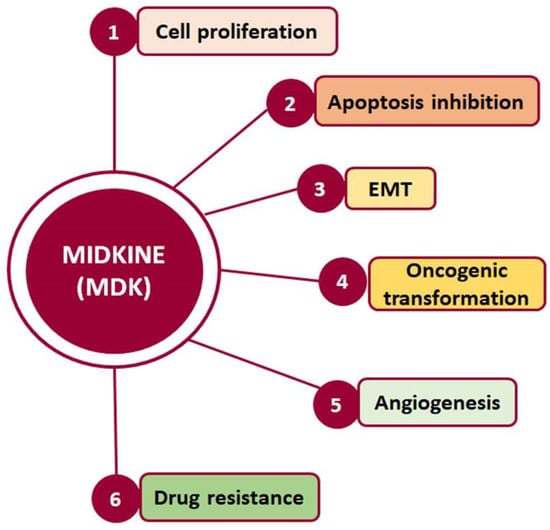
Midkine (MDK) is a multifunctional secreted protein that can act as a cytokine or growth factor regulating multiple signaling pathways and being implicated in fundamental cellular processes, such as survival, proliferation, and migration. Although its expression in normal adult tissues is barely detectable, MDK serum levels are found to be elevated in several types of cancer, including hepatocellular carcinoma (HCC).
- metastasis
- EMT
- AFP
- liver cancer
- NEGF-2
1. Hepatocellular Carcinoma
2. MDK-Mediated Signaling and Cellular Function
Midkine (MDK) is a multifunctional secreted protein that has emerged as a promising biomarker with the potential to aid in early diagnosis and intervention [5][7]. MDK, also known as neurite growth-promoting factor-2 (NEGF-2), amphiregulin-associated protein (ARAP), mid-gestation and kidney protein, and retinoic acid inducible factor, is a 13 kDa cysteine-rich protein encoded by the MDK gene [6][14], which is located on chromosome 11 [7][15]. It was originally discovered as a highly expressed gene during mouse embryogenesis [8][16] and, to date, seven MDK mRNA isoforms have been reported due to alternative splicing and differences in the transcription initiation site [9][17]. Classified as a heparin-binding protein, MDK can act as a cytokine or growth factor [6][8][10][14,16,18]. It is composed of two domains, each including three antiparallel β-strands and various heparin-binding consensus sites [6][14], which enable its binding to heparan sulfate and chondroitin sulfate and the formation of a molecular complex with proteoglycans [10][18]. Importantly, MDK binding to sulfated glycosaminoglycans (GAGs) leads to interactions with several key receptors, including protein-tyrosine phosphatase-ζ (PTP-ζ), syndecans, low-density lipoprotein receptor-related protein (LRP), α4β1 and α6β1 integrins, and neurogenic locus notch homolog protein 2 (Notch-2), while it has also been reported to phosphorylate the cell-matrix adhesion proteins paxillin and focal adhesion kinase (FAK) [11][19] (Figure 1).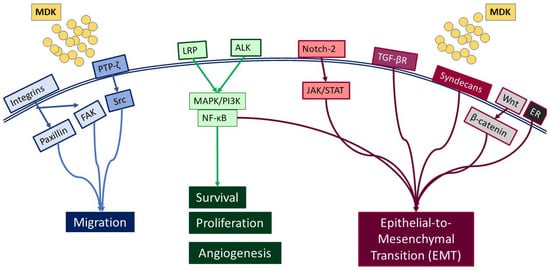
3. MDK Localization, Expression, and Detection
4. MDK’s Potential as a Biomarker for HCC Diagnosis and Progression
3. MDK Localization, Expression, and Detection
4. MDK’s Potential as a Biomarker for HCC Diagnosis and Progression
MDK was therefore proposed as a potential biomarker over a decade ago, as its levels were observed to be elevated in the serum of HCC patients. Indeed, several studies have shown that MDK is upregulated in HCC patients compared with healthy individuals More specifically, Omran et al. [28][37] assessed MDK serum levels by ELISA, initially in 104 HCC patients and 92 individuals with non-malignant liver disease, and subsequently in 80 HCC patients and 42 patients with liver cirrhosis. They found elevated MDK levels in HCC patients compared with cirrhotic patients, suggesting MDK’s potential as a distinctive marker in HCC diagnosis and its differentiation from cirrhosis. Notably, a recent comprehensive study in HCC using bioinformatics analysis approaches identified 10 hub genes from protein–protein interaction networks, among which MDK was further verified by polymerase chain reaction (PCR) and immunohistochemistry (IHC) and found to be highly expressed in HCC [29][41]. Interestingly, Sun et al. [15][23] showed elevated MDK levels in the serum of 341 HCC patients who also had curative partial hepatectomy compared with healthy individuals. More importantly, these were positively correlated with increased recurrence rate compared with normal MDK levels. Moreover, they analyzed MDK mRNA expression in nine HCC cell lines (PLC/PRF5/F, Huh7, Hep3B, HepG2, SMMC7721, MHCC97L, and MHCC97H) and two normal liver cell lines (WRL68 and Chang liver) and showed that although MDK mRNA expression varied significantly among the HCC cell lines tested, in all cases it was much higher than that in the normal cell lines used. Moreover, they continued with a series of in vitro and in vivo experiments and reported a negative correlation of differential MDK expression in the cell lines tested with resistance to suspension-induced cell death, known as anoikis. Moreover, PLC/PRF/5 cells lacking MDK via small interfering RNA (siRNA)-mediated silencing exhibited reduced in vitro expression of pro-apoptotic caspase-3 and Bax and a concurrent upregulation of anti-apoptotic B-cell lymphoma 2 (Bcl2) and tropomyosin receptor kinase B (TrkB), a known and potent suppressor of anoikis.5. MDK in Comparison with AFP
Few studies showed no correlation with AFP levels. Specifically, Saad et al. [30][42] determined MDK mRNA expression using real-time PCR in 29 patients with HCC and compared it with that of 7 healthy individuals, 27 patients who had chronic HCV, and 18 patients who had liver cirrhosis. They found that MDK mRNA expression was higher in HCC patients compared with the other groups. However, no significant correlation was observed between MDK and tumor characteristics (number of nodules, lesion size, and extrahepatic metastases) or AFP levels. In agreement with the above, Shaheen et al. [7][15], evaluated MDK protein levels as a biomarker in patients with newly diagnosed HCC. Among 100 participants, including 40 HCC patients, 30 liver cirrhosis patients, and 30 controls, MDK was found to be significantly upregulated in HCC patients compared with both liver cirrhosis patients and controls but showed no association with tumor diameter, number of nodules, AFP levels, or Barcelona Clinic liver cancer (BCLC) staging, which is widely used for staging primary liver cancer. However, it is worth noting that MDK showed greater sensitivity compared with AFP in HCC diagnosis, especially in the early stages, highlighting its potential as a novel marker, especially in differentiating HCC from liver cirrhosis.
The majority of studies, however, showed that MDK provides some additional advantages as a biomarker compared with AFP. Specifically, in a recent study [31][43], serum MDK levels were assessed in 238 individuals, including 78 HCC patients with HCV-related HCC, 40 with HCV-related liver cirrhosis, 40 with chronic HCV without liver cirrhosis, and 80 healthy controls. The findings consistently confirmed elevated MDK levels in HCC patients compared with other groups. However, although no association with tumor size was found, and while there was no significant difference in MDK protein expression between the other groups, the authors highlighted that MDK diagnostic accuracy for HCC diagnosis was high.
Interestingly, in a recent phase II validation study, Zhu et al. [32][44] evaluated MDK as a diagnostic biomarker in early-stage HCC for those with negative AFP. Their study also included in vitro work in nine HCC cell lines (Bel-7402, Huh-7, HCCLM3, MHCC97H, PLC, HepG2, and Hep3B, with L-O2 and Chang liver cells serving as controls), as well as evaluation of 88 HCC samples, their corresponding adjacent tissues, and serum samples from 388 HCC cases and 545 controls. MDK expression was evaluated using IHC in tissue microarrays (TMA), ELISA in serum samples, and Western blotting in cell lines. They found elevated MDK protein expression in all HCC cell lines compared with controls, while IHC analysis in the TMA exhibited high MDK expression in the form of diffused cytoplasmic staining in 72% of HCCs compared with normal adjacent liver tissue or cancer-free cirrhotic samples. Although serum MDK levels did not exhibit correlations with tumor aggressiveness indicators, such as poor differentiation, microvascular invasion, larger tumor size, advanced tumor stage, survival, and tumor recurrence, they did correlate with MDK expression in tumor tissues. No association was found between MDK and BCLC staging. Compared with AFP, in AFP-positive patients, MDK and AFP had similar specificities; however, MDK showed superior sensitivity to AFP (86.9% and 51.9%, respectively). On the other hand, in patients with early-stage HCC and negative AFP, MDK had better performance compared with AFP for distinguishing early-stage HCC and small-sized tumors from non-HCC cases, including cirrhosis.
In another study, El-Shayeb et al. [33][45] tested MDK serum levels in 89 patients with liver cirrhosis without HCC, 86 patients with cirrhotic HCV-induced HCC, and 69 healthy controls. They found serum MDK levels to be increased in HCC patients compared with the other two control groups. Interestingly, however, MDK exhibited higher levels in patients with multiple focal lesions, lesions exceeding 5 cm, and those with portal vein thrombosis, compared with those with single focal lesions, lesions smaller than 5 cm, and those without portal vein thrombosis. Finally, MDK was proven to have superior performance compared with AFP in differentiating HCC patients from individuals with liver cirrhosis.
Furthermore, in a study by Hodeib et al. [34][47], the diagnostic utility of serum MDK compared with AFP for the diagnosis of HCC in HCV-related liver cirrhosis was evaluated. The study involved a total of 140 participants, encompassing 35 HCV patients without cirrhosis, 35 with HCV and liver cirrhosis, 35 with HCC on top of liver cirrhosis, and 35 healthy controls, and serum MDK levels were evaluated by ELISA. Their main findings showed that serum MDK levels were elevated in HCC patients compared with the other groups and did not correlate with AFP levels, but that MDK had better sensitivity in diagnosing HCC compared with AFP (98.4% vs. 97%). However, the combination of MDK and AFP had a diagnostic value of 98% for HCC diagnosis. Corroborating further the idea that a combination of MDK and AFP increases diagnostic capacity for HCC, Mashaly et al. [35][48] also evaluated serum MDK levels by ELISA in 44 HCC patients, 31 with liver cirrhosis, and 15 healthy controls. They also found increased MDK levels in HCC patients compared with cirrhotic patients and controls. More importantly, 21 out of the 44 HCC patients were AFP-negative, but 17 of these AFP-negative patients were MDK-positive, while no correlation was revealed between MDK and AFP, suggesting the independent nature of MDK’s increase in relation to AFP. Similarly, Hung et al. [36][49] included in their study four groups: 18 samples from HCC tissues with adjacent non-cancerous liver tissues, 85 archival HCC patient samples, 165 samples from patients with active HCC, and 285 samples from individuals in remission after HCC treatment or at high risk for HCC development. MDK serum levels were assessed by ELISA, while gene expression in the tissue samples was evaluated with microarrays and real-time PCR. MDK mRNA expression was shown to be elevated in all HCC samples compared with the respective adjacent tissue samples. When measuring serum MDK and AFP levels in the 85 archival patients, they found that 25% had elevated levels of both MDK and AFP, 16% had elevated MDK levels only, 33% had elevated AFP levels only, and 26% had neither elevated MDK nor AFP, suggesting that the combination of MDK and AFP can increase the sensitivity of HCC detection. In order to assess the specificity of serum MDK in HCC detection, they also measured serum MDK levels in 72 patients with newly diagnosed HCC from the follow-up group. Of these, 60% had elevated MDK levels. Finally, Daif et al. [37][51] evaluated the gene expression of MDK in HCC patients compared with serum AFP levels in 40 HCC patients, 30 HCV patients with no evidence of HCC, and 30 healthy controls. Gene expression levels were assessed using qRT-PCR, and MDK mRNA expression was elevated in the HCC and HCV groups compared with controls. Contrary to the other studies described above, MDK alone showed lower sensitivity (50%) and specificity (68.2%) in detecting HCC compared with AFP (78.6% and 72.7% respectively). However, the combination of MDK and AFP reached a sensitivity of 71.4% and a specificity of 81.8%. Although most studies clearly demonstrated a strong, indisputable correlation between MDK levels and HCC disease progression as well as certain benefits in terms of early detection, sensitivity, or specificity compared with AFP, there was one study by Vongsuvanh et al. [38][52] showing elevated MDK levels in HCC compared with other groups (86 HCC, 86 liver cirrhosis, 86 non-cirrhotic chronic liver disease, and 86 controls), but, when compared, AFP was proven to be superior to MDK in distinguishing HCC from non-HCC cases and HCV or HBV-associated HCC from liver cirrhosis. However, MDK could differentiate NASH-related HCC from cirrhosis. In a later phase, however, they recruited 112 individuals, including 28 with HCC, 28 with HBV cirrhosis, 28 with non-cirrhotic chronic HBV, and 28 with HCV cirrhosis. MDK was elevated in 54% of the HCC patients at the time of diagnosis and, remarkably, MDK was elevated 6 months prior to diagnosis in 67% of patients, suggesting MDK’s role in pre-clinical HCC diagnosis. Last but not least, a comparison of MDK’s specificity and sensitivity with the published specificity and sensitivity of in vitro diagnostic assays such as the GAAD or GALAD score-based models shows that MDK is comparable to both GAAD and GALAD scores. More specifically, the average MDK specificity based on the 11 studies described above (Table 2) is 80.34%, while the GAAD score’s specificity is 90% [39][53] and the GALAD score’s average specificity is 87.71% [40][41][42][54,55,56]. With regard to sensitivity, the average MDK sensitivity value from the 11 studies described above (Table 2) was 83.77%, compared with 71.8% (for GAAD) [39][53] and 85.82% (the average for GALAD) [40][41][42][54,55,56]. This further demonstrates that MDK could be used in the clinic in combination with AFP, GAAD, and GALAD scores for more effective HCC diagnosis.6. Conclusions
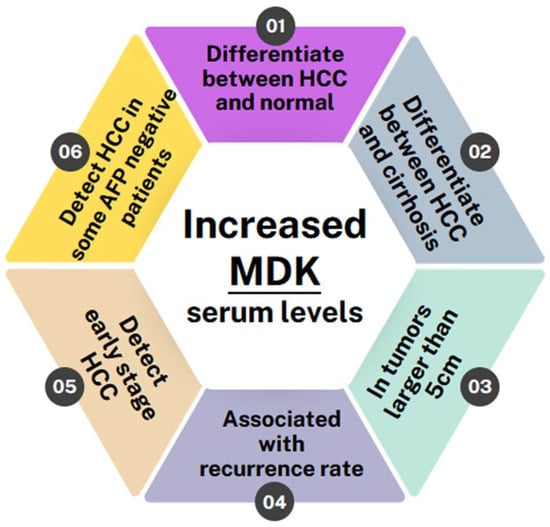
Overall, all of the studies conducted so far indicate that MDK levels are elevated in HCC patients and can, in fact, differentiate not only between HCC patients and normal individuals but also between HCC patients and patients with other liver pathologies, such as liver cirrhosis, regardless of whether it is HCV/HBV-induced or not [16][17][18][22][24][26][25,26,27,31,33,35]. Furthermore, two studies have shown MDK levels to be correlated with a tumor size greater than 5 cm [19][24][28,33] and it is also associated with high recurrence rates [12][20]. MDK was also shown to monitor disease progression and response to therapy, as it remains elevated in patients with incompletely treated or recurrent HCC while it drops after curative surgery [43][9]. Most importantly, though, MDK levels can be used to diagnose early-stage HCC and can even diagnose HCC in patients who have tested negative for AFP [30][32][33][44][45][11,42,44,45,46] (Figure 3).