Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Giorgio Ciprandi and Version 2 by Rita Xu.
Respiratory tract infections (RTIs) are usually characterized by mucus hypersecretion. This condition may worsen and prolong symptoms and signs. For this reason, reducing mucus production and improving mucus removal represent relevant aspects of managing patients with RTIs. In this regard, mucoactive drugs may be effective. Mucoactive agents constitute a large class of compounds characterized by different mechanisms of action. Sobrerol is a monoterpene able to fluidify mucus, increase mucociliary clearance, and exert antioxidant activity. Sobrerol is available in various formulations (granules, syrup, nebulized, and suppository). Sobrerol has been on the market for over 50 years.
- mucus
- sobrerol
- mucolytic agent
- respiratory tract infections
1. Background on Respiratory Tract Infections
Respiratory tract infections (RTIs) are widespread diseases and constitute among the most frequent causes of access to primary care doctors, as recently reported by a systematic review including data from 12 countries across five continents [1]. Acute upper RTIs are prevalent and usually recognize a bacterial or viral cause, although viral forms are the most common, as reported in the literature [2]. It has to be underlined that, in clinical practice, the diagnosis is given without a known pathogen. Many viral agents may cause acute upper RTIs, but rhinovirus, coronavirus, syncytial, influenza, parainfluenza, adenovirus, coxsackievirus, echovirus, paramyxovirus, and enterovirus are the most common [3][4][5][6][7][8][3,4,5,6,7,8]. Viral respiratory infections are typically seasonal, such as increased infectivity during cold seasons [9]. Exposure to cold exerts different mechanisms to promote RTIs, including impaired mucociliary clearance, deficient nasal defense, and reduced immune function [10]. Clinically, rwesearchers have to consider that all respiratory viruses may induce an influenza-like illness (ILI), also named flu-like syndrome [11]. Indeed, ILI represents a typical acute viral illness and mimics the clinical features of influenza [12]. ILI is also an acute medical condition characterized by general and respiratory symptoms. In particular, the definition of ILI (common throughout Europe) includes “any person who presents a sudden and rapid onset of at least one of the following general symptoms: fever or feverishness, malaise/exhaustion, headache, myalgia, and at least one of the following respiratory symptoms: cough, sore throat, and wheezing” [13]. However, if milder manifestations occur, the typical common cold has to be considered [14]. Even if AURI may be associated with lower respiratory tract involvement, a healthy and immunocompetent subject usually presents only symptoms concerning the upper respiratory tract.
2. Practical Management
From a clinical point of view, AURI management is generally grounded in a quick treatment that presumes a diagnosis usually based on clinical and epidemiological criteria [15][16]. The most common symptoms include sneezing, rhinorrhea, nasal congestion, hypo/anosmia, hypo/ageusia, facial pressure, sore throat, cough, headache, discomfort, myalgias, and low-grade fever [16][17]. Notably, these symptoms usually last less than ten days, apart from the cough, which tends to last longer [17][18]. The treatment should be timely and appropriate for every single patient. However, if symptoms persist longer or worsen, a trivial common cold may evolve into rhinosinusitis, needing an appropriate work-up [18][19]. As mentioned above, it has to be underlined that the cough may even last for more than a month in some subjects [19][20]. Another aspect that has to be considered is that even if these symptoms are self-resolving, they are still particularly annoying. The parents want to solve them immediately, mainly if a fever is present. Fever often instills fear in parents, even unmotivated fear, so a real fever-phobia is generated [20][21]. Consequently, doctors prescribe symptomatic relievers as a first-line treatment [21][22]. The main goal of treatment is, in fact, the prompt reduction of symptom intensity and duration. It is vital to recommend to patients and parents that antibiotics should not be used unless a bacterial complication occurs [22][23]. Non-steroidal anti-inflammatory drugs (NSAIDs), nasal lavage, and non-pharmacologic remedies are usually sufficient to rapidly cure the most acute viral infections [23][24]. Another aspect that rwesearchers still need to consider has been further emphasized by the recent COVID-19 pandemic [24][25]. RWesearchers should believe that facing an infection is always accompanied by inflammation [25][26]. As a result, inflammation dampening represents a leading therapeutic target in managing infections. The second lesson provided by COVID-19 infection concerns the dramatic outbreak of other RTIs that occurred successively. The explanation of this infections epidemy depends on the restrictive measure (lockdown, mask use, and social distancing) that significantly diminished the incidence of RTIs [26][27]. The paradigmatic example was the negligible prevalence of bronchiolitis during the early COVID-19 pandemic [27][28]. However, since the slackening of restrictive measures, there has been a surge in cases of bronchiolitis that has put a strain on the pediatric hospital network [28][29]. The 2022/2023 seasonal influenza epidemic had an early onset, extraordinary incidence, clinical severity, and persistent duration of the epidemic plateau [29][30].3. The Relevance of Mucus Hyperproduction in Respiratory Tract Infections
The respiratory mucus secretion is a complex mixture produced by different structures, including submucosal glands and secreting epithelial cells (goblet cells and Clara cells) [30][31][33,34]. The submucosal glands are tubular/tubulacinar formations producing mucous, serous, or seromucous secretions. The goblets cells are mucous-secreting cells intercalated in the cylindrical ciliated epithelium lining, disappearing in the terminal bronchioles. The Clara cells are intercalated with the low or cubic cylindrical epithelium, ciliated or not, which extends in a single layer along the peripheral airways. These cells produce both a mucous secretion (like goblet cells) and a lipoprotein secretion (like type B pneumocytes), which can be identified as an alveolar surfactant [32][33][35,36]. The amount of mucus produced depends on the number of mucus-secreting cells present at that level, which in turn is related to the total surface area of the airways; thus, mucus production occurs more in the peripheral airways than in the central airways [34][37]. Physiologically, an adult produces about 10–100 mL of mucus per day, and the amount of mucus that reaches the trachea is approximately 10–20 mL/day [30][31][33,34]. The superficial layer constitutes the ‘sol’ phase of the mucus, very rich in water, about 3 microns thick, and occupies almost the entire length of the cilia of the epithelial cells [35][38]. Above, there is a dense layer: the ‘gel’ phase. It mainly contains glycoproteins (mucins), characterized by a central protein structure anchored to lateral polysaccharide chains formed by sialic acid (sialomucins) or fucose (fucosomucins). In the gel layer, molecules with anti-infective activity exist, such as secretory IgA (S-IgA), lactoferrin, and lysozyme. In addition, it has been hypothesized that a third layer consisting of surfactant exists between the sol and gel layers [31][34]. Usually, only the gel layer is transported, but the sol layer seems essential for mucus transport because it allows the cilia to beat effectively [33][36]. Mucus transport is governed by the mechanical forces of ciliary beating and airflow, counteracted by the friction and inertia of the mucus itself [36][39]. Mucociliary clearance is prevalent in the peripheral airways. Each ciliary cell has about 200 cilia, and the cilia are equipped with ‘claws’ that reach into the gel layer and push it toward the oropharynx [34][35][37,38]. The mucociliary clearance efficacy depends on the airflow velocity, a function of the airway diameter, and the pressure the expiratory muscles create [37][40]. Moreover, in the first years of life, the small airways tend to collapse during normal breathing, and the ciliary machinery develops progressively [38][41].4. Sobrerol
Sobrerol has been on the market in many European countries for over 50 years since its launch in the early 1970s. Sobrerol (5-hydroxy-α, α, 4-trimethyl-3-cyclohexene-1-methanol) is a monocyclic monoterpene with two hydroxyl functions. Various effects characterize it (Figure 1). RWesearchers focused on sobrerol as it is commonly used, and a large body of evidence exists on this compound. However, most studies are old, and researcherswe would propose new possible strategies for their use.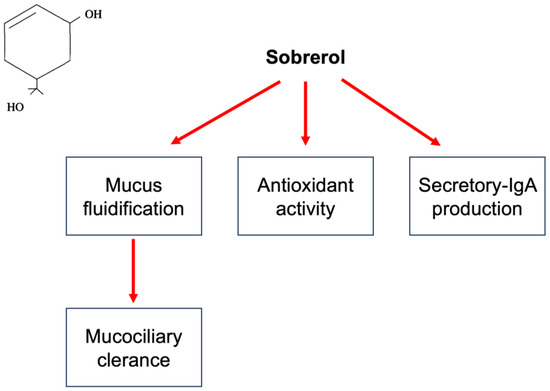
Figure 1. Mechanisms of action of sobrerol. In the left quadrant is reported the chemical molecule. Sobrerol, as schematized, induces mucus fluidification and consequently improves mucociliary clearance, exerts antioxidant activity, and increases sIgA production.