 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Sidney Ley | -- | 3746 | 2024-06-13 01:54:25 | | | |
| 2 | Jason Zhu | -177 word(s) | 3569 | 2024-06-13 03:16:35 | | | | |
| 3 | Catherine Yang | Meta information modification | 3569 | 2024-10-31 01:55:06 | | |
Video Upload Options
Influenza viruses cause acute respiratory infections responsible for significant mortality and morbidity around the world. Various factors, such as antigenic drift, allow influenza strains to avoid being fully suppressed by seasonal vaccines. This has led to the increased scrutiny of antivirals as treatment and prophylaxis options for seasonal outbreaks and potential pandemics. Unfortunately, many influenza antivirals suffer from a lack of adequate clinical trials, as well as a lack of toxicity data. This is especially true of umifenovir (arbidol), a drug popularly used for the prevention and treatment of influenza strains in China and Russia. Neuraminidase inhibitors, though widely prescribed, display a potential for future resistance. Adamantanes, while proven to be effective in treating influenza A, are already encountering rapid and widespread cross-resistance and are effectively obsolete. Baloxavir marboxil, a newer antiviral, shows promise in treating acute uncomplicated influenza and may avoid the development of resistance when co-administered with other antiviral drugs. Indeed, the low genetic barrier to resistance associated with influenza antivirals could potentially be overcome by co-administration with other antivirals.
1. Introduction
Influenza viruses belong to the Orthomyxoviridae family. Among these, influenza A, B, and C, are known to infect human hosts and cause acute respiratory infections [1]. Influenza A is prone to antigenic variation and is capable of interspecies transmission. Moreover, this variant is often the cause of major flu pandemics [2][3][4]. Influenza viruses have the glycoproteins hemagglutinin (HA) and neuraminidase (NA) on their surface, as well as Matrix-2 (M2) proton channels (Figure 1). The presence of HA and NA gives influenza viruses their ability to adapt to and evade host immune responses, which necessitates the invention of new preventative vaccines each flu season.
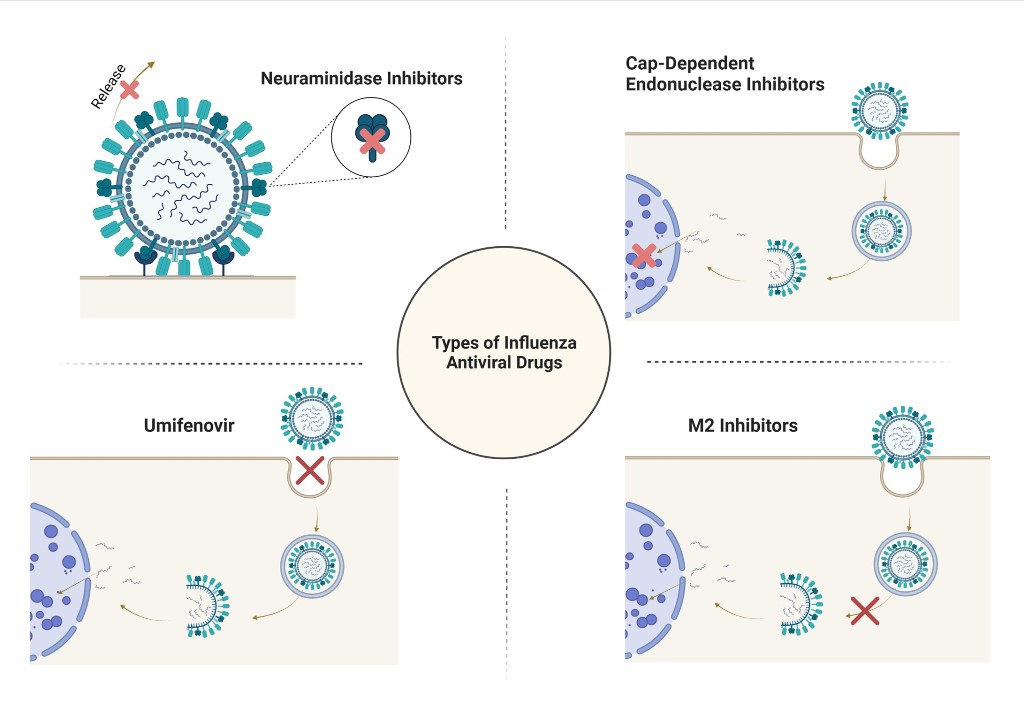
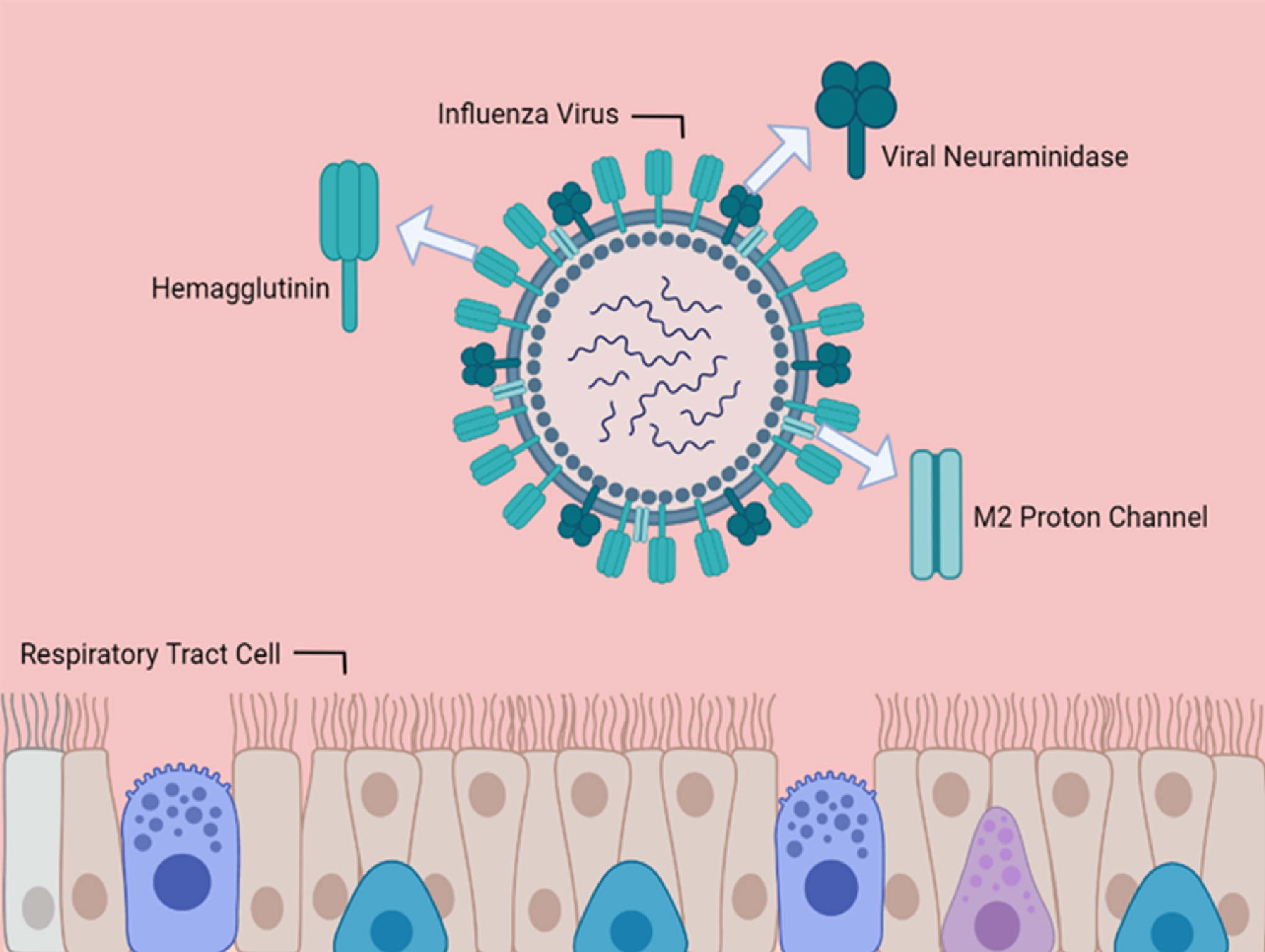
Figure 1. Structure of an Influenza Virus. The prominent viral coat structures are emphasized, including the two glycoproteins hemagglutinin and neuraminidase. The M2 proton channel is also displayed. Near the bottom of the figure is the surface of the respiratory tract. Made with BioRender.com.
A viral life cycle is composed of five (5) stages: viral entry, viral uncoating, viral replication, assembly and budding, and viral release from the host cell [5]. HA is a sialic acid receptor-binding molecule that mediates the entry of the influenza virus into the target cell and is, therefore, the main target for a host body’s neutralizing enzymes [6]. NA enzymes are then responsible for cleaving the glycosidic linkages of viral neuraminic acids, which allows the release of these new influenza particles to spread throughout the infected organism [7]. These unique surface proteins, as well as each viral life stage, provide influenza antivirals with different targets for therapeutic action.
2. Umifenovir
Umifenovir (Arbidol) is a broad-spectrum antiviral that acts against viral HA, specifically [10]. Developed in the 1970s by the collaborative efforts of the Chemical–Pharmaceutical Scientific Research Institute of Russia, the Scientific Research Institute of Medical Radiology in Obninsk, and the Leningrad-Pasteur Scientific Research Institute for Epidemiology and Microbiology, Umifenovir is currently approved only in Russia and China for the treatment of influenza A and B, prophylaxis, and post-influenza complications[11][12][13], though it does exhibit anti-influenza C activity as well [10]. Umifenovir is a controversial drug; due to a lack of reproducible lab results [14] and limited toxicity data outside of Russia, it has yet to gain global use and remains unapproved for influenza treatment in many countries. Information on umifenovir is difficult to find in the West, largely due to the language barrier, as key information including early clinical trial designs and results is often available only in Russian [15]. There are, however, many Russian reports describing umifenovir’s anti-influenza activity against various strains, such as influenza A (H5N1) and the 2009 A (H1N1) variant [15][16][17].
Umifenovir is considered an inhibitor of various enveloped and non-enveloped RNA viruses based on its insertion into membrane lipids, leading to the inhibition of membrane fusion between virus particles and plasma membranes, as well as interfering with the fusion between virus particles and the membranes of endosomes (Figure 2) [10][14][18]. In influenza strains, umifenovir interacts with HA, causing an increase in HA stability and preventing its transition into the fusing state [19][20][21]. Umifenovir may also be immunomodulatory, which would allow it to interfere with induction and macrophage activation[11]. Umifenovir shows antioxidant activity, which presumably counteracts virus activity [22]. As this drug is not well known outside of Russia and China, this section examines the recent and notable in vitro, in vivo, and clinical studies about umifenovir’s efficacy as an influenza treatment.
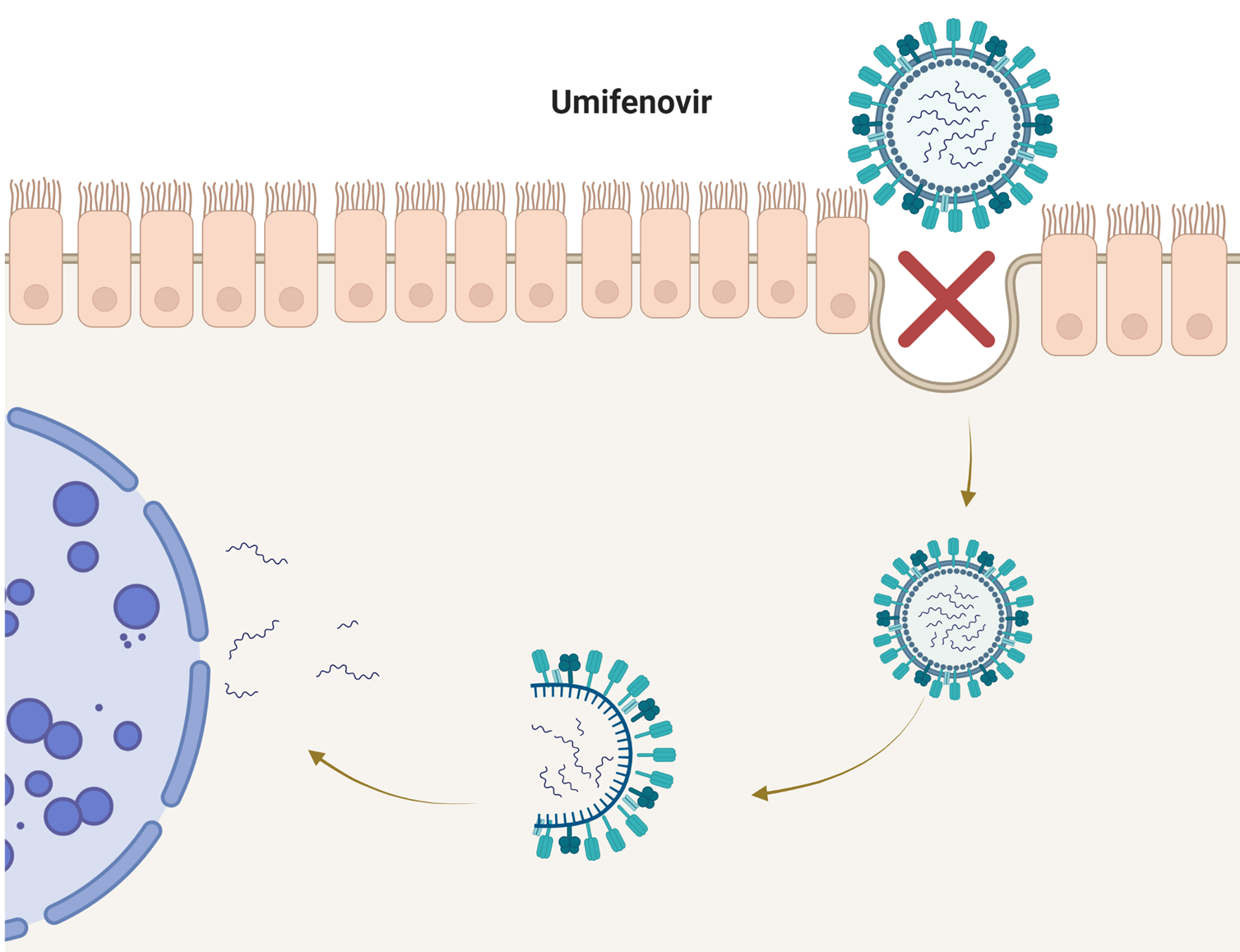
Figure 2. Proposed Umifenovir Mechanism. The current understanding of umifenovir’s method of action is based on its insertion into membrane lipids, leading to the inhibition of membrane fusion between virus particles and plasma membranes, as well as interfering with the fusion between virus particles and the membranes of endosomes. Made with BioRender.com.
Russian in vitro studies are plentiful and report IC50s for umifenovir in the 2.5–16 μM range [13][15][16][23][24][25]. One of the best sources of information on this drug currently is the I.I. Mechnikov Research Institute of Vaccines and Sera, Russian Academy of Medical Sciences, Moscow, Russia, and its affiliates. Most notably, these labs have performed tests in vivo [25][26], in vitro [17][21][23][27][28][29], and clinical trials [30][31] gauging the effectiveness of umifenovir against influenza strains, as well as other types of viruses. A recent in vitro study showed, using an MDCK cell-based enzyme-linked immunosorbent assay, that influenza A and B viruses from the 2012-2014 flu seasons were inhibited by umifenovir. Moreover, no markers of resistance were found in viruses isolated from umifenovir-treated patients [25]. Another in vitro study examined nasal swabs from 57 umifenovir-treated patients, with influenza A(H1N1), A(H3N2), and influenza B strains and found no sign of resistance [26]. An in vivo study also showed that umifenovir was effective against influenza A(H3N2) in orally treated mice at the daily doses of 15 mg/kg or 20 mg/kg [30]. Another notable in vivo study explored the effectiveness of umifenovir in post-influenza complications, specifically Staphylococcus aureus pneumonia, following the infection of the California 2009 A(H1N1) strain in mice. This study showed that oral 40 or 60 mg/kg/day doses increased the survival rate in mice from 0% to 90%. Furthermore, after dissection, the lungs of the treated mice displayed less severe histopathologic lesions as compared to the control group [26].
Two clinical studies also examined patients with either influenza or acute respiratory tract infection. The first clinical trial enrolled 215 patients aged 18-74 years and split them into placebo (n=106) and treatment (n=109) groups. The treatment group received umifenovir 200 mg four times a day for 5 days [31]. The second clinical trial enrolled 359 patients aged 18-65 years and split them into treatment (n=181) and placebo (n=178) groups. The treatment group received 800 mg/day for 5 days [30]. In both trials, both the influenza and acute respiratory tract infection patients were grouped. The patients in the umifenovir treatment group in both trials recovered faster and displayed fewer complications. Still, it is difficult to parse out what the results mean for umifenovir’s efficacy against influenza alone [30]. These studies reported no adverse effects attributed to umifenovir.
Umifenovir efficacy testing has been performed in labs in other countries as well, though such studies remain scarce. Studies out of China reported the efficacy of umifenovir against influenza A variants. An in vivo study from Wuhan University showed that 24 hours before virus exposure, at doses of 50 or 100 mg/kg/day for 6 days, umifenovir significantly reduced the rate of infection and mortality in mice infected with an influenza A strain [18]. An in vitro study also conducted at Wuhan University showed that umifenovir was effective against two influenza A(H1N1) strains, responsible for both seasonal and pandemic influenza, in MDCK cells via an MTT assay [32]. Afterward, an in vivo study on mice found that umifenovir treatment at oral doses of 90-180 mg/kg/day reduced viral lung titers and lesions. Additionally, the secretion of lung and macrophage cytokines was downregulated [32]. A more recent in vitro study from the First Affiliated Hospital of Guangzhou Medical University, Guangzhou, China showed that umifenovir inhibited other local influenza A(H1N1) variants, including A(H3N2) and A(H9N2), with IC50s ranging from 4.4 to 12.1μM [33]. The in vitro experiment performed shortly after on mice and ferrets showed that the survival rates of influenza-infected mice, given 25 mg/ml and 45 mg/ml umifenovir, were 40% and 50%, respectively. Moreover, these mice displayed reduced viral lung titers. The ferret data also showed a decrease in fever symptoms duration in umifenovir treatment groups as compared to controls [33]. A clinical trial conducted by the Department of Respiratory Diseases, in Beijing, China tested the efficacy of umifenovir on influenza on 125 influenza-infected patients. Of these patients, 59 were in the treatment group and 66 were in the placebo group. This clinical study reported that at a dose of 200 mg, administered orally 3 times per day for 5 days, the treatment group saw a significant reduction in symptoms and a median duration of illness of around 72 hours, compared to the placebo group’s 96 hours. Adverse effects were not attributed to umifenovir [34].
At the Department of Biotechnology and Environmental Biology, RMIT University, Bundoora, Victoria, Australia, both in vivo and in vitro testing revealed that umifenovir neither reduced lung viral titers nor caused a significant reduction of lung consolidation in mice after oral and intraperitoneal administration and intranasal challenge with a local influenza A(H3N2) strain. In cells, the therapeutic indices for influenza A and B were in the range of 1.9-8.5 and umifenovir was more effective against influenza A(H3N2) than rimantadine or amantadine [14]. Overall, the available studies indicate that umifenovir is an effective and broad-spectrum antiviral that works against several human pathogenic respiratory viruses, although its actual effectiveness remains in question until lab results are reproducible, globally.
3. Neuraminidase Inhibitors
NA inhibitors target the viral enzyme neuraminidase to inhibit viral release and are effective against influenza A and B [35]. NA inhibitors, as their name suggests, are a class of drugs that inhibit the actions of NA enzymes [35]. NA cleaves the terminal sialic acid from the carbohydrate residue on the surface of host cells, which influenza virus envelopes. This promotes the release of the virus from the infected cells which, in turn, allows the virus to spread [35]. NA inhibitors block the active site of this enzyme, which reduces viral shedding [5][35]. In this way, replication can be blocked by NA inhibitors, which prevent virions from being released from the surface of the infected host cells (Figure 3) [7].
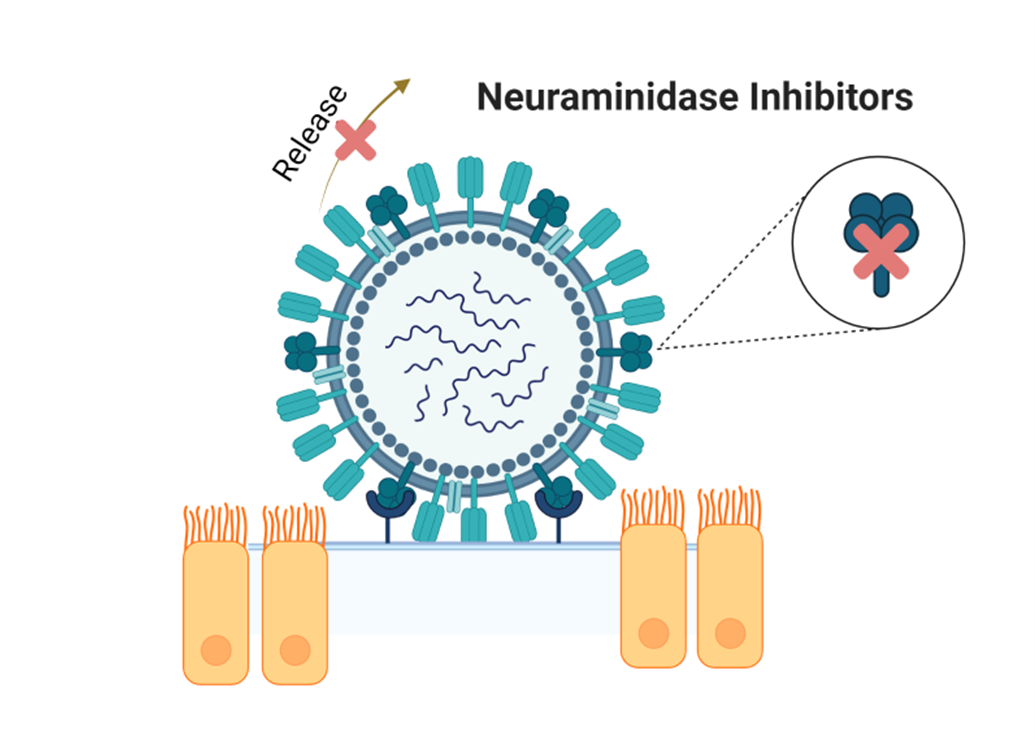
Figure 3. Neuraminidase Inhibitors. These antivirals prevent neuraminidase from acting on terminal sialic acid from the carbohydrate residue on the surface of the host cells, thereby inhibiting viral release and further replication. Made with BioRender.com.
As of the time of writing, of the four antivirals approved for the treatment of influenza in the United States, three, including oseltamivir (Tamiflu), zanamivir (Relenza Diskhaler), and peramivir (Rapivab), are NA inhibitors [36]. The recommended oseltamivir dosage for the treatment of acute influenza infection in adults, beginning within 2 days of symptom onset, is 75 mg taken orally twice daily for 5 days [37]. For prophylaxis, oseltamivir can be taken once daily for up to 42 days [38][39]. Oseltamivir is taken as a prodrug (oseltamivir phosphate) and converted by hepatic esterases into its active metabolite oseltamivir carboxylate, which has high bioavailability [38]. The recommended zanamivir dosage for the treatment of acute influenza in adults, beginning within 2 days after symptom onset, is 10 mg via oral inhalation twice daily for 5 days [40]. For prophylaxis, zanamivir can be taken once daily for up to 28 days [40]. Up to 15% of the dose is absorbed in the lungs [7][40]. The recommended dosage of peramivir for the treatment of acute influenza in adults, beginning within 2 days after symptom onset, is a single dose of 600 mg taken intravenously [41]. Peramivir displays a low binding affinity to human plasma (<30%) [41]. However, in healthy adult volunteers, the peak concentration of peramivir in both pharyngeal and bronchial epithelial lining fluid samples was greater than the IC50 value for influenza [42].
Whether NA inhibitors are genuinely effective treatmentsfor influenza A and B has been questioned in the past due to the sloppy clinical trials involving the drugs [43]. One large meta-analysis found that many of the clinical trials contained bias, and several (possibly) had an active substance as their placebo [43]. Several studies concluded that NA inhibitors shorten the duration of influenza symptoms, although not in all patients [43][44][45][46][47][48][49]. While using NA inhibitors for prophylaxis is effective, the use of oseltamivir increases the chance of adverse effects, such as nausea, vomiting, psychiatric effects, and renal events in adults, along with vomiting in children [43]. Zanamivir produces fewer adverse effects than the other two drugs in this class, possibly due to its lower bioavailability and inhalation route, while peramivir produces the most adverse effects, possibly due to its intravenous route of administration [43]. The balance between their potential adverse effects and their potential benefits should be carefully weighed before drug administration.
Resistance to NA inhibitors is drug-specific; however, given the similar structure shared by the drugs in this class, resistance to one can affect the activity of others. Amino acid substitutions in either the NA catalytic site or the HA receptor binding site of influenza viruses can cause resistance to NA inhibitors to arise [50]. The H275Y amino acid substitution of the neuraminidase gene found in various influenza A viruses provides resistance towards oseltamivir and peramivir. Similarly, E119E/V (found in influenza A(H3N2) and A(H7N9)) causes resistance to oseltamivir and R292K causes resistance to all three NA inhibitors, though lower resistance rates are observed for zanamivir [50][51][52]. While resistance to NA inhibitors can crop up in circulating strains, it is generally seen as rare [53][54][55], especially for zanamivir [56]. Regardless of its rarity, close monitoring for global NA inhibitor susceptibility is still required [50].
4. M2 Inhibitors (Adamantanes)
Adamantanes are a class of anti-influenza antivirals used specifically for treating type A influenza infections, although mass viral resistance has limited their recent use. There are only two members of this class, namely amantadine hydrochloride (Symmetrel) and rimantadine hydrochloride (flumadine), or simply amantadine and rimantadine, both of which are symmetric tricyclic amines [57]. Adamantanes are also called M2 inhibitors or M2 ion-channel inhibitors based on their mechanism of action [58]. M2 ion-channel inhibitors target the stage of viral uncoating. M2 proteins are responsible for forming the proton channels that lower the pH of the viral interior right before the dissociation of the matrix protein, which eventually leads to the uncoating of the viral genome during replication [5][59]. By inhibiting these ion channels, amantadine and rimantadine specifically inhibit the replication of influenza A strains (Figure 4) [60].
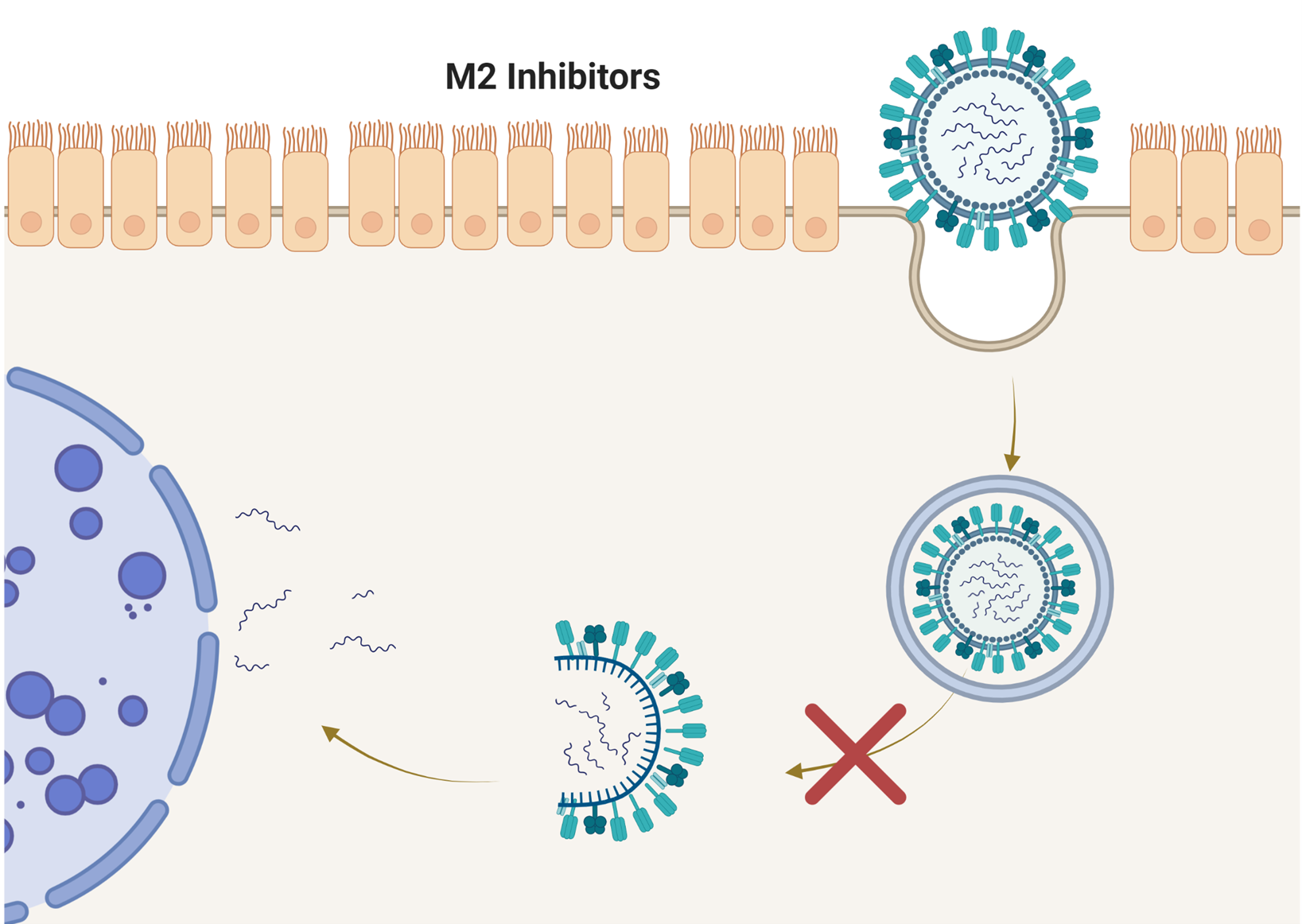
Figure 4. M2 Ion-Channel Inhibitors. These antivirals target the stage of viral uncoating and prevent it from happening altogether. This stops the virus from proceeding to the replication stage. Made with BioRender.com.
Amantadine and rimantadine are given in similar dosages administered orally, that is, 100 mg tablets and a syrup formulation of 50 mg/5ml [60]. The dosage for adults, for the treatment and prevention of influenza A, is 100 mg every 12 hours. Both drugs achieve peak levels within the body at around 3-5 hours after dosing. Amantadine is excreted unchanged by the kidneys but rimantadine undergoes extensive hepatic metabolism before renal excretion [61][62]. Common side effects of adamantanes are minor central nervous system complaints, such as anxiety, difficulty concentrating, insomnia, dizziness, and headaches, as well as gastrointestinal upset. Rarer but well-documented side effects include antimuscarinic effects, orthostatic hypotension, and congestive heart failure. Drug–drug interactions can occur within a large number of drug classes, including antihistamines and anticholinergic drugs, which further limits their usage [60][63][64].
Rimantadine is the structural analog of amantadine and is seen as the superior drug due to its larger volume of distribution, higher concentration in respiratory secretion, and more extensive metabolism that results in fewer central nervous system side effects [60][65]. However, rimantadine shares its specificity, mechanism of action, and potential for resistance with amantadine [66]. Cross-resistance to both drugs occurs when a single amino acid is substituted in the transmembrane portion of the M2 protein. Resistance has been noted to emerge as early as 2–4 days after the start of the therapy in up to 30% of the patients infected with strains that showed susceptibility to either drug [60]. Many studies have demonstrated influenza resistance to this drug class [67][68][69][70][71][72][73][74][75]. Due to the widespread resistance to M2 inhibitors exhibited by influenza A strains, these drugs are not currently recommended for the prevention or treatment of influenza in the United States [60][72][73].
5. Cap-Dependent Endonuclease Inhibitors
The cap-dependent endonuclease, found within the RNA polymerase subunit of influenza viruses, plays a crucial role in facilitating the cap-snatching process during the creation of viral mRNA. This process is essential for the replication of the virus [76]. Baloxavir marboxil (xofluza), or baloxavir, was approved for the treatment of uncomplicated influenza first in Japan and then in the United States in 2018, followed shortly thereafter by several other countries [77][78], making it the sole approved member of the antiviral class known as cap-dependent endonuclease inhibitors [5]. Baloxavir is a prodrug metabolized via hydrolysis into its active metabolite, baloxavir acid [79]. Baloxavir acid targets the replication stage of the viral life cycle and selectively inhibits the endonuclease activity of the polymerase acidic protein, one of the subunits of RNA polymerase [80]. The targeted endonuclease is a virus-specific enzyme required for viral gene transcription [81] which provides baloxavir its specificity. Through the inhibition of cap-dependent endonuclease, baloxavir can inhibit viral replication for both influenza A and B viruses [5][79] (Figure 5).
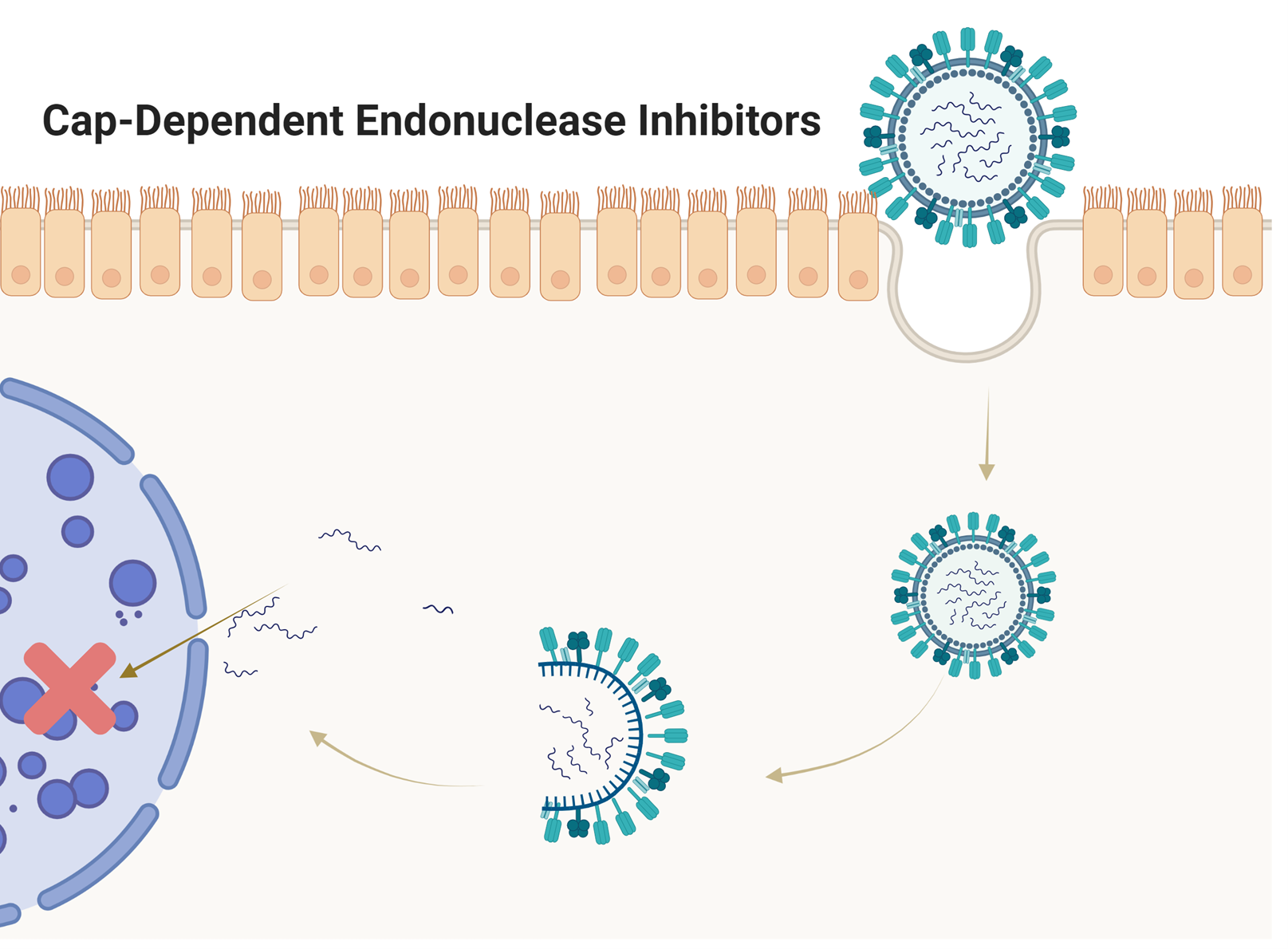
Figure 5. Cap-Dependent Endonuclease Inhibitors. These antivirals target the replication stage of the viral life cycle and selectively inhibit the endonuclease activity of the polymerase acidic protein, one of the subunits of RNA polymerase. Through inhibition of cap-dependent endonuclease, these antivirals inhibit influenza viral replication. Made with BioRender.com.
Baloxavir is metabolized in the liver mainly by the enzyme UGT1A3, with minor contributions by CYP3A4. To date, no serious drug-drug interactions have been documented, even with co-administered CYP3A and UGT inhibitors, such as probenecid [5][82]. Co-administration with medicines containing polyvalent cations, such as antacids, lowers the bioavailability of baloxavir. Baloxavir is mainly excreted in the feces, with minor excretions in the urine. Moreover, in patients with renal and hepatic impairments, baloxavir showed no altered pharmacokinetic properties [5][82]. Baloxavir is suggested for use in patients 12 years of age and older who have been symptomatic for a maximum of 48 hours and only for acute uncomplicated influenza [5][82]. In this regard, it is an inferior alternative to other antivirals that are also generally suggested for prophylaxis as well as influenza treatment. Baloxavir, however, is the preferred choice in patients where the use of NA inhibitors is contraindicated. Since it has a half-life of about 79 hours, baloxavir is given in a single-dose regimen [5][82]. In this regard, it is a superior treatment to other multi-dose regimens, as patient compliance is an issue with multiple-dose treatment plans.
While baloxavir can treat viruses resistant to NA inhibitors, the main problem in using baloxavir alone is the speed by which influenza viruses develop resistance towards it. Both influenza A and B can develop resistance, though A more so than B [5]. In an in vitro study, it was found that viruses substituted at I38 in the polymerase acidic protein, which resulted in reduced susceptibility to baloxavir [83]. Indeed, one clinical study that used this drug to treat influenza A(H3N2) reported that even after a single dose, a small subset of influenza patients developed resistance to it, with an overall rate of 19.5% resistance [77], while another clinical study showed resistance appearing between 8%-10% [84]. Interestingly, previous results reported a resistance rate of only 2.2%, however, the patients treated previously had contracted the 2009 A(H1N1) variant, the strain responsible for the 2009 pandemic [77].
In recent years, baloxavir resistance was only observed at the rates of 0.5% and 0.1% during the 2018-2019 and 2019-2020 flu seasons, respectively [85]. These results imply that baloxavir resistance varies across influenza strains and the drug remains a valid choice for treatment [86]. Additionally, when co-administered with oseltamivir, synergistic properties were shown between the two drugs. Moreover, resistance and drug-drug interactions were avoided [87][88][89]. Additionally, a recent study showed a lack of drug-drug interactions between baloxavir and NA inhibitors, though it failed to report improved clinical outcomes when compared to treatment plans consisting of a single antiviral [90]. These results suggest that if widespread viral resistance to baloxavir, NA inhibitors, or both occur in the future, co-administering baloxavir with an NA inhibitor may be the most effective treatment regimen to bypass resistance.
6. Conclusion
Antigenic drift in influenza strains allows these viruses to circumvent seasonal vaccines. Due to this fact, recent public interest, as well as recent scientific interest, has led to the reevaluation of older anti-influenza antivirals, as well as the development of new anti-influenza antivirals. Unfortunately, low genetic barriers to resistance will continue to be a problem for existing antivirals in the future. Even now, adamantanes are not recommended for widespread use due to the speed of resistance seen even after a single dose. Careful global monitoring of antiviral susceptibility to resistance is needed to ensure that the few antivirals currently available for the treatment of influenza do not end up obsolete in the same manner. Considering the low genetic barriers to resistance when given individually, combination therapy utilizing two or more antivirals may be a way to circumvent viral resistance, at least in the short term. As each class of antivirals has a unique mechanism of action, using a variety of anti-influenza antivirals may help to prevent resistance from cropping up quickly among influenza strains. In conclusion, the development of new antivirals, innovative combinations of existing treatments, and strategic co-administration with preventive measures, like vaccines, stand as most effective strategies against the persistent threat of influenza.
In-Text Abbreviations
HA: hemagglutinin
NA: neuraminidase
M2: Matrix-2
References
- Hayden F, Aoki F. Amantadine, rimantadine, and related agents; Williams & Wilkins, Eds.; Antimicrobial Chemotherapy: Baltimore, MD, 1999; pp. 1344–1365.
- David Y Gaitonde; Faith C Moore; Mackenzie K Morgan; Influenza: Diagnosis and Treatment. null. 2019, 100, 751-758.
- Jeffery K. Taubenberger; David M. Morens; Influenza: The Once and Future Pandemic. Public Heal. Rep.. 2010, 125, 15-26.
- Arnold S Monto; Keiji Fukuda; Lessons From Influenza Pandemics of the Last 100 Years. Clin. Infect. Dis.. 2019, 70, 951-957.
- I. Barberis; P. Myles; S.K. Ault; N.L. Bragazzi; M. Martini; History and evolution of influenza control through vaccination: from the first monovalent vaccine to universal vaccines. null. 2016, 57, E115-E120.
- Tianrui Yang; Baloxavir Marboxil: The First Cap-Dependent Endonuclease Inhibitor for the Treatment of Influenza. Ann. Pharmacother.. 2019, 53, 754-759.
- Björn F. Koel; Ramona Mögling; Salin Chutinimitkul; Pieter L. Fraaij; David F. Burke; Stefan van der Vliet; Emmie de Wit; Theo M. Bestebroer; Guus F. Rimmelzwaan; Albert D. M. E. Osterhaus; Derek J. Smith; Ron A. M. Fouchier; Miranda de Graaf; Identification of Amino Acid Substitutions Supporting Antigenic Change of Influenza A(H1N1)pdm09 Viruses. J. Virol.. 2015, 89, 3763-3775.
- Anne Moscona; Neuraminidase Inhibitors for Influenza. New Engl. J. Med.. 2005, 353, 1363-1373.
- Seizaburo Kashiwagi; Akira Watanabe; Hideyuki Ikematsu; Shinichiro Awamura; Takako Okamoto; Mitsutoshi Uemori; Katsuyasu Ishida; Laninamivir octanoate for post-exposure prophylaxis of influenza in household contacts: a randomized double blind placebo controlled trial. J. Infect. Chemother.. 2013, 19, 740-749.
- Kazumi Takahashi; Yousuke Furuta; Yoshiko Fukuda; Masako Kuno; Tomoko Kamiyama; Kyo Kozaki; Nobuhiko Nomura; Hiroyuki Egawa; Shinzaburo Minami; Kimiyasu Shiraki; In Vitroandin VivoActivities of T-705 and Oseltamivir against Influenza Virus. Antivir. Chem. Chemother.. 2003, 14, 235-241.
- Boriskin YS, Leneva IA, Pécheur EI, Polyak SJ. Arbidol: a broad-spectrum antiviral compound that blocks viral fusion. Curr. Med. Chem.. 2008, 10, 997-1005.
- Jan Haviernik; Michal Štefánik; Martina Fojtíková; Sabrina Kali; Noël Tordo; Ivo Rudolf; Zdeněk Hubálek; Luděk Eyer; Daniel Ruzek; Arbidol (Umifenovir): A Broad-Spectrum Antiviral Drug That Inhibits Medically Important Arthropod-Borne Flaviviruses. Viruses. 2018, 10, 184.
- P. G. Deryabin; T. M. Garaev; M. P. Finogenova; A. I. Odnovorov; Assessment of the antiviral activity of 2HCl*H-His-Rim compound compared to the anti-influenza drug Arbidol for influenza caused by A/duck/Novosibirsk/56/05 (H5N1) (Influenza A virus, Alphainfluenzavirus, Orthomyxoviridae). Probl. Virol.. 2019, 64, 268-273-273.
- Julie Blaising; Stephen J. Polyak; Eve-Isabelle Pécheur; Arbidol as a broad-spectrum antiviral: An update. Antivir. Res.. 2014, 107, 84-94.
- Megan J. Brooks; Elena I. Burtseva; Philip J. Ellery; Glenn A. Marsh; Andrew M. Lew; Anatoly N. Slepushkin; Suzanne M. Crowe; Gregory A. Tannock; Antiviral activity of arbidol, a broad‐spectrum drug for use against respiratory viruses, varies according to test conditions. J. Med Virol.. 2011, 84, 170-181.
- I T Fediakina; I A Leneva; S S Iamnikova; D K Livov; R G Glushkov; A M Shuster; [Sensitivity of influenza A/H5 viruses isolated from wild birds on the territory of Russia to arbidol in the cultured MDCK cells].. null. 2006, 50, 32-5.
- I T Fediakina; M Iu Shchelkanov; P G Deriabin; I A Leneva; N V Gudova; T V Kondrat'Eva; D K L'Vov; [Susceptibility of pandemic influenza virus A 2009 H1N1 and highly pathogenic avian influenza virus A H5N1 to antiinfluenza agents in cell culture].. null. 2011, 56, 3-9.
- I A Leneva; A M Shuster; [Antiviral etiotropic chemicals: efficacy against influenza A viruses A subtype H5N1].. null. 2006, 51, 4-7.
- L. Shi; H. Xiong; J. He; H. Deng; Q. Li; Q. Zhong; W. Hou; L. Cheng; H. Xiao; Z. Yang; Antiviral activity of arbidol against influenza A virus, respiratory syncytial virus, rhinovirus, coxsackie virus and adenovirus in vitro and in vivo. Arch. Virol.. 2007, 152, 1447-1455.
- Alhassan Ali Ahmed; Mohamed Abouzid; Arbidol targeting influenza virus A Hemagglutinin; A comparative study. Biophys. Chem.. 2021, 277, 106663.
- Rameshwar U. Kadam; Ian A. Wilson; Structural basis of influenza virus fusion inhibition by the antiviral drug Arbidol. Proc. Natl. Acad. Sci.. 2016, 114, 206-214.
- Irina A. Leneva; Rupert J. Russell; Yury S. Boriskin; Alan J. Hay; Characteristics of arbidol-resistant mutants of influenza virus: Implications for the mechanism of anti-influenza action of arbidol. Antivir. Res.. 2008, 81, 132-140.
- Elena V. Proskurnina; Dmitry Yu. Izmailov; Madina M. Sozarukova; Tatiana A. Zhuravleva; Irina A. Leneva; Artem A. Poromov; Antioxidant Potential of Antiviral Drug Umifenovir. Mol.. 2020, 25, 1577.
- E I Burtseva; E S Shevchenko; I A Leneva; L N Merkulova; T A Oskerko; O V Shliapnikova; A L Zaplatnikov; A M Shuster; A N Slepushkin; [Rimantadine and arbidol sensitivity of influenza viruses that caused epidemic morbidity rise in Russia in the 2004-2005 season].. null. 2007, 52, 24-9.
- A A Romanovskaia; A M Durymanov; K A Sharshov; A V Zaĭkovskaia; I M Susloparov; A M Shestopalov; I A Leneva; I G Drozdov; [Investigation of susceptibility of influenza viruses A (H1N1), the cause of infection in humans in April-May 2009, to antivirals in MDCK cell culture].. null. 2009, 54, 41-7.
- I A Leneva; I T Fediakina; M Iu Eropkin; N V Gudova; A A Romanovskaia; D M Danilenko; S M Vinogradova; A Iu Lepeshkin; A M Shestopalov; [Study of the antiviral activity of Russian anti-influenza agents in cell culture and animal models].. null. 2010, 55, 19-27.
- I A Leneva; I N Falynskova; E I Leonova; I T Fedyakina; N R Makhmudova; E A Osipova; L N Lepekha; N A Mikhailova; V V Zverev; [Umifenovir (Arbidol) efficacy in experimental mixed viral and bacterial pneumonia of mice].. null. 2014, 59, 17-24.
- Irina A. Leneva; Irina N. Falynskova; Nailya R. Makhmudova; Artem A. Poromov; Svetlana B. Yatsyshina; Viktor V. Maleev; Umifenovir susceptibility monitoring and characterization of influenza viruses isolated during ARBITR clinical study. J. Med Virol.. 2018, 91, 588-597.
- I.A. Leneva; E.I. Burtseva; E.S. Kirillova; L.V. Kolobukhina; A.G. Prilipov; A.L. Zaplatnikov; Moscow Russian Medical Academy Of Post-Graduate Education; Assessment of a risk for development of umifenovir resistance in epidemic strains of influenza A and B viruses in clinical settings. Infekc. Bolezn.. 2019, 17, n/a.
- I A Leneva; I T Fediakina; T A Gus'Kova; R G Glushkov; [Sensitivity of various influenza virus strains to arbidol. Influence of arbidol combination with different antiviral drugs on reproduction of influenza virus A].. null. 2005, 77, 84-8.
- N Yu Pshenichnaya; V A Bulgakova; N I Lvov; A A Poromov; E P Selkova; A I Grekova; I V Shestakova; V V Maleev; I A Leneva; Clinical efficacy of umifenovir in influenza and ARVI (study ARBITR). Ter. arkhiv. 2019, 91, 56-63.
- N. Pshenichnaya; V. Bulgakova; E. Selkova; V. Maleyev; N. Lvov; I. Leneva; A. Grekova; I. Shestakova; Umifenovir in treatment of influenza and acute respiratory viral infections in outpatient care. Int. J. Infect. Dis.. 2019, 79, 103-103.
- Qiang Liu; Hai-Rong Xiong; Li Lu; Yuan-Yuan Liu; Fan Luo; Wei Hou; Zhan-Qiu Yang; Antiviral and anti-inflammatory activity of arbidol hydrochloride in influenza A (H1N1) virus infection. Acta Pharmacol. Sin.. 2013, 34, 1075-1083.
- Yutao Wang; Yuewen Ding; Chunguang Yang; Runfeng Li; Qiuling Du; Yanbing Hao; Zhengtu Li; Haiming Jiang; Jin Zhao; Qiaoyan Chen; Zifeng Yang; Zhanlong He; Inhibition of the infectivity and inflammatory response of influenza virus by Arbidol hydrochloride in vitro and in vivo (mice and ferret). Biomed. Pharmacother.. 2017, 91, 393-401.
- Meng-Zhao Wang; Bai-Qiang Cai; Long-Yun Li; Jiang-Tao Lin; Nan Su; Hong-Xia Yu; He Gao; Jian-Zhong Zhao; Li Liu; [Efficacy and safety of arbidol in treatment of naturally acquired influenza].. null. 2004, 26, 289-93.
- Nongluk Sriwilaijaroen; Christopher J. Vavricka; Hiromasa Kiyota; Yasuo Suzuki. Influenza A Virus Neuraminidase Inhibitors; Springer Science and Business Media LLC: Dordrecht, GX, Netherlands, 2022; pp. 321-353.
- Hui-Chen Su; I-Jung Feng; Hung-Jen Tang; Mei-Fen Shih; Yi-Ming Hua; Comparative effectiveness of neuraminidase inhibitors in patients with influenza: A systematic review and network meta-analysis. J. Infect. Chemother.. 2021, 28, 158-169.
- Karen McClellan; Caroline M. Perry; Oseltamivir. Drugs. 2001, 61, 263-283.
- Brian E. Davies; Pharmacokinetics of oseltamivir: an oral antiviral for the treatment and prophylaxis of influenza in diverse populations. J. Antimicrob. Chemother.. 2010, 65, ii5-ii10.
- Annex I. Summary of product characteristics; Committee for Proprietary Medicinal Products, Eds.; The European Public Assessment Report (EPAR): Stocrin. London, 1999; pp. all.
- Michael Elliott; Zanamivir: from drug design to the clinic. Philos. Trans. R. Soc. B: Biol. Sci.. 2001, 356, 1885-1893.
- Lesley J. Scott; Peramivir: A Review in Uncomplicated Influenza. Drugs. 2018, 78, 1363-1370.
- Yutaka Saisho; Toru Ishibashi; Hidenori Fukuyama; Hiroyuki Fukase; Jingoro Shimada; Pharmacokinetics and Safety of Intravenous Peramivir, Neuraminidase Inhibitor of Influenza Virus, in Healthy Japanese Subjects. Antivir. Ther.. 2016, 22, 313-323.
- Tom Jefferson; Mark A Jones; Peter Doshi; Chris B Del Mar; Carl J Heneghan; Rokuro Hama; Matthew J Thompson; Elizabeth A Spencer; Igho J Onakpoya; Kamal R Mahtani; David Nunan; Jeremy Howick. Neuraminidase inhibitors for preventing and treating influenza in healthy adults and children; Wiley: Hoboken, NJ, United States, 2012; pp. CD008965.
- Timothy L. Wiemken; Stephen P. Furmanek; Ruth M. Carrico; Paula Peyrani; Daniel Hoft; Alicia M. Fry; Julio A. Ramirez; Effectiveness of oseltamivir treatment on clinical failure in hospitalized patients with lower respiratory tract infection. BMC Infect. Dis.. 2021, 21, 1-7.
- Mark H Ebell; Marlene Call; JoAnna Shinholser; Effectiveness of oseltamivir in adults: a meta-analysis of published and unpublished clinical trials. Fam. Pr.. 2012, 30, 125-133.
- Carl J Heneghan; Igho Onakpoya; Matthew Thompson; E. A. Spencer; Mark Jones; Tom Jefferson; Zanamivir for influenza in adults and children: systematic review of clinical study reports and summary of regulatory comments. BMJ. 2014, 348, g2547-g2547.
- Atsuko Hata; Ryoko Akashi-Ueda; Kazufumi Takamatsu; Takuro Matsumura; Safety and efficacy of peramivir for influenza treatment. Drug Des. Dev. Ther.. 2014, 8, 2017-2038.
- Milena M McLaughlin; Erik W Skoglund; Michael G Ison; Peramivir: an intravenous neuraminidase inhibitor. Expert Opin. Pharmacother.. 2015, 16, 1889-1900.
- Jen-Wei Liu; Shen-Hua Lin; Lin-Chien Wang; Hsiao-Yean Chiu; Jen-Ai Lee; Comparison of Antiviral Agents for Seasonal Influenza Outcomes in Healthy Adults and Children. JAMA Netw. Open. 2021, 4, e2119151-e2119151.
- Ha T Nguyen; Alicia M Fry; Larisa V Gubareva; Neuraminidase inhibitor resistance in influenza viruses and laboratory testing methods. Antivir. Ther.. 2012, 17, 159-173.
- Aeron C Hurt; Tawee Chotpitayasunondh; Nancy J Cox; Rod Daniels; Alicia M Fry; Larisa V Gubareva; Frederick G Hayden; David S Hui; Olav Hungnes; Angie Lackenby; Wilina Lim; Adam Meijer; Charles Penn; Masato Tashiro; Timothy M Uyeki; Maria Zambon; Antiviral resistance during the 2009 influenza A H1N1 pandemic: public health, laboratory, and clinical perspectives. Lancet Infect. Dis.. 2012, 12, 240-248.
- Lady Tatiana Pinilla; Benjamin P. Holder; Yacine Abed; Guy Boivin; Catherine A. A. Beauchemin; The H275Y Neuraminidase Mutation of the Pandemic A/H1N1 Influenza Virus Lengthens the Eclipse Phase and Reduces Viral Output of Infected Cells, Potentially Compromising Fitness in Ferrets. J. Virol.. 2012, 86, 10651-10660.
- Temi Lampejo; Influenza and antiviral resistance: an overview. Eur. J. Clin. Microbiol. Infect. Dis.. 2020, 39, 1201-1208.
- Nelson Lee; Aeron C. Hurt; Neuraminidase inhibitor resistance in influenza: a clinical perspective. Curr. Opin. Infect. Dis.. 2018, 31, 520-526.
- Yong Chong; Shinya Matsumoto; Dongchon Kang; Hideyuki Ikematsu; Consecutive influenza surveillance of neuraminidase mutations and neuraminidase inhibitor resistance in Japan. Influ. Other Respir. Viruses. 2018, 13, 115-122.
- Kristian Thorlund; Tahany Awad; Guy Boivin; Lehana Thabane; Systematic review of influenza resistance to the neuraminidase inhibitors. BMC Infect. Dis.. 2011, 11, 134-134.
- Tom Jefferson; Vittorio Demicheli; Carlo Di Pietrantonj; Daniela Rivetti; Amantadine and rimantadine for influenza A in adults. Cochrane Database Syst. Rev.. 2006, 2006, CD001169.
- Jessica L. Thomaston; Marley L. Samways; Athina Konstantinidi; Chunlong Ma; Yanmei Hu; Hannah E. Bruce Macdonald; Jun Wang; Jonathan W. Essex; William F. DeGrado; Antonios Kolocouris; Rimantadine Binds to and Inhibits the Influenza A M2 Proton Channel without Enantiomeric Specificity. Biochem.. 2021, 60, 2471-2482.
- Rafal M. Pielak; James J. Chou; Influenza M2 proton channels. Biochim. et Biophys. Acta (BBA) - Biomembr.. 2010, 1808, 522-529.
- Michael G. Ison. Antiviral Agents against Respiratory Viruses; Wiley: Hoboken, NJ, United States, 2009; pp. 401-428.
- Bessey Geevarghese; Eric Af Simões; Antibodies for prevention and treatment of respiratory syncytial virus infections in children. Antivir. Ther.. 2012, 17, 201-211.
- Hayden F, Aoki F. Amantadine, rimantadine, and related agents; Antimicrobial Chemotherapy: Baltimore, MD, 1999; pp. 1344–1365.
- F G Hayden; A Minocha; D A Spyker; H E Hoffman; Comparative single-dose pharmacokinetics of amantadine hydrochloride and rimantadine hydrochloride in young and elderly adults. Antimicrob. Agents Chemother.. 1985, 28, 216-221.
- Susan M. Wintermeyer; Milap C. Nahata; Rimantadine: A Clinical Perspective. Ann. Pharmacother.. 1995, 29, 299-310.
- Debasis Mondal. Rimantadine; Elsevier BV: Amsterdam, NX, Netherlands, 2007; pp. 1-4.
- D.R. Snydman; Incidence of Adamantane Resistance Among Influenza A (H3N2) Viruses Isolated Worldwide From 1994 to 2005: A Cause for Concern. Yearb. Med.. 2006, 2006, 71-72.
- I.G. Barr; A.C. Hurt; P. Iannello; C. Tomasov; N. Deed; N. Komadina; Increased adamantane resistance in influenza A(H3) viruses in Australia and neighbouring countries in 2005. Antivir. Res.. 2007, 73, 112-117.
- MMWR. Update: Influenza Activity - United States, 2009-10 season. MMWR Morb Mortal Wkly Rep.. 2010, 59(29), 901-908.
- Guoying Dong; Chao Peng; Jing Luo; Chengmin Wang; Le Han; Bin Wu; Guangju Ji; Hongxuan He; Adamantane-Resistant Influenza A Viruses in the World (1902–2013): Frequency and Distribution of M2 Gene Mutations. PLOS ONE. 2015, 10, e0119115-e0119115.
- Kyoko Shiraishi; Keiko Mitamura; Yuko Sakai‐Tagawa; Hideo Goto; Norio Sugaya; Yoshihiro Kawaoka; High Frequency of Resistant Viruses Harboring Different Mutations in Amantadine‐Treated Children with Influenza. J. Infect. Dis.. 2003, 188, 57-61.
- A. Kumar; D. Funk; Emergence of a Novel Swine-Origin Influenza A (H1N1) Virus in Humans. Yearb. Crit. Care Med.. 2010, 2010, 176-177.
- Varough M. Deyde; Xiyan Xu; Rick A Bright; Michael Shaw; Catherine B. Smith; Ye Zhang; Yuelong Shu; Larisa V. Gubareva; Nancy J. Cox; Alexander I. Klimov; Surveillance of Resistance to Adamantanes among Influenza A(H3N2) and A(H1N1) Viruses Isolated Worldwide. J. Infect. Dis.. 2007, 196, 249-257.
- Natalia A. Ilyushina; Elena A. Govorkova; Charles J. Russell; Erich Hoffmann; Robert G. Webster; Contribution of H7 haemagglutinin to amantadine resistance and infectivity of influenza virus. J. Gen. Virol.. 2007, 88, 1266-1274.
- Silvia Carnaccini; Daniel R. Perez; H9 Influenza Viruses: An Emerging Challenge. Cold Spring Harb. Perspect. Med.. 2020, 10, a038588.
- Simon Portsmouth; Keiko Kawaguchi; Masatsugu Arai; Kenji Tsuchiya; Takeki Uehara; Cap-dependent Endonuclease Inhibitor S-033188 for the Treatment of Influenza: Results from a Phase 3, Randomized, Double-Blind, Placebo- and Active-Controlled Study in Otherwise Healthy Adolescents and Adults with Seasonal Influenza. Open Forum Infect. Dis.. 2017, 4, S734-S734.
- Frederick G. Hayden; Norio Sugaya; Nobuo Hirotsu; Nelson Lee; Menno D. de Jong; Aeron C. Hurt; Tadashi Ishida; Hisakuni Sekino; Kota Yamada; Simon Portsmouth; Keiko Kawaguchi; Takao Shishido; Masatsugu Arai; Kenji Tsuchiya; Takeki Uehara; Akira Watanabe; Baloxavir Marboxil for Uncomplicated Influenza in Adults and Adolescents. New Engl. J. Med.. 2018, 379, 913-923.
- Michael G Ison; Simon Portsmouth; Yuki Yoshida; Takao Shishido; Melissa Mitchener; Kenji Tsuchiya; Takeki Uehara; Frederick G Hayden; Early treatment with baloxavir marboxil in high-risk adolescent and adult outpatients with uncomplicated influenza (CAPSTONE-2): a randomised, placebo-controlled, phase 3 trial. Lancet Infect. Dis.. 2020, 20, 1204-1214.
- Takashi Hashimoto; Keiko Baba; Kae Inoue; Miyako Okane; Takahiro Noda; Satoshi Hata; Takao Shishido; Akira Naito; Steffen Wildum; Shinya Omoto. Comprehensive assessment of amino acid substitutions in the trimeric RNA polymerase complex of influenza virus detected in clinical trials of baloxavir marboxil; Authorea, Inc.: Brooklyn, NY, United States, 2020; pp. n/a.
- Liva Checkmahomed; Blandine Padey; Andrés Pizzorno; Olivier Terrier; Manuel Rosa-Calatrava; Yacine Abed; Mariana Baz; Guy Boivin; In Vitro Combinations of Baloxavir Acid and Other Inhibitors against Seasonal Influenza A Viruses. Viruses. 2020, 12, 1139.
- Alexandre Dias; Denis Bouvier; Thibaut Crépin; Andrew A. McCarthy; Darren J. Hart; Florence Baudin; Stephen Cusack; Rob W. H. Ruigrok; The cap-snatching endonuclease of influenza virus polymerase resides in the PA subunit. Nat.. 2009, 458, 914-918.
- Pharmaceu-ticals, Inc. XofluzaTM [package insert]; n/a: South San Francisco, CA, 2014; pp. n/a.
- Shinya Omoto; Valentina Speranzini; Takashi Hashimoto; Takeshi Noshi; Hiroto Yamaguchi; Makoto Kawai; Keiko Kawaguchi; Takeki Uehara; Takao Shishido; Akira Naito; Stephen Cusack; Characterization of influenza virus variants induced by treatment with the endonuclease inhibitor baloxavir marboxil. Sci. Rep.. 2018, 8, 1-15.
- Takeki Uehara; Frederick G Hayden; Keiko Kawaguchi; Shinya Omoto; Aeron C Hurt; Menno D De Jong; Nobuo Hirotsu; Norio Sugaya; Nelson Lee; Keiko Baba; Takao Shishido; Kenji Tsuchiya; Simon Portsmouth; Hiroshi Kida; Treatment-Emergent Influenza Variant Viruses With Reduced Baloxavir Susceptibility: Impact on Clinical and Virologic Outcomes in Uncomplicated Influenza. J. Infect. Dis.. 2019, 221, 346-355.
- Emi Takashita; Rod S. Daniels; Seiichiro Fujisaki; Vicki Gregory; Larisa V. Gubareva; Weiijuan Huang; Aeron C. Hurt; Angie Lackenby; Ha T. Nguyen; Dmitriy Pereyaslov; Merryn Roe; Magdi Samaan; Kanta Subbarao; Herman Tse; Dayan Wang; Hui-Ling Yen; Wenqing Zhang; Adam Meijer; Global update on the susceptibilities of human influenza viruses to neuraminidase inhibitors and the cap-dependent endonuclease inhibitor baloxavir, 2017–2018. Antivir. Res.. 2020, 175, 104718.
- Larisa V Gubareva; Alicia M Fry; Baloxavir and Treatment-Emergent Resistance: Public Health Insights and Next Steps. J. Infect. Dis.. 2019, 221, 337-339.
- Keita Fukao; Takeshi Noshi; Atsuko Yamamoto; Mitsutaka Kitano; Yoshinori Ando; Takahiro Noda; Kaoru Baba; Kazumi Matsumoto; Naoko Higuchi; Minoru Ikeda; Takao Shishido; Akira Naito; Combination treatment with the cap-dependent endonuclease inhibitor baloxavir marboxil and a neuraminidase inhibitor in a mouse model of influenza A virus infection. J. Antimicrob. Chemother.. 2018, 74, 654-662.
- Nao Kawaguchi; Hiroki Koshimichi; Toru Ishibashi; Toshihiro Wajima; Evaluation of Drug–Drug Interaction Potential between Baloxavir Marboxil and Oseltamivir in Healthy Subjects. Clin. Drug Investig.. 2018, 38, 1053-1060.
- Pool Tobar Vega; Elena Caldeira; Hasan Abad; Peguy Saad; Erik Lachance; Oseltamivir and baloxavir: Dual treatment for rapidly developing ARDS on a patient with renal disease. IDCases. 2020, 21, e00819.
- Deepali Kumar; Michael G Ison; Jean-Paul Mira; Tobias Welte; Jick Hwan Ha; David S Hui; Nanshan Zhong; Takefumi Saito; Laurie Katugampola; Neil Collinson; Sarah Williams; Steffen Wildum; Andrew Ackrill; Barry Clinch; Nelson Lee; Combining baloxavir marboxil with standard-of-care neuraminidase inhibitor in patients hospitalised with severe influenza (FLAGSTONE): a randomised, parallel-group, double-blind, placebo-controlled, superiority trial. Lancet Infect. Dis.. 2022, 22, 718-730.



