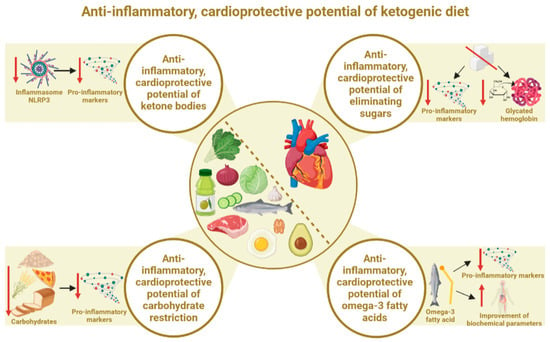
The main ketone body, β-hydroxybutyrate (BHB), exhibits a number of anti-inflammatory properties, including mimicking the fasting state. It has multifaceted effects, including influencing gene expression, reducing inflammation and improving mitochondrial function. This is extremely important given that an integral aspect of cardiovascular diseases is, among others, inflammation. The primary anti-inflammatory effect of BHB is its inhibitory effect on the NLRP3 inflammasome, which is a type of command center for pro-inflammatory cytokines. The fact that it is sensitive to imbalance factors means that its activation may be associated with an increase in inflammatory markers
[16][19]. At the same time, it is known that the NLRP3 inflammasome plays an important role in the heart, as its activation contributes to the deterioration and loss of myocardial function and the pathological development of cardiovascular diseases
[58][59][60][87,88,89].
3.2. Anti-Inflammatory, Cardioprotective Effects of Elimination of Simple Sugars
The ketogenic diet involves limiting the total supply of carbohydrates, most often to a maximum of 50 g per day. In view of this, simple sugars are marginalized and, in fact, can often even be considered to be completely eliminated. This is important to minimize frequent increases in serum glucose and insulin, which inhibit the achievement of the full desired state of ketosis
[16][61][19,99].
It is well known that simple sugars are one of the key pro-inflammatory dietary factors
[62][63][64][100,101,102], which applies mainly to all simple sugars (by the manufacturer, consumer or food preparer). Concerns about the negative effects of simple sugars on CVD date back to the 1960s
[65][103]. At the same time, however, low-fat diets were promoted for the prevention of CVD. Increasing the proportion of carbohydrates (including simple sugars) in the diet consequently led to worsening parameters related to cardiovascular health. It was only decades later that this was proven not to be a useful approach in the fight against increasing heart disease
[66][67][68][69][70][71][104,105,106,107,108,109]. Too much added sugar in the diet can be one of the greatest threats to cardiovascular health. It exacerbates chronic inflammation, increasing the risk of developing CVD
[72][110].
It should be clearly noted that the source of simple sugars often plays an important role. Free sugars are the most pro-inflammatory (including fructose in the form of sugar sweetened beverages (SSB), not necessarily from fruit). Kelly et. al. showed that replacing 5% of the energy from free sugars with non-free sugars was associated with a lower risk of total CVD (0.95; 0.92–0.98;
p-trend = 0.001) and total stroke (0.91; 0.86–0.97;
p-trend = 0.005)
[73][112]. Studies show that the simple sugars present in fruit are unlikely to have a pro-inflammatory effect. A diet rich in fruits and vegetables may even help to reduce inflammation as they are a rich source of antioxidants and other bioactive substances
[74][113]. It is known that a diet with excess fructose is pro-inflammatory, increasing the risk of metabolic syndrome or gout. Elevated levels of fructose metabolites (including uric acid and lactate) are closely related to oxidative stress and local inflammatory reactions in tissues and organs
[75][76][114,115].
Glycated hemoglobin (HbA1c), which reflects the average serum glucose concentration over the past 3 months, is also one of the most important CVD risk factors
[77][119]. Importantly, high HbA1c levels are strongly associated with CVD risk in people both with and without diabetes
[78][79][120,121]. HbA1c has been shown to be positively correlated with CVD, such as carotid and coronary atherosclerosis, ischemic heart disease, ischemic stroke and hypertension, among others. The author of the publication also points out that HbA1c causes dyslipidemia, hyperhomocysteinemia and hypertension. In addition, it increases C-reactive protein (CRP) levels, oxidative stress and blood viscosity. All of these may eventually lead to the development of CVD
[80][122]. It appears that HbA1c is an independent risk factor for the development of CVD and death from these diseases, even in people without diabetes. This shows the remarkable relevance of this marker for the general population
[79][121]. However, the ketogenic diet has been shown to have HbA1c-lowering properties, through which it can also benefit CVD prevention and therapy. The efficacy of KD in lowering HbA1c is supported by a number of meta-analyses and other publications.
3.3. Anti-Inflammatory, Cardioprotective Effects of Total Carbohydrate Restriction
The beneficial above-mentioned effects of ketogenic diets on the values of inflammatory markers and CVD risk factors may also be due to the reduction of the total carbohydrate pool, not simply the elimination of simple sugars. This may be supported by an extensive meta-analysis from 2022, which did not look strictly at the ketogenic diet but precisely at the effect of reducing the percentage of carbohydrates in the diet. It examined the effect of reducing the percentage of energy from carbohydrates from 55–65% to 10% on cardiometabolic risk factors in people with type 2 diabetes mellitus (T2DM). It was shown that each 10% reduction in carbohydrate energy percentage reduced the HbA1c concentration (by an average of 0.20 HbA1c%), fasting blood glucose (by an average of 0.34 mmol/L), triglyceride concentration (by an average of 0.12 mmol), body weight (by an average of 1.44 kg) and even systolic blood pressure (by an average of 1.79 mmHg). These values decreased linearly with a decrease in carbohydrate intake from 55–65% to 10%. These results reflected a 6-month period. When the indices were rechecked 12 months after baseline, HbA1c values continued their linear downward trend (by an average of 0.11 HbA1c%), as did triglyceride levels (a reduction of 0.12 mmol on average)
[81][127]. At the same time, a U-shaped effect was observed at 6 months of follow-up for total and LDL cholesterol, where the greatest benefits occurred when reducing the amount of carbohydrates to 40% of energy, and for body weight at 12 months of observation (greatest benefits at 35% of carbohydrates within total energy).
It should be taken into account that the source of total carbohydrates itself is extremely important. Some studies do not take into account the source, while this certainly influences the subsequent results of the study. It is clear that a diet based on refined carbohydrates will be significantly worse compared to a diet based on unprocessed, whole grain carbohydrate sources. Given these relationships, in addition to achieving a state of ketosis and eliminating simple sugars, the ketogenic diet may also show beneficial anti-inflammatory cardioprotective potential as a result of limiting the total carbohydrate supply, especially if processed carbohydrates are subjected to this restriction.
3.4. Anti-Inflammatory, Cardioprotective Effects of Omega-3 Fatty Acids
A properly composed ketogenic diet is abundant in anti-inflammatory fatty acids from the omega-3 group. In this respect, it may show an advantage over other diets, especially low-fat diets. This is because it is much easier to provide the correct amounts of fatty acids, as one of the main foods is oily fish (which is the main source of omega-3). It is a high-fat diet, so there is much less concern about exceeding the percentage of energy from fats than with other diets.
Omega-3 fatty acids exhibit systemic anti-inflammatory effects, although, in the context of cardiovascular health, they are of particular importance. Indeed, it has been shown that omega-3 PUFAs, by competing with omega-6 PUFAs and displacing arachidonic acid in membrane phospholipids, exert anti-inflammatory properties by reducing the production of pro-inflammatory eicosanoids. Simonetto et al., in a publication, indicated that omega-3 PUFA supplementation may reduce the risk of various phenotypes of atherosclerosis and cardiovascular diseases
[82][134]. A 2023 systematic review indicated and confirmed that omega-3 also improves the blood lipid profile
[83][135]. The cardioprotective effect of omega-3 fatty acids is therefore firmly established in the literature and further confirmed by a number of recent publications, including meta-analyses
[84][85][86][87][88][136,137,138,139,140].
4. Ketone Bodies and Cardiac Energy Metabolism
The influence of the ketogenic diet on cardiac energy metabolism is increasingly being studied and described in scientific publications. This is due to the specific state of ketosis, in which there is increased induction of ketone body production. The main ketone body found in the blood, β-hydroxybutyrate, is seen to have the potential to affect myocardial metabolism and function. Of all the organs, the heart has the highest energy requirement. This is due to the need to work continuously, from fetal life until death. Thus, the cells of the heart muscle (cardiomyocytes) are characterized by the highest concentrations of mitochondria, i.e., “cellular power plants”, in the body. Indeed, mitochondria are the energy centers of the cells, as they are responsible for the production of energy in the form of adenosine triphosphate (ATP)
[89][90][144,145]. It is known that in order to obtain ATP, the heart can use acetyl-coenzyme A (acetyl-CoA) from glucose (via glycolysis) or lipids (via β-oxidation). Under normal conditions, acetyl-CoA from fatty acids is the preferred substrate for ATP production in the heart. However, in patients with HFrEF, the contribution of ketone oxidation to myocardial ATP production increases from 6.4% (in control subjects) to 16.4%
[91][146]. It appears that ketone bodies are therefore a very good, and, in many cases, perhaps better, energy substrate for the acquisition of ATP
[92][93][97,147]. In the early stages of heart disease, the organ shifts its energy preference from fatty acids towards glucose, which is associated with a loss of metabolic flexibility
[94][95][98,148]. However, it is still difficult to determine whether metabolic abnormalities occur due to the onset of heart disease or whether heart disease occurs as a result of metabolic abnormalities
[96][149]. The fact is, however, that this eventually leads to heart failure, resulting in the further reprogramming of the heart’s metabolism towards the uptake and use of ketone bodies as an energy source. The fact that this may be an adaptive response offers a convincing argument for the relevance of ketone bodies to the metabolism of this organ. This is supported by a number of publications that show higher concentrations of ketone bodies and greater uptake of ketone bodies, among others, when heart failure occurs
[97][98][99][100][101][150,151,152,153,154]. The heart prefers ketone bodies to glucose under conditions where both substrates are available. This was shown in a study by Gormsen et al., in which increasing the concentration of ketone bodies to 3.8 mM resulted in a 50% reduction in myocardial glucose uptake. This occurred despite maximal insulin stimulation and sufficient glucose
[102][155]. It appears that the increased oxidation of ketone bodies is of particular use to the heart (and brain), as hyperketonemia does not affect glucose and fatty acid uptake in other organs
[103][104][156,157].
5. The Ketogenic Diet and the Vascular Endothelium
Endothelial cells are extremely important in maintaining the function of the cardiovascular system and, by extension, the whole body. They regulate vascular tone by, among other actions, producing nitric oxide, endothelin and prostaglandins. They produce and respond to various cytokines and adhesion molecules. In addition, they are key immunoreactive cells, and their dysfunction results in a number of pathological changes. In addition, they play an extremely important role in many other processes
[105][106][176,177]. It appears that the ketogenic diet, via ketone bodies, can also affect endothelial cells. These cells are intimately involved in the transport of ketone bodies. Importantly, they are able to take them up and use them to generate biomass and ATP, as they express succinyl-CoA:3-oxoacid-CoA transferase (SCOT) (an enzyme that oxidizes ketone bodies). This was demonstrated in a 2022 publication showing that cardiac endothelial cells are capable of oxidizing ketone bodies, which increases proliferation, cell migration and vascular sprouting. Additionally, in a mouse model of cardiac hypertrophy, the ketogenic diet prevented vasodilation. In view of this, the ketogenic diet may play a beneficial role in heart disease
[107][178]. The publication by Nasser et al. adds further evidence of the protective effect of ketone bodies. Ketone bodies (mainly BHB) in low concentrations (achievable with a ketogenic diet) have been shown to potentially improve endothelial and vascular function in metabolic disease. At the same time, excess ketone bodies resulting from diabetic ketoacidosis have been shown to affect diabetic vasculopathy and the vascular complications of diabetes
[92][97]. However, diabetic ketoacidosis is known to occur with simultaneous excess concentrations of ketone bodies and glucose, with such high levels of ketone bodies not usually achievable through a ketogenic diet
[16][19]. Unsurprisingly, diabetic patients experiencing ketoacidosis are at risk of not only vascular complications but even death from them
[108][109][110][179,180,181].
However, ketone bodies in nutritional ketosis concentrations (induced by a ketogenic diet) exert direct beneficial effects on vascular endothelial modulation, showing anti-inflammatory effects in the endothelium, among others
[92][97]. Gormsen et al. further demonstrated that hyperketonemia induced by Na-3-hydroxybutyrate infusion increased myocardial blood flow by up to 75% and heart rate by approximately 25%. The authors concluded that ketone bodies reduce myocardial glucose uptake and increase myocardial blood flow. They thus suggested that ketone bodies are important vasodilators and an important source of fuel for the heart. This affects the overall therapeutic potential of ketone bodies in CVD
[102][155]. Another randomized controlled trial showed that the infusion of 3-hydroxybutyrate increased the cardiac minute volume by 2 L/min (40%), with an absolute improvement in the left ventricular ejection fraction (8%). Importantly, an effect on vasodilation was noted. This was accompanied by stable systemic and pulmonary pressure
[111][167].
6. The Ketogenic Diet and Blood Pressure
Taking into account the nature of the ketogenic diet, it seems reasonable to consider how this dietary intervention affects blood pressure. Indeed, there are several mechanisms by which it is able to affect this parameter. On the one hand, it is known that the ketogenic diet reduces insulin concentrations because it provides a low amount of carbohydrates
[53][82]. Insulin, on the other hand, is responsible for the retention of sodium in the body by stimulating its reabsorption, and this is also related to the retention of water in the body. With a decrease in insulin concentrations, there is then the increased removal of water and sodium from the body
[112][113][190,191]. This in turn leads to the removal of more of the other electrolytes, e.g., potassium, with the urine
[114][115][192,193]. Magnesium or calcium may also decrease. However, it has been shown that electrolyte loss only occurs during the first period of the ketogenic diet (first week) and is due to natural adaptations to the state of ketosis
[16][116][117][19,194,195]. It is known that adequate electrolyte levels are an essential factor in maintaining normal blood pressure
[118][196]. On the other hand, it is also known that the vascular endothelium has an extremely important influence on blood pressure
[119][120][197,198], which can be affected by the ketogenic diet. In addition, it may beneficially affect the hypothalamic–pituitary–adrenal (HPA) axis and the sympathetic nervous system (SNS)
[121][122][199,200]. Another possible mechanism for the effect on blood pressure may include the effect of the ketogenic diet on the renin–angiotensin–aldosterone (RAA) system, as discussed in two publications from 2023
[123][124][201,202]. Weight loss is a significant, simple mechanism involved in the influence of the ketogenic diet on blood pressure. A caloric deficit used simultaneously with the ketogenic diet, and weight loss itself (and an improvement in body composition), can indirectly improve blood pressure parameters
[125][126][127][203,204,205]. A number of potential mechanisms for the effects of the ketogenic diet on blood pressure make it worthwhile to consider publications examining actual blood pressure changes that have occurred in people using this dietary intervention. The authors of a 2021 publication indicate that the ketogenic diet is able to provide a reduction in blood pressure but does not produce significant changes compared to non-ketogenic diets. They also indicate that this is largely due to weight and fat loss and improvements in CVD risk parameters
[125][126][127][203,204,205].
7. The Ketogenic Diet and Weight Loss as a Factor in CVD Prevention and Therapy
The ketogenic calorie deficit diet is often used to reduce excess body weight. Taking into account its nature, for many people, it is a more effective weight loss strategy compared to standard diets. Taking into consideration that obesity is one of the primary risk factors for CVD, weight loss in itself will significantly reduce the risk of these diseases. Obesity, therefore, simultaneously is the effect of other risk factors, i.e., poor diet and physical inactivity, while at the same time being another risk factor on its own
[2][3][128][129][130][1,6,59,213,214]. In addition, it affects other risk factors, e.g., dyslipidemia, hypertension, type 2 diabetes and sleep disorders, among others. Furthermore, an increased waist circumference can be considered as an independent risk factor for CVD, independent of BMI. Excessive visceral obesity is also an independent indicator and has been linked to poor cardiovascular outcomes. Losing excessive body weight thereby improves cardiovascular function, resulting in a reduction in CVD risk
[131][215].
In addition to these mechanisms, the ketogenic diet improves CVD risk factors and, in addition, often reduces body weight (often the main reason for its use). Thus, it decreases the risk factor of obesity/overweight and, at the same time, nullifies other risk factors that arise from excess body weight. A meta-analysis by Bueno et al. showed that the ketogenic diet may be a more effective option for long-term weight loss (and improvements in some CVD risk factors), compared to low-fat diets
[132][212]. The superiority of ketogenic diets over low-fat diets was also shown in a meta-analysis by Choi et al. It was shown that, compared to low-fat diets, the ketogenic diet was more effective in improving metabolic parameters related to, among other factors, body weight, lipid profile and glycemic control in patients with excess body weight (overweight or obesity), particularly in diabetic patients
[133][125].
8. The Effect of the Ketogenic Diet among Patients with CVD and Healthy People
Some studies often present greater benefits of the ketogenic diet among CVD patients than among healthy and often physically active people. These differences may be due to certain mechanisms. Firstly, people suffering from CVD frequently also have excessive body weight (which is much less common in healthy people), so a greater weight loss effect is observed among people affected by CVD. Additionally, it is known that weight loss alone provides a marked improvement in parameters related to CVD risk
[131][215]. This is shown e.g., in publications by Li et. al, Schiavo et. al. and Michalczyk et. al., in which people using the ketogenic diet lost significantly more body weight compared to the control group, thus improving the values of parameters such as total cholesterol, LDL, HDL and triglycerides
[32][43]. T
his aspect is described in more detail in Section 7.
The other mechanism is the fact that people suffering from CVD have, by definition, an abnormal lipid profile, which is not present to such an extent in healthy and physically active people. An example is a study in which, in healthy, young and trained women, the ketogenic diet did not improve their lipid profiles, and the authors even concluded that it deteriorated
[134][47], which is in opposition to a number of studies described
(in
Section 2.2) in which the ketogenic diet reduced CVD risk parameters among patients with and without overweight. Another argument for the greater benefits of the ketogenic diet among people suffering from or at risk of CVD is the composition of the current diet.
The composition of the diet of these people is often inappropriate, particularly regarding the content of many processed products. A Western-style diet alone worsens CVD risk parameters, thereby increasing the risk of developing the disease. Therefore, the act of switching to an unprocessed diet (which, as a rule, should be a ketogenic diet) should reduce this risk. An example was given in a publication that compared the adoption of an unprocessed ketogenic diet to the continuation of a standard Western model of nutrition (which certainly had a significant impact on the body weight of the surveyed women and dysregulation of the lipid profile, insulin or glucose levels). Women who switched to a ketogenic diet showed significantly improvements in their overall health and CVD risk parameters
[135][50].
9. Conclusions
Summarizing the extensive scientific evidence, the ketogenic diet is a promising nutritional model in the context of cardiovascular disease prevention and therapy. Through its pleiotropic properties, it is able to influence the cardiovascular system on multiple levels. Scientific evidence mostly confirms its beneficial (even more beneficial compared to other diets) effects on the lipid profile and other CVD risk factors. However, there is a lack of strong evidence of the CVD risk from dyslipidemia due to the ketogenic diet. A potential advantage of the ketogenic diet is the strong anti-inflammatory effect that interacts with the cardioprotective properties. In addition, the effect on cardiomyocyte metabolism and the increased uptake of ketone bodies in cardiac disorders means that ketone bodies can be described as “rescue fuel” for the heart. The multifaceted effects of the ketogenic diet may also be confirmed by the effect of ketone bodies on the vascular endothelium, modulating vascular endothelial cells, improving their function or delaying their ageing. This also confirms the beneficial effect of the ketogenic diet on blood pressure values and other indirect CVD risk factors, i.e., reduction in excess body weight. A number of these factors contribute to the overall cardioprotective potential of the ketogenic diet in the prevention and treatment of cardiovascular diseases. This is confirmed by an increasing number of recent scientific studies.