 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Antonio Maria Labate | -- | 1906 | 2026-06-06 22:28:53 | | | |
| 2 | Catherine Yang | -114 word(s) | 1792 | 2026-06-08 03:41:04 | | |
Video Upload Options
Liver–kidney–vascular crosstalk describes the clinical interaction between metabolic dysfunction-associated steatotic liver disease, diabetic kidney disease, and cardiovascular disease in type 2 diabetes. These conditions share common drivers, including insulin resistance, visceral adiposity, chronic low-grade inflammation, endothelial dysfunction, and atherogenic dyslipidemia. Recognizing this integrated network may improve residual cardiometabolic risk stratification and support a more comprehensive approach to prevention and treatment.
1. Introduction
Type 2 diabetes is a systemic cardiometabolic disease associated with increased risk of cardiovascular disease, chronic kidney disease, heart failure, hepatic metabolic dysfunction, and premature mortality. Major advances in glucose-lowering therapy, lipid management, blood pressure control, weight reduction, and organ-protective strategies have improved outcomes, but a substantial proportion of patients continue to experience adverse events despite apparently adequate control of conventional targets [1][2][3][4][5].
This persistent burden is commonly described as cardiometabolic residual risk. In clinical practice, residual risk is often interpreted as the difference between observed risk and the risk expected after correction of individual factors such as glycated hemoglobin, low-density lipoprotein cholesterol, blood pressure, body weight, albuminuria, or estimated glomerular filtration rate (eGFR). However, this target-centered view may underestimate the biological and clinical complexity of T2D [1][2][3][4][5][6][7][8][9][10][11][12].
A broader pathway-centered model considers T2D as a disorder of interacting organs and risk domains. In this model, MASLD, DKD, and vascular disease are not isolated complications, but mutually reinforcing expressions of a shared metabolic environment. The liver–kidney–vascular axis offers a practical clinical framework for interpreting persistent vulnerability, identifying high-risk phenotypes, and selecting therapies that may modify multiple components of cardiometabolic risk [1][6][7][8][9][10][11][12][13][14][15].
2. Clinical Meaning of Liver–Kidney–Vascular Crosstalk
The liver, kidney, and vascular system are increasingly recognized as components of a single cardiometabolic continuum. People with T2D frequently exhibit combinations of hepatic steatosis, albuminuria, eGFR decline, endothelial dysfunction, atherosclerosis, heart failure, obesity, hypertension, and dyslipidemia. These abnormalities share upstream drivers such as insulin resistance, visceral adiposity, chronic low-grade inflammation, and abnormal lipid handling.
The clinical relevance of crosstalk lies in mutual amplification. MASLD may identify a phenotype with higher systemic metabolic burden, greater dyslipidemia, increased inflammatory activation, and higher cardiovascular risk. DKD, even at early stages, is associated with vascular dysfunction, blood pressure dysregulation, heart failure risk, and adverse cardiovascular outcomes. Vascular disease, in turn, worsens renal perfusion, contributes to microvascular injury, and reflects cumulative exposure to metabolic and inflammatory stress.
Consequently, an organ-by-organ approach may miss the integrated nature of risk. A patient with T2D, hepatic steatosis, elevated triglycerides, albuminuria, and arterial disease should not be considered as having several unrelated comorbidities, but as expressing a coherent liver–kidney–vascular phenotype of residual cardiometabolic risk.
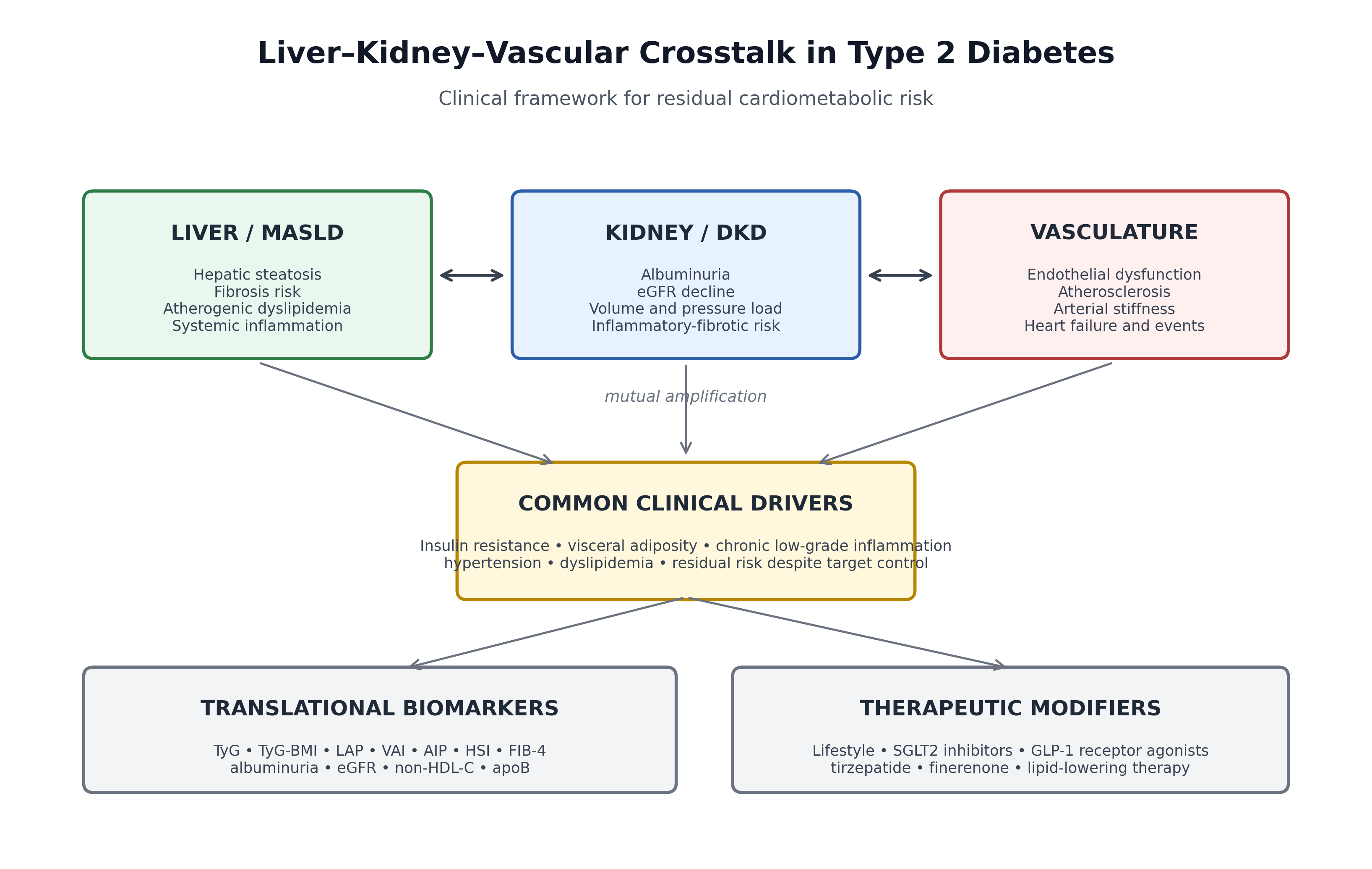
Figure 1. Clinical model of liver–kidney–vascular crosstalk in type 2 diabetes. MASLD, DKD, and vascular disease represent interconnected expressions of residual cardiometabolic risk. Simple biomarkers and contemporary therapeutic strategies may help identify and modify this network.
3. MASLD and Cardiometabolic Risk
MASLD is one of the most common chronic liver diseases in people with T2D and is strongly associated with obesity, insulin resistance, dyslipidemia, hypertension, chronic kidney disease, and cardiovascular outcomes [6][7][8][9][10]. The transition from the older NAFLD terminology to MASLD emphasizes the metabolic basis of the disease and its close relationship with cardiometabolic risk factors [7].
From a clinical perspective, MASLD should not be viewed only as a hepatic condition. It often identifies patients with increased visceral adiposity, impaired insulin sensitivity, triglyceride-rich lipoprotein excess, and a higher burden of cardiometabolic complications. Importantly, the severity of liver disease, particularly fibrosis, appears to be more strongly associated with adverse outcomes than the mere presence of steatosis [6][8][10][15].
The association between MASLD and cardiovascular disease extends beyond shared risk factors. Patients with MASLD have higher rates of atherosclerotic cardiovascular disease, and cardiovascular events remain a leading cause of death in this population. In T2D, the coexistence of MASLD may therefore signal a broader residual-risk phenotype requiring integrated assessment of liver, kidney, and vascular health.
Emerging pharmacological data also reinforce the clinical connection between liver disease and cardiometabolic risk. GLP-1 receptor agonists and dual incretin therapies have shown beneficial effects on weight, glycemic control, and liver-related outcomes, while SGLT2 inhibitors may improve metabolic and cardiorenal parameters. These observations support the concept that liver involvement is a modifiable component of systemic cardiometabolic disease.
4. Diabetic Kidney Disease and Vascular Risk
DKD is a major determinant of morbidity and mortality in people with T2D. Albuminuria and eGFR are not only renal markers; they are also powerful indicators of systemic vascular risk and adverse cardiovascular outcomes.
Albuminuria reflects a complex phenotype that includes glomerular endothelial dysfunction, podocyte injury, tubular stress, and microvascular damage. Even moderately increased albuminuria is associated with higher risk of cardiovascular events, heart failure, CKD progression, and mortality. Likewise, reduction in eGFR identifies a phenotype with greater vulnerability to volume overload, hypertension, vascular calcification, inflammation, and cardiac dysfunction.
The bidirectional relationship between kidney and vascular disease is clinically important. Renal dysfunction contributes to hypertension, sodium retention, neurohormonal activation, systemic inflammation, and heart failure risk. Conversely, vascular disease and endothelial dysfunction promote renal hypoperfusion and microvascular injury. This reciprocal relationship makes kidney assessment central to cardiometabolic risk stratification in T2D [1][2][5][10].
The clinical validation of SGLT2 inhibitors and finerenone has strengthened the kidney–vascular paradigm. SGLT2 inhibitors reduce CKD progression and heart failure events across broad patient populations, while finerenone reduces kidney and cardiovascular outcomes in people with T2D and CKD. These therapies demonstrate that targeting the renal component of the network can translate into cardiovascular protection.
5. Vascular Dysfunction as the Common Clinical Pathway
Cardiovascular disease remains the leading cause of death among individuals with T2D. The vascular system represents the final common pathway through which metabolic, hepatic, renal, inflammatory, and lipid-related abnormalities translate into clinical events.
Endothelial dysfunction, arterial stiffness, atherogenic dyslipidemia, coronary and peripheral atherosclerosis, microvascular disease, and thrombotic tendency all contribute to residual cardiovascular risk. These abnormalities may persist even when HbA1c, LDL cholesterol, and blood pressure are near target, which explains why isolated risk-factor control may be insufficient in a subset of patients.
The vascular dimension also connects macrovascular and microvascular complications. Albuminuria, retinopathy, neuropathy, coronary disease, peripheral artery disease, and heart failure frequently cluster in high-risk patients, reflecting shared vascular vulnerability. In this context, MASLD and DKD may be interpreted as organ-specific windows into systemic cardiometabolic vascular injury.
6. Clinical Biomarkers of Organ Crosstalk
Because the liver–kidney–vascular network is complex, clinically accessible biomarkers and composite indices may help identify residual-risk phenotypes. These tools do not replace dedicated organ assessment, but they provide practical signals of insulin resistance, visceral adiposity, hepatic involvement, lipid-related vascular risk, and renal-microvascular damage.
Table 1. Practical clinical markers of liver–kidney–vascular crosstalk.
|
Domain |
Markers |
Clinical interpretation |
Main limitations |
|
Insulin resistance / adiposity |
TyG, TyG-BMI, LAP, VAI, waist circumference, BMI |
Approximate metabolic burden, visceral adiposity, and insulin-resistant phenotype. |
Indirect; influenced by fasting status, medications, and anthropometry. |
|
Lipid-related vascular risk |
Triglycerides, HDL-C, non-HDL-C, apoB, AIP |
Identify atherogenic dyslipidemia, remnant-related risk, and residual lipid burden. |
AIP and related indices are supportive, not definitive risk scores. |
|
Liver involvement |
ALT/AST/GGT, HSI, FIB-4, imaging, elastography |
Screen for steatosis and fibrosis-related risk in MASLD. |
Blood-based scores require confirmation when abnormal or indeterminate. |
|
Kidney / microvascular injury |
Albuminuria, ACR, eGFR, eGFR trajectory |
Capture renal dysfunction and systemic microvascular risk. |
Must be interpreted with age, acute illness, and repeated measurements. |
The TyG index and TyG-derived indices combine fasting glucose, triglycerides, and anthropometric measures, providing low-cost surrogates of insulin resistance and metabolic burden. LAP and VAI integrate anthropometric and lipid variables and may reflect visceral adiposity and adipose-lipid dysfunction. AIP, non-HDL cholesterol, and apoB help characterize lipid-related vascular risk beyond LDL cholesterol alone.
Liver-related indices such as HSI and FIB-4 may identify probable steatosis and fibrosis-related risk, while albuminuria and eGFR remain essential markers of renal and systemic microvascular damage. The value of these indices is greatest when they are interpreted together, rather than as isolated measurements.
7. Therapeutic Implications
Recognition of liver–kidney–vascular crosstalk has important therapeutic implications. Treatment should not focus exclusively on glycemic targets, but should address weight, blood pressure, lipids, renal protection, liver-related metabolic dysfunction, and global cardiovascular risk [1][2][3][4][5][6][9][10].
7.1. Lifestyle Intervention
Weight reduction, structured physical activity, smoking cessation, dietary quality, and improvement in cardiorespiratory fitness remain foundational. Lifestyle intervention can simultaneously improve insulin sensitivity, visceral adiposity, hepatic fat, blood pressure, lipid profile, inflammation, and endothelial function.
7.2. SGLT2 Inhibitors
SGLT2 inhibitors have demonstrated major benefits on CKD progression, heart failure hospitalization, and cardiovascular outcomes in people with and without diabetes. Their role extends beyond glucose lowering and directly supports the concept of cardiorenal protection within the liver–kidney–vascular network.
7.3. GLP-1 Receptor Agonists and Dual Incretin Therapies
GLP-1 receptor agonists reduce body weight, improve glycemic control, and decrease cardiovascular events in high-risk patients. Semaglutide and tirzepatide have also shown clinically relevant effects on metabolic liver disease, supporting their role in patients with combined adipose-liver-cardiovascular risk.
7.4. Kidney-Protective and Antifibrotic Strategies
Optimized renin–angiotensin system blockade remains central in patients with albuminuria and hypertension. Finerenone provides additional kidney and cardiovascular protection in patients with T2D and CKD, highlighting the relevance of inflammatory-fibrotic risk in the kidney–vascular axis.
7.5. Lipid-Lowering Therapy
Aggressive management of atherogenic dyslipidemia remains essential. Statins, ezetimibe, PCSK9-targeted therapies, and selected triglyceride-focused strategies may reduce lipid-related residual risk, particularly in patients with insulin resistance, MASLD, elevated triglycerides, low HDL cholesterol, or high apoB/non-HDL cholesterol [2][3].
8. Future Perspectives
Future cardiometabolic care is likely to move from isolated target-based management toward integrated phenotyping. The goal will not be only to estimate whether a patient is at high risk, but to understand why that risk persists.
Near-term clinical strategies may combine simple biomarkers such as TyG-derived indices, adiposity measures, FIB-4, HSI, albuminuria, eGFR, non-HDL cholesterol, apoB, and inflammatory markers when available. Imaging-based liver and vascular assessment may further refine risk stratification in selected patients.
Artificial intelligence and machine-learning approaches may help integrate electronic health records, laboratory data, imaging, continuous glucose monitoring, and outcomes data. Their potential value lies not only in risk prediction, but in identifying dominant clinical phenotypes such as adipose-liver, kidney-vascular, lipid-inflammatory, or mixed residual-risk patterns. These tools will require external validation, interpretability, and clinically meaningful implementation before routine adoption.
9. Conclusions
The traditional view of diabetic complications as isolated organ-specific disorders is progressively being replaced by an integrated cardiometabolic model. MASLD, DKD, and cardiovascular disease often represent interconnected manifestations of a common pathological process driven by metabolic dysfunction, insulin resistance, adiposity, inflammation, dyslipidemia, and vascular injury.
Recognition of liver–kidney–vascular crosstalk may improve clinical interpretation of residual risk, support earlier identification of vulnerable phenotypes, and guide more comprehensive therapeutic strategies. In people with T2D, reducing long-term complications will require moving beyond isolated target control toward integrated cardiometabolic prevention.
References
- Labate AM, Cimino E, Giacomelli L, Ettori S, Oladeji OA, Agosti B. Molecular Pathways of Cardiometabolic Residual Risk in Type 2 Diabetes: Insulin Resistance, Metaflammation, and Liver–Kidney–Vascular Crosstalk. Preprints. 2026. doi:10.20944/preprints202606.0057.v1.
- Ndumele CE, Rangaswami J, Chow SL, et al. Cardiovascular-Kidney-Metabolic Health: A Presidential Advisory From the American Heart Association. Circulation. 2023;148:1606–1635.
- Marx N, Federici M, Schütt K, et al. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes. Eur Heart J. 2023;44:4043–4140.
- American Diabetes Association. Cardiovascular Disease and Risk Management: Standards of Care in Diabetes—2026. Diabetes Care. 2026;49(Suppl 1).
- American Diabetes Association. Chronic Kidney Disease and Risk Management: Standards of Care in Diabetes—2026. Diabetes Care. 2026;49(Suppl 1).
- KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024;105(Suppl):S117–S314.7. EASL–EASD–EASO Clinical Practice Guidelines on the management of MASLD. Diabetologia. 2024;67:1712–1742.
- EASL–EASD–EASO Clinical Practice Guidelines on the management of MASLD. Diabetologia. 2024;67:1712–1742.
- Rinella ME, et al. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. Hepatology. 2023;78:1966–1986.
- Mantovani A, Byrne CD, Bonora E, Targher G. Nonalcoholic fatty liver disease and risk of incident cardiovascular disease. Lancet Gastroenterol Hepatol. 2021;6:903–913.
- The EMPA-KIDNEY Collaborative Group. Empagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2023;388:117–127.
- Perkovic V, Tuttle KR, Rossing P, et al. Effects of Semaglutide on Chronic Kidney Disease in Patients with Type 2 Diabetes. N Engl J Med. 2024.
- Sanyal AJ, et al. Tirzepatide for Metabolic Dysfunction–Associated Steatohepatitis with Liver Fibrosis. N Engl J Med. 2024.
- Heerspink HJL, et al. Dapagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2020;383:1436–1446.
- Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N Engl J Med. 2019;380:2295–2306.
- Bakris GL, Agarwal R, Anker SD, et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes. N Engl J Med. 2020;383:2219–2229.

