The recreational use of nitrous oxide (N2O), also called laughing gas, has increased significantly in recent years. In 2022, the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) recognized it as one of the most prevalent psychoactive substances used in Europe. Chronic nitrous oxide (N2O) exposure can lead to various clinical manifestations. The most frequent symptoms are neurological (sensitive or motor disorders), but there are also other manifestations like psychiatric manifestations or cardiovascular disorders (thrombosis events). N2O also affects various neurotransmitter systems, leading to its anesthetic, analgesic, anxiolytic and antidepressant properties. N2O is very challenging to measure in biological matrices. Thus, in cases of N2O intoxication, indirect biomarkers such as vitamin B12, plasma homocysteine and plasma MMA should be explored for diagnosis and assessment.
- nitrous oxide
- cobalamin
- homocysteine
- methylmalonic acid
- vitamin
1. Introduction
2. Clinical Manifestations
2.1. Brief History of the First Reported Manifestations of Chronic N
2
O Exposure
The first adverse effects of N2O, reported in 1952, were hematological in nature described in young patients infected with tetanus to relieve their pain. One of the patients, a 15-year-old boy, died days later from septicemia and granulocytopenia secondary to severe bone marrow depression [2]. Several years later, one of the authors coined this incident as the time “when nitrous oxide lost its innocence” [3]. The first neurological adverse effects were reported in 1978 by Robert Layzer in San Francisco, even without Magnetic Resonance Imaging (MRI) and biological background [4][5][4,5]. Many case reports have since been described and the number of patients drastically increasing over time. A small increase in publications and cases were reported in the late 90′s due to an increased recreational use of N2O among dentists and healthcare givers in the USA who had easy access to the gas [6].2.2. Common Symptoms and Signs
As reported initially by Layzer, patients had a mixture of central and peripheral nervous system symptoms (Figure 1). In several examinations, subjects even alternated between hyper and hyporeflexia, as myelopathic or neuropathic influences predominated. This presentation was called “myeloneuropathy” [4].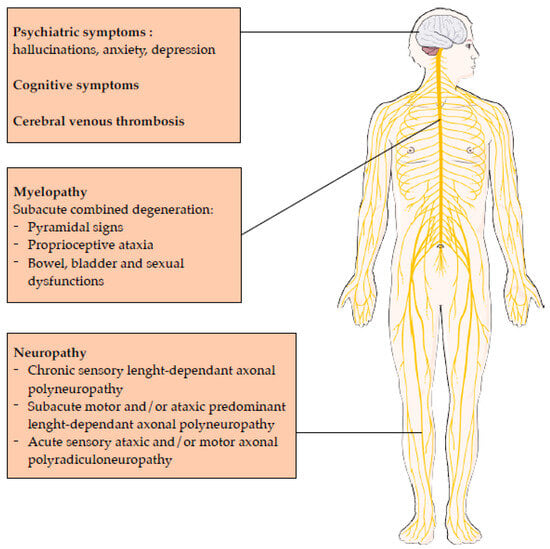
2.3. Central Nervous System Involvement
The classical spinal magnetic resonance presentation is a hypersignal on sagittal T2-weighted images in the cervical level, and to a lesser extent, in the thoracic level. An inverted “v” shaped signal is observed on the axial plane, corresponding to the dorsal columns. Interestingly, these lesions are rarely responsible for a spinal sensory level on examination. In a Chinese study describing 15 patients with spinal cord lesions, 80% had a cervical lesion and 86.7% did not have a spinal sensory level on clinical examination. This may be explained by their non-transverse nature. The vulnerability of the cervical segment had been attributed to the higher density of myelinated fibers of the dorsal columns in the cervical segment compared with the thoracic segment [8][15].2.4. Peripheral Nervous System Involvement
In the first report from Layzer in 1978, the electromyographic (EMG) examination showed normal to subnormal sensory conduction studies, with predominantly abnormal motor conduction studies. It was concluded that neuropathy was due to axonal degeneration rather than to segmental demyelination. One patient had a sural-nerve biopsy that showed only non-specific axonal degeneration [5]. Many N2O abusers have persistent paresthesia or numbness distributed in a stocking-glove pattern, suggesting a length-dependent axonal polyneuropathy. Patients have predominantly lower limb motor axonal injury, consisting of a motor length-dependent axonal polyneuropathy, sometimes associated with demyelinating injury in the upper limbs [7][8]. From an electrophysiological perspective [9][19], there seem to be specific features not usually seen in classic length-dependent polyneuropathies, such as:-
More motor and sensory nerve injury in the lower limbs compared to the upper limbs,
-
More motor nerve injury than sensory nerve injury in the lower limbs,
-
More demyelinating features in the sensory and motor nerves of the upper limbs, with a marked motor predominance.
2.5. Prognosis of Central and Neurological Nervous System Involvement
Data regarding the long-term prognosis of neurological consequences of N2O consumption is scarce. Many patients do not come back to their follow up medical appointment. A French study reported the evolution of 6 patients after a mean time of 4.9 months (interquartile range 3.0–6.25). They evaluated their Overall Neuropathy Limitations Scale, which measures disability due to peripheral neuropathy, and found that they have a score of 2 on the lower limbs on second evaluation, corresponding to an independent but abnormal looking gait [10][9].3. Pharmacological Effects
3.1. Dependence Producing Potential of Nitrous Oxide
This short-lived psychoactive effect of N2O may precipitate frequent and heavy use. Coupled with this is N2O’s reinforcing effect [11][12][13][33,34,35], which is the ability of a drug to increase the probability that it will be self-administered again. The nucleus accumbens (NAcc), located in the basal forebrain, is involved in motivation, pleasure and reward. In the NAcc, antagonism of the NMDA (N-methyl-D-aspartate) subtype of glutamate receptors by N2O causes disruption of glutamate homeostasis, which otherwise helps establish and maintain drug-seeking behavior [14][36]. Genetic variability at the receptor level is a potential factor affecting susceptibility to developing N2O dependence [15][37]. N2O is recognized for its anesthetic, analgesic, anxiolytic and anti-depressant effects [1][16][1,42] and the molecular targets of N2O and concomitant regulation of key neurotransmitters (glutamate, opioid, noradrenaline and γ-aminobutyric acid (GABA) will be considered in turn with major neuropharmacological effects (Figure 2).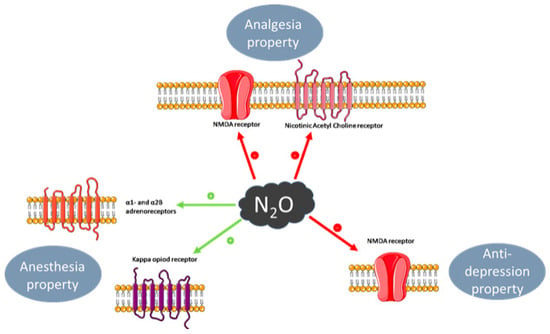
3.2. Anaesthesia
3.3. Analgesia
Analgesia is defined as insensibility to pain without loss of consciousness, and a property of general anesthesia [17][43]. The analgesic and anti-nociceptive effect of N2O involves the opioidergic system, by antagonism of the kappa opioid receptor, and the subsequent regulation of GABAergic and noradrenergic systems. In the periaqueductal grey (PAG) area of the midbrain, which is responsible for modulation of descending pain, blockade of these opioid receptors ablates nitrous-oxide-mediated analgesia, itself also partially reversed by the opioid receptor antagonist naloxone [19][47]. Corticotrophin releasing factor from the hypothalamus is also released in response to N2O [20][48] and causes activation of opiodergic neurons in the PAG with release of endogenous opioids such as dynorphins, which also activate kappa opioid receptors [21][49].3.4. Anxiolytic Effect
Anxiolytics are used to prevent or treat anxiety symptoms or disorders and include the benzodiazepine class of drugs. The anxiolytic effect of N2O involves activation of the gamma-aminobutyric acid type A (GABAA) receptor through its benzodiazepine binding site, though a direct effect is uncertain [22][23][51,52]. However, any such effect is considered minimal compared to the effect on NMDA receptors [24][53].3.5. Anti-depressant Effect
N2O’s purported anti-depressant effect [25][54], which is a comparatively more recent and ongoing area of exploration, is mediated through non-competitive inhibition of NMDA receptors, and is considered analogous to that of ketamine and similarly short-lived [25][26][54,55]. The latter property perhaps hinders its use clinically as an anti-depressant. Other purported molecular targets and effects include the regulation of Brain-derived neurotrophic factor (BDNF) which has a role in synaptic plasticity, synaptogenesis and neurogenesis [27][28][56,57], contributing to its anti-depressant effect, as opposed to neuronal atrophy and synaptic loss, as seen with stress and depression.4. Laboratory Medicine
4.1. Direct N
2
O Measurement
N2O may affect driving behavior and may cause fatal car accidents. As such, detection is an important issue. N2O has a very short half-life of a few minutes [29][58], as the uptake and elimination curves are comparable [30][59]. N2O elimination is mainly pulmonary. When exposure ends, exhaled air concentration declines rapidly, from 66–70% to 6–9% at 5 min and to 2–4% at 30 min during normoventilation. The elimination is slower in cases of hypoventilation [31][60]. Thus, the measurement of N2O in exhaled air is not routinely usable for patients presenting to the emergency department due to the time gap between consumption and admission. The issue is the same for toxicology screening: indeed, for police roadside controls, this appears to be difficult due to the time gap between arrest and sample collection. Additionally, there are technical difficulties concerning N2O measurement in biological fluids. First, gas chromatography–mass spectrometry (GC-MS) can be used, but has limitations, including the challenge of finding an optimal internal standard, the lack of sensitivity and the potential risk of leaks during sampling, extraction and analysis. Headspace-GC-MS, which is a method in which the sample is placed in a hermetically-sealed, gas-tight container, could be promising but need further studies to be used in laboratory medicine [32][61]. Infrared Spectroscopy techniques are sensitive methods to measure N2O in air, but not on biological matrices [33][62].4.2. Impact on Metabolism
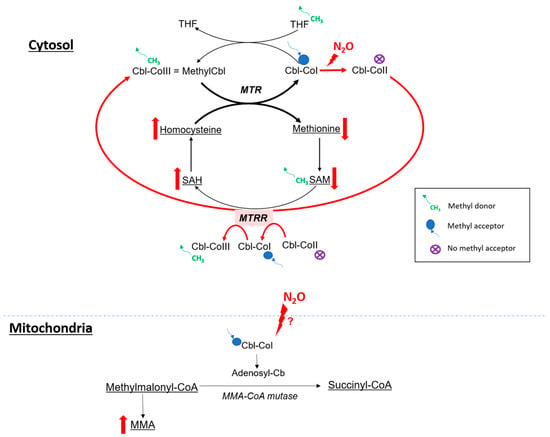
4.2.1. Cobalamin and One Carbon Metabolism
The clinical presentation of N2O intoxication is related to the functional impairment of vitamin B12, also called cobalamin (Figure 3). Indeed, N2O is a powerful oxidant agent: it leads to the oxidation of the cobalt ion of cobalamin(I) [34][63], resulting in the formation of cobalamin(II), unable to accept methyl groups. This results in a decrease in the formation of methylcobalamin, which is a cofactor for methionine synthase (MS or MTR).