Fernandez-Palomo, C. Microbeam Radiation Therapy (MRT). Encyclopedia. Available online: https://encyclopedia.pub/entry/9699 (accessed on 30 June 2026).
Fernandez-Palomo C. Microbeam Radiation Therapy (MRT). Encyclopedia. Available at: https://encyclopedia.pub/entry/9699. Accessed June 30, 2026.
Microbeam Radiation Therapy (MRT) induces a transient vascular permeability window, which offers a novel drug-delivery system for the preferential accumulation of therapeutic compounds in tumors. MRT is a preclinical cancer treatment modality that spatially fractionates synchrotron X-rays into micrometer-wide planar microbeams which can induce transient vascular permeability, especially in the immature tumor vessels, without compromising vascular perfusion.
Chemotherapy is one of the most suitable treatment options for cancer therapy. However, solid tumors’ anatomical and physiological characteristics limit the exposure of all tumor cells to a sufficient concentration of such therapeutic agents [1][2]. For example, a compound must cross the vascular wall before it can affect the tumor tissue. In particular, the abnormal vasculature and the lack of a functional lymphatic network are tumor characteristics that lead to interstitial hypertension, which minimizes drug diffusion into the tumor core [3][4], ultimately diminishing the therapeutic potential of an anti-cancer compound.
Much work has focused on developing new strategies to overcome this blood-tumor barrier and improve the therapeutic potential of existing agents [5]. These strategies, which involve both pharmacological and physical approaches, include the following:
Modulators of tumor blood flow reduce flow resistance through vasodilation and increase the blood pressure with vasoconstrictors, thereby also increasing the transvascular hydrostatic gradient [6]. Angiotensin II is a clinically proven agent in this group [7];
Vascular normalization describes the correction of structural abnormalities by pruning immature branches, enhancing perivascular coverage, and reinstating the basal membrane [4]. This restores vascular functionality, in particular, the transportation of drugs to the tumor cells. Of all compounds used to achieve vascular normalization [8], VEGF inhibitors have been successful in clinical trials [9];
Vascular permeabilization refers to the increase in capillary permeability due to the administration of inflammatory cytokines and vasomodulators, such as histamine, bradykinin, TNF-alpha, angiotensin II, botulinum neurotoxin and nitric oxide donors amongst others [5]. Some approaches use specific receptor-triggered endocytosis, i.e., employing the insulin-like growth factor 1 receptor to enable trafficking of compounds to the abluminal site [10];
Overcoming the extracellular matrix (ECM) of tumors—extensive collagen networks are major obstacles for the penetration of therapeutic agents [11]. The use of collagen-degrading enzymes [12] or the downregulation of fibroblast activity [13] have shown great effectivity at improving the distribution of macromolecules;
Hyperthermia is a simple, physical method that promotes drug delivery by increasing the local temperature of tissues to a range of 39–42 °C using tools such as microwaves, radiofrequency, and ultrasound. The induced capillary dilation increases perfusion and oxygenation, therefore enhancing the uptake and efficacy of chemotherapeutics [14];
Ultrasound and microbubbles—the use of ultrasound in conjunction with intravenously administered microbubbles disrupts tight junction complexes and improves the delivery of chemotherapeutics in tumors [15][16]. Positive effects have been demonstrated in clinical studies of pancreatic cancer [17];
Sonodynamic therapy is a novel, rapidly developing treatment based on preferential uptake of sonosensitizing compounds in tumor tissues and subsequent activation of the drug by high-intensity focused ultrasound. This strategy is minimally invasive and may be administered to deeply situated tumors [18][19].
Of all the drug-delivery systems mentioned above, more than a dozen have been approved by the Food and Drug Administration agency of the United States; however, most of them are mainly physical or only allow for topical application. This is not surprising since the permeability of the blood vessels is affected by the size and charge of the plasma components, making the delivery of macromolecules even more difficult compared to skin application [19]. As a result, there is a great need for a simple, precise, well-tolerated, and reliable drug delivery system to enhance the therapeutic potential of anti-cancer agents.
Synchrotron Microbeam Radiation Therapy (MRT) could be used as a novel drug delivery strategy that transiently enhances vessel permeability in tumors before drug administration. MRT has a unique vascular disruptive effect, where only the immature vessels are destroyed, while mature microvasculature is preserved [20][21]. MRT is based on the spatial fractionation of synchrotron-generated X-rays into arrays of micron-wide parallel, planar beamlets (25–100 µm), spaced 50–500 µm from center-to-center [22]. This generates a heterogenous dose deposition with tissue in the beam path receiving high (peak) doses of radiation (hGy) and the regions between microbeams (valley) receiving much lower doses (Gy). MRT has shown exceptional tumor control by reducing or even stopping tumor growth [23][24][25][26][27][28][29]. One potential mechanism of action involves MRT’s preferential destruction of the immature dysregulated tumor vasculature, which decreases tumor blood volume, leading to necrosis [23][30]. Remarkably, normal tissues show extremely high tolerance to MRT, as has been observed in the brains of rodents [26][31][32][33], piglets [34], duck embryos [35], cerebella of suckling rat pups [36][37], weanling piglets [34][36], and in different types of normal tissues of mice after partial or total body MRT irradiation [38][39] (recently reviewed in [22]). This normal tissue sparing effect has been attributed to the preservation of mature microvasculature. Due to the spatial fractionation of MRT, vascular damage is confined to the beam path and, unlike the tumor, the minimally irradiated endothelial cells in the valley region can repair neighboring regions damaged by the microbeam [33]. The unique vascular disruptive effects of MRT have been demonstrated in the Chick Chorioallantoic Membrane (CAM) where the vascular properties resemble those of tumors [20]. The CAMs were exposed to peak doses of 200–300 Gy, which preferentially destroyed immature vessels (with the first subcellular changes occurring 15 min after exposure) while vascular integrity was maintained in the valley regions. This promoted the resolution of damaged regions and subsequent clearance of edema one hour post-irradiation with sustained capillary perfusion. Perfusion studies 6 h following MRT with FITC-dextran showed zones of intact, perfused capillaries in the valley (low-dose) region and vascular disruption and loss of perfusion limited to the microbeam path (high-dose) [20]. The reversible damage to the vasculature is attributable to the spatial fractionation of the incident beam, as homogenous dose delivery resulted in unresolved damage at doses hundreds of Gy below those delivered by MRT. The induction and subsequent resolution of edema suggest that MRT induces a transient increase in vascular permeability following MRT that could be exploited for therapeutic gain.
2. Microbeams Induced a Transient Vascular “Permeability Window” in CAM without Impairing Tissue Perfusion
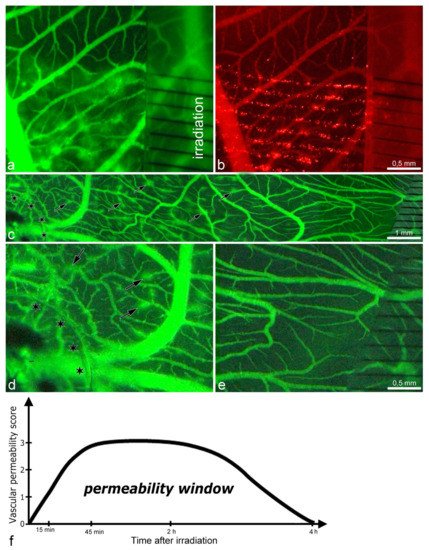
After irradiating the CAM with microbeam entrance peak-doses of 75 Gy, there was an increase in transpermeability without vascular destruction and preservation of vascular perfusion. The vascular permeability assay revealed that only FITC-dextran (~27 nm) extravasated into the surrounding tissue, while the larger microspheres (100 nm) remained stuck along the microbeam paths (Figure 1a,b). Successive semi-quantitative evaluation (every 15 min) showed that the extravasation of FITC-dextran was transient, detected from 15 min until it ended at 4 h after irradiation (Figure 1f, Video below).
In addition, we administered VEGF to the top of the CAM prior to irradiation to induce neovascularization. The goal was to simulate the tumor microenvironment, which normally has high amounts of VEGF. Then, we compared the vascular effects caused by MRT in the VEGF-treated (Figure 1c, left side) and non-treated areas (Figure 1c, right side). We found that the vascular transpermeability occurred earlier (10 min after irradiation) in the VEGF-induced neovasculature (higher magnification in Figure 1d) than in the VEGF-untreated vasculature (higher magnification in Figure 1e). This suggests that immature vessels are more sensitive to the microbeams and show an earlier onset of vascular transpermeability.
Figure 1. Images from intravital microscopy showing increased vascular permeability in CAM after exposure to MRT peak doses of 75 Gy; (a,b): normal CAM vasculature; (c–e): vasculature after VEGF treatment. Note: (a) forty-five minutes after exposure to MRT, the vascular permeability is increased, as demonstrated by the extravasation of FITC-dextran (green-fluorescent halos around the blood vessels). Conversely, in (b), the microspheres did not diffuse into the surrounding tissue but remained affixed as red-fluorescent dots along the microbeams path. Left side: (c) at the site of VEGF application (asterisks indicate the edge of the Thermanox® coverslip), the vascular permeability increased as early as 10 min after MRT, as shown by the halos of extravasated FITC-dextran (some marked by arrows). Right side: in the non-treated zone, no such signs of increased vascular permeability were observed simultaneously. Images (d,e): parts of (c) at higher magnification. Image (f): schematic representation of the vascular permeability window after 75 Gy of MRT. The score: (0) = no FITC extravasation; (1) = small non-confluent FITC “halo” surrounding the capillaries; (2) = FITC “halos” start merging but they are not completely confluent; (3) = the “halos” are completely confluent. In (a–e), black stripes on the radiochromic film indicate the path of the microbeams.
Supplementary Video: Vascular Permeability in CAM.
3. Time Course of the Structural Changes in the CAM during the Vascular “Permeability Window”
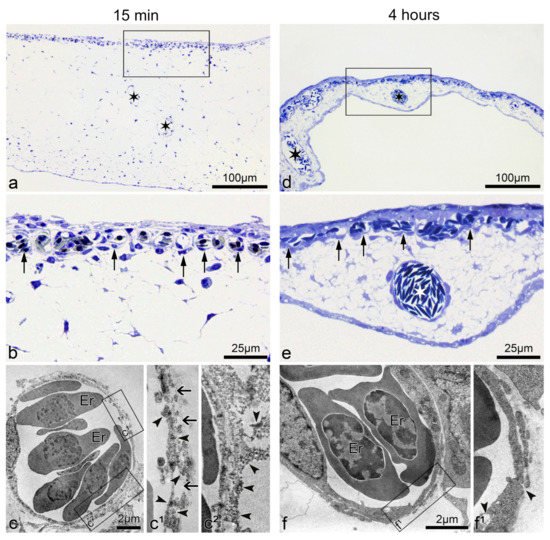
Fifteen minutes after microbeam radiation of 75 Gy, the CAM thickness increased transiently to approximately three times its regular size. This was assessed by comparing it against the recovered CAM 4 h post-irradiation (Figure 2a,d). The acute increase in size is likely attributed to the development of edema underneath the capillary plexus (Figure 2b). The ultrastructural analysis revealed a discontinuous luminal surface of the microvessels, with rarefication of the endothelial cytoplasm resulting in fissures and gaps. The increased permeability was evidenced by the presence of FITC-dextran dots in the endothelial cell wall of the microvessels, as well as in the extravascular space (Figure 2c(c1,c2)). Conversely, 4 h after irradiation, the endothelial cells showed restored integrity, which was accompanied by only single holes and solitary FITC-dextran depositions in the endothelium (Figure 2f(f1)). These observations suggest that microbeams of 75 Gy increased the vascular transpermeability without long-lasting damage to CAM vasculature.
Figure 2. Morphological alteration of CAM vasculature 15 min and 4 h post-75 Gy of MRT. Images (a,b): semithin section of CAM fifteen minutes after MRT exposure: Irradiated CAM is enlarged (edematous). The capillary vessels (arrows) appear almost normal at light microscopy. (c(c1,c2)): Ultrastructure of CAM samples shown in (a,b) reveal a discontinuous endothelium with gaps and fissures (arrows). Those are most likely responsible for the increased permeability, as demonstrated by the presence of FITC-dextran dots (arrowheads) in the endothelial cell wall (c1) as well as in the abluminal space (c2). Images (d,e): four hours after 75 Gy of MRT, the CAM thickness decreased, thus almost reverting to the normal morphology. The capillary plexus (arrows) and supplying vessels (white asterisk) appear perfused and intact in semithin sections. Images (f(f1)): four hours after microbeam exposure, the capillaries regained their normal ultrastructure, as evidenced by the nearly normal endothelial cells. Only occasional vacuoles and fissures were present (arrowheads). Images (b,c1,c2,e,f1) are higher magnifications of the rectangles in (a,c,d,f), respectively. Er = erythrocyte.
4. Microbeams also Induced Vascular Permeability in Human U-87 Glioblastoma Xenografts
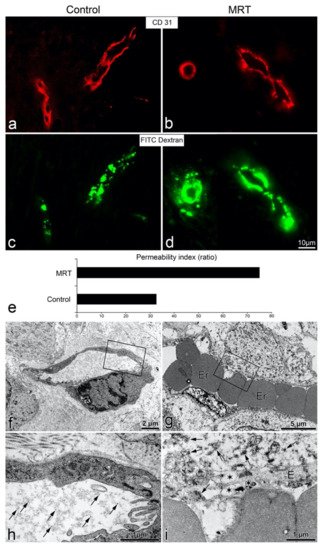
To determine whether microbeams promote vascular permeability in a human glioblastoma xenograft mouse model, we compared one group treated with 150 Gy (peak-entry dose) of microbeams with an unirradiated tumor control group (Figure 3). We observed clear extravasation of FITC-dextran in the irradiated tumors 45 min post-irradiation (Figure 3d). Conversely, the fluorescent compound remained intravascular in the control group (Figure 3c). The permeability index revealed a two-fold increase in transpermeability following MRT relative to the unirradiated control (Figure 3e). At the ultrastructural level, no extravasation of the fluorescent probe was observed in control tumors; FITC-dextran dots remained in the lumen (Figure 3f,h). However, in microbeam-treated tumors, FITC-dextran was observed in the extravascular space together with partially disintegrated endothelial cells (Figure 3g,i). These results confirm that MRT can also induce vascular permeability in this mammalian tumor model, and thus, vascular permeability is not restricted to the CAM (avian).
Figure 3. MRT-induced vascular permeability in mice harbouring the human U-87 glioblastoma xenograft. Fluorescence microscopy for CD31 and FITC-dextran in a control tumor (a,c); tumor post-MRT (b,d). There was no extravasation of the green FITC-dextran in the control tumor (c), while in the MRT-treated tumor (d), 45 min after 150 Gy, a bright halo of green fluorescence was visible. Image (e): graph showing the quantification of the vascular permeability in controls and MRT-treated tumors as the ratio of extravasated FITC-dextran fluorescent area/vessel area. The ultrastructure of tumor vessels was normal in controls (f,h), with no extravasation of FITC-dextran (intraluminal dextran as dark dots indicated by arrows). Conversely, in treated tumors (g,i), an extravasated fluorescent probe material was observed as dark dots (arrows) in the extravascular space; the disrupted endothelium contained multiple vacuoles of different sizes, indicated by asterisks. Er = erythrocyte. Images (h,i) are higher magnifications of the rectangles in (f,g), respectively.
5. Using the MRT-Induced Vascular Permeability to Enhance the Delivery of Cisplatin
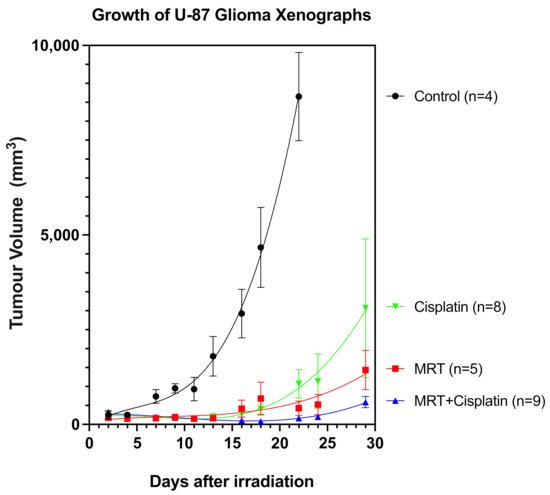
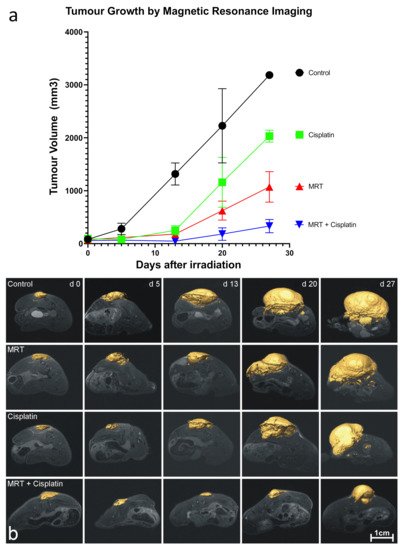
To exploit the MRT-induced “permeability window”, the adjuvant Cisplatin was administered in conjunction with MRT in mice bearing glioblastoma xenografts. Cisplatin is known to have efficacy against glioblastoma in vitro but a poor clinical response as a single agent and in combination with radiotherapy [54]. This is primarily due to poor penetration across the blood–brain barrier [55] and dose-limiting cytotoxicity [56]. Microbeam radiation therapy was delivered to the tumors 17 days after cell inoculation, and Cisplatin was administered 40 min after irradiation. Tumors in the control group began to grow exponentially 2 days after treatment (Figure 4). Differences between the treatment groups started on day 13, with the fastest-growing tumors belonging to the Cisplatin group, followed by those treated with MRT alone. In contrast, tumors treated with the combination of MRT + Cisplatin remained unchanged until approximately 22 days after treatment, when their growth rate began to abate slowly. In a second experimental trial, tumor growth measurements performed with Magnetic Resonance Imaging (MRI) on days 0, 5, 13, 20 and 27 after treatment yielded tumor volumes comparable to those measured with the digital caliper; tumor volumes decreased in the same order: Control > Cisplatin alone > MRT alone > MRT + Cisplatin (Figure 5a). Accordingly, images of tumor progression (Figure 5b) show the best treatment results on animals subjected to MRT + Cisplatin in comparison with the other experimental groups; with a 2.75-fold decrease in comparison with MRT alone, and a 5.25-fold decrease compared to Cisplatin alone. These results show that the administration of adjuvant Cisplatin can take advantage of the MRT-induced vascular permeability.
Figure 4. Growth of U-87 glioblastoma xenograft. Groups are unirradiated Controls (n = 4), Cisplatin (n = 8), MRT (n = 5), and Double Treatment (MRT + Cis) (n = 9). The tumors were measured with a digital caliper every second day.
Figure 5. U-87 glioblastoma growth followed by MRI. Image (a) shows the tumor volume growth measured by MRI. Image (b): MRI images of the tumor progression for each animal group. Control (n = 3), Cisplatin (n = 4), 150 Gy MRT (n = 7), and Double Treatment (150 Gy MRT + Cis) (n = 5).
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
 +1 credit
+1 credit