Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Haneesh Jasuja | -- | 5271 | 2024-03-05 03:35:15 | | | |
| 2 | Camila Xu | Meta information modification | 5271 | 2024-03-05 04:19:27 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Katti, P.D.; Jasuja, H. Tissue Engineering for Cancer Metastasis Therapeutics. Encyclopedia. Available online: https://encyclopedia.pub/entry/55848 (accessed on 28 July 2026).
Katti PD, Jasuja H. Tissue Engineering for Cancer Metastasis Therapeutics. Encyclopedia. Available at: https://encyclopedia.pub/entry/55848. Accessed July 28, 2026.
Katti, Preeya D., Haneesh Jasuja. "Tissue Engineering for Cancer Metastasis Therapeutics" Encyclopedia, https://encyclopedia.pub/entry/55848 (accessed July 28, 2026).
Katti, P.D., & Jasuja, H. (2024, March 05). Tissue Engineering for Cancer Metastasis Therapeutics. In Encyclopedia. https://encyclopedia.pub/entry/55848
Katti, Preeya D. and Haneesh Jasuja. "Tissue Engineering for Cancer Metastasis Therapeutics." Encyclopedia. Web. 05 March, 2024.
Copy Citation
Tissue engineering is a promising field for regenerative medicine that is likely to be able to provide rehabilitation procedures to patients who have undergone surgeries, such as mastectomy and other reconstructive procedures. Another important use of tissue engineering has emerged recently that involves the development of realistic and robust in vitro models of cancer metastasis, to aid in drug discovery and new metastasis therapeutics, as well as evaluate cancer biology at metastasis.
tissue engineering
cancer
metastasis
in vitro models
3D models
1. Introduction
Cancer is emerging as a leading cause of premature death worldwide [1]. Globally, the World Health Organization reported 9.6 million deaths in 2018, making cancer the second leading cause of death worldwide. The large global economic burden of cancer from 2020 to 2050 was estimated to be USD 25.2 trillion [2]. Metastasis remains the primary cause of death due to cancer [3]. In a 2022 study, it was estimated that 623,405 people were living with metastatic cancers or metastatic melanoma in the US, and that number is expected to increase to 693,452 by the year 2025 [4]. A 2007 study reported that the economic burden for patients with metastatic bone diseases is USD 12.6 billion. This number represents 17% of the total medical burden estimated by the National Institutes of Health [5]. A more recent 2022 study estimated that the bone metastasis burden has increased to 20% of the overall oncology costs [6]. Alarmingly, most survivors with metastatic cancer of various types, except melanoma, have a life expectance of less than five years [4]. Palliative treatments are often the only course of treatment for metastasis. For example, at bone metastasis, palliative treatment includes the use of drugs, such as bisphosphonates and Denosumab, which are used to stabilize skeletal issues [7][8]. The complex cascade of biochemical and resulting pathological events that lead to metastasis to bone is still mostly unknown. This knowledge is further hampered by the lack of appropriate and relevant model systems for testing new drugs and therapies. In vitro models mimicking bone metastasis are much needed for this purpose.
All types of cancers can spread. The mechanisms of spreading cancer are varied. These range from cancer invading normal tissue in its proximity, traveling through either the lymphatic system or blood vessels to other parts of the body, attaching to invading blood vessel walls and forming tumors, to the growth of new blood vessels that enable metastatic tumor growth. Different cancers have the propensity to metastasize to specific locations in the body, e.g., breast cancer and prostate cancer tend to spread to the bones, and colon cancer and pancreatic cancer spread to the liver, as shown in Figure 1. Metastasis is the cause of most patient deaths, yet the mechanisms of metastasis remain primarily unknown. The process is fundamentally described as a two-step process, with the initial dislocation of cancer from its primary site and transportation of cells to a distant site through blood and lymph systems, and the phenomenon of recolonization of cancer at the remote site [9].
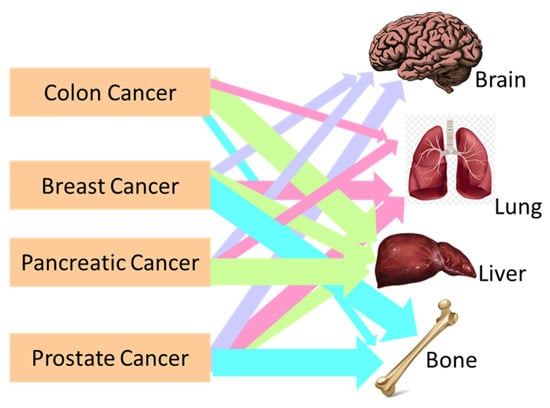
Figure 1. Schematic representation showing the metastasis locations of colon, breast, pancreatic, and prostate cancer in the human body.
Tumorigenesis has been traditionally studied in 2D cultures of cancer cells. Although many characteristics of cancer cells have been well explored using these 2D cell culture systems, they do not replicate the realistic tumor microenvironment. The 3D culture systems have been increasingly gaining attention for the past few years. These systems include 3D spheroids of cancer cells. Extensive studies report using 3D spheroid models of cancer [10], and their important use in screening drugs. The spheroids are fundamentally clusters of cancer cells that are grown either in suspension or embedded in a matrix. Although the spheroids have 3D structures, they do not accurately capture the mechanical, biological, and chemical characteristics of the metastasis site. While extensive studies are undertaken on the development of the complex chemo-physio-mechanical analogs of the primary site of cancer [11], efforts in producing accurate 3D models of metastasis are rare, as they do not represent the migration characteristics of metastasis well.
Further, transwell-based assays are useful to assess the inherent migratory and invasion characteristics of cancer cells [12][13][14]. Migration is an important characteristic of cancer cells that are likely to arrive at the metastatic site—they do not capture the behavior of the cells at metastasis. Several detailed reviews illustrate the important use of transwell assay-based models [15]. To develop a deeper understanding of the process of cancer metastasis and to be able to aid in the development of effective therapies for metastasis prevention and cure, in vitro and in vivo models are extensively investigated. While in vivo models can capture the complexity of living systems and are generally considered useful models for studying primary cancer types, they often fail to develop into cancer metastasis.
Robust in vitro models present themselves as a fast, inexpensive evaluation route for the study of cancer metastasis. The extremely high-cost and time-intensive nature of PDX models further necessitates robust in vitro systems that effectively represent cancer and metastasis stages. Many in vitro models have been developed for capturing various aspects of tumor growth, proliferation, invasion into tissues, intra and extravasation through blood vessels, angiogenic characteristics, and also delivery of drugs and their efficacies [15]. The source of cancer cells, either commercial or patient-derived origins, for seeding the in vitro models is just as important. Many commercial cell lines of several cancer types are easily available and are used to study tumor cell biology and proliferation [16][17]. The molecular profiles and various characterizations of human cancer cell lines are available in the Cancer Line Encyclopedia [10][18][19][20]. Often, the spectrum of variabilities within a particular cancer type is very vast, and the commercial cell lines are not able to capture such a wide spectrum of variabilities and, thus, achieve limited clinical relevance for patients [21]. Patient-derived cell lines are thus increasingly popular as a source in the development of in vitro cancer models. While cell lines from patients, even with advanced cancer stages, are available [22], the availability of cancer cell lines from metastasized tissue types is rare.
2. Tissue Engineering
Tissue engineering provides an important platform for the design of site-specific structural and biological similarity of metastasis. Tissue engineering is an interdisciplinary field that aims to develop new tissue and organ substitutes using biological sciences and engineering. The primary components of tissue engineering include biomaterials and scaffolds, cells, and regulatory signals, such as the use of growth factors (Figure 2).
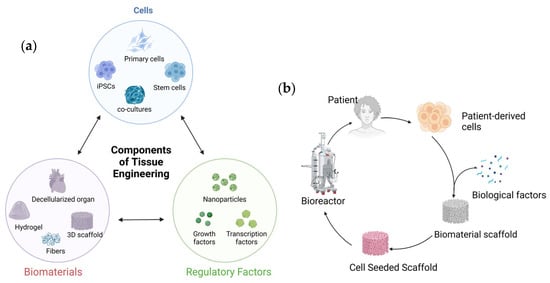
Figure 2. Schematic showing tissue engineering: (a) three important components of tissue engineering and (b) the tissue engineering process.
Originally proposed by Langer and Vacanti [23], it remains the forefront technology for regenerative medicine. The three important components of tissue engineering are the cells, regulatory signals, such as growth factors, and biomaterials, such as scaffolds (Figure 2a). The scaffolds are designed with porous microstructures and made of degradable materials. When seeded with appropriate human cells in the presence of growth factors, it enables the formation of engineered tissues, while the scaffolds themselves degrade. The development of in vitro models of cancer metastasis benefits from advances in tissue engineering of brain, lung, liver, and bone tissue. Tissue engineering has the potential to transform cancer research by providing mechanisms to observe tumorigenesis and migration at metastasis directly. Inducing angiogenesis is an important hallmark of cancer [24][25] and, thus, growth of solid tumors is often associated with neovascularization. Tissue engineering also provides the ability to recapitulate the tumor microenvironment and its complex and multifold characteristics [26]. The phenomenon of neovascularization around tumors was observed over a 100 years ago [27]. Thus, the importance of angiogenesis for tumor development also makes the tissue-engineered scaffolds with engineered porosities a promising platform for studying cancer metastasis. Thus, tissue-engineered constructs can also be used to study angiogenic characteristics of tumor growth factors. Hypoxic conditions of the tumors lead to the production of pro-angiogenic factors that enable neovascularization in the tumors. VEGF is an important angiogenic factor that plays a vital role in tumor growth as well as metastasis [28]. Hence, many antiangiogenic drugs (AAD) are used clinically. The exact mechanics of the AAD in controlling metastasis remain unknown [29]. Hence, VEGF-loaded scaffolds are extensively investigated for bone regeneration [30][31]. Scaffolds are used to evaluate the role of angiogenic factors in tumorigenic properties [32]. Cancer cells also secrete other growth factors and cytokines, such as basic fibroblast growth factor and interleukin-8, which also promote blood vessel formation and can thus be incorporated into the scaffolds.
The tissue engineering approaches toward understanding cancer have been studied extensively over the last two decades [33], enabling the advent of bioengineered tumors that represent viable in vitro models of cancer [34][35][36] using many biomaterial constructs [37][38][39][40]. It is expected that the next-generation 3D tissue-engineered constructs may replace animals in cancer drug testing [41]. The specific role of the metastasis site microenvironment is an important area of scientific investigation [42]. Recent advances in regenerative medicine pave the way for new cancer therapeutics as well as methodologies for the evaluation of fundamental cancer biology at metastasis [43][44].
In addition, in recent years, the development of bioreactors that provide important mechanical cues through fluid-enabled shear stresses has brought further development in viable in vitro models [45][46][47][48]. The metastasis condition is often delayed, as clinically, cancer cells are reported to remain dormant at the distant site after the removal of the tumor from the primary site. Tissue-engineered constructs also represent an effective methodology to evaluate the influence of local microenvironments at the metastasis site [42]. Dormancy of tumors is often an important issue that affects early diagnosis and intervention and, hence, the resulting metastasis. Tissue-engineered models, albeit few as of now, are also attempted to evaluate tumor dormancy and reactivation [49]. In vitro models are also useful in these cases to study the behavior of the dormant cells due to the difficulty in obtaining patient samples [50].
Tissue engineering also shows promise in providing therapeutic opportunities for cancer treatment. Patients suffering from post-prostatectomy incontinence or erectile dysfunction due to prostate cancer, or who need reconstructive surgeries, can be treated with tissue engineering therapies [51][52][53]. Bone and other cancers are also treated with the use of tissue-engineered scaffolds [54].
3. Cancer Metastasis 3D In Vitro Models
3.1. Breast Cancer Metastasis Models
Female breast cancer is reported as the most common cancer and the fourth highest in mortality due to cancer [55]. Cancer originating in the breast can metastasize to the lungs, brain, and bone. Therapies and treatments for bone metastasis of breast cancer are primarily palliative. Metastasis of breast cancer to bone is not curable. The blood-induced mechanical stresses and cancer cell–host (bone) interactions are the major players in bone metastasis of breast cancer. Various material systems are used to develop scaffolds that mimic bone sites. While extensive studies remain underway on the design of primary breast cancer with co-cultures of various cells [56], recent works also report tissue-engineered bone metastasis models. Mimicking the complex dynamic environment of the bone site on arrival of the cancer cells is a useful and valuable approach currently being investigated [57]. Many unique material models have been used to develop tissue-engineered bone structures to evaluate the bone metastasis of breast cancer. These models use a variety of polymeric scaffolds with and without infiltration with bone-forming minerals. A detailed overview of the various materials used to develop the bone niche and cell lines investigated is shown in Table 1. Each material model is tested with in vitro experimentations that validate some hallmarks of breast/prostate cancer colonization to bone.
Table 1. List of materials and cells for developing the bone niche for breast cancer bone metastasis models.
| Material Class | Material Type | Cell Types | References |
|---|---|---|---|
| Collagens | Collagen fibers and hydroxyapatite | HUVEC (human umbilical cord endothelial cells) Breast cancer cells tested: SUM149, SUM159, MDA-MB-231, BT474, MCF7, T47D, ZR75 |
[58][59] |
| Dense collagen hydrogel | MDA-MB-231 breast cancer cells and MC3T3-E1 pre-osteoblasts | [60] | |
| Collagen-glycosaminoglycan (GAG) | Murine mammary adenocarcinoma 4T1 cells | [61] | |
| Collagen gel seeded with osteo-differentiated human bone marrow-derived mesenchymal stem cells | MDA-MB-231 human breast cancer cells | [62] | |
| Heavily mineralized collagen fibers for a bone-on-a-chip | A co-culture of metastatic breast cancer cells and osteoblasts GFP-labeled metastatic breast cancer cell line, MDA-MB-231GFP cells, and metastasis-suppressed breast cancer cell line, MDA-MB-231-BRMS1GFP cells |
[63] | |
| 3D Collagen matrix (GELFOAM), seeded with endothelial, bone marrow stromal cells, and fetal osteoblasts | MDA-MB-231, BoM1833 | [59] | |
| PCL | 3D-printed scaffolds made of Piezo-electro-ceramics, such as BaTiO3 with polycaprolactone | In vitro models of MDA MB231 breast cancer cell migration and invasion studies | [41][64] |
| 3D-printed polycaprolactone (PCL) scaffolds with dispersed HAP | This in vitro model shows migration of MDA-MB-231, MCF-7, and MDA-MB-453 breast cancer cells toward the bone | [65][66] | |
| PCL scaffolds coated with fibronectin and collagen IV | Human LM2-4 cells derived from MDA-MB-231 cells and mouse 4T1 cells | [67] | |
| Random and aligned PCL fibers | Chemo-resistant MDA-MB-231 and T47D breast cancer cells | [68] | |
| PCL with nano-clay–biomimetic hydroxyapatite | MCF 7, MDA 231, patient-derived cell lines | [69][70][71][72][73][74] | |
| PEG | Polyethylene glycol hydrogel and nanocrystalline hydroxyapatite composite scaffolds |
MDA-MB-231 | [75] |
| Silk Proteins | Fibrous proteins derived from natural fibers derived from silkworms and spiders | MDA MB 231, MCF 7 | [76][77][78] |
| Silk protein scaffolds | Human breast cancer cells injected into the mammary fat pads of mice | [49][50][51][77] | |
| 3D-printed spatially layered bone tissues with gelatin to generate a layered structure of scaffold that has an outer ring composed of tissue-engineered bone and a center composed of macroporous scaffolds that host cancer cells | MDA MB 231 | [79] | |
| Polyurethane | Polyurethane foam scaffold | MCF7 | [80] |
| PLA-PGA | Poly (lactide-co-glycolide) PLA-PGA scaffolds dispersed with nanoHAP particles | MDA-MB231 | [81][82] |
| Chitosan | NanoHAP inside a chitosan gel | MDA-MB-231, MCF-7, and transfected MDA-MB-231 | [83] |
The bone extracellular matrix (ECM) is considered an attractive site for cancer cell attachment, growth, and survival [84]. Since bone ECM consists of cells, collagen fibers, and hydroxyapatite, extensive studies have been performed using 3D structures fabricated using collagen. Many efforts in the literature involve using collagen fibers to create bone niches. Recent studies use these structures seeded with primary human mesenchymal stem cells and several breast cancer cells: SUM149, SUM159, MDA-MB-231, BT474, MCF7, T47D, and ZR75 [58][59]. Dense collagen hydrogels are fabricated to study the interactions between triple-negative breast cancer cells and bone cells. In particular, the effect of osteolytic breast cancer cells on osteoblast differentiation is studied [60]. Due to the osteogenic characteristic of the mineral hydroxyapatite (HAP), often, collagen composites with HAP are investigated as bone surrogates. Collagen fibers decorated with HAP nanocrystals were made using porcine type 1 atelocollagen [85]. Studies performed with animal models have shown high osteoconductivity and biosorbibility of the HAP-decorated collagen fibers [86][87], as well as the use of these scaffolds to treat osteochondral defects via delivery of paclitaxel to breast cancer bone metastasis in a rat model [88].
Mammary cells can calcify within the breast tissue, and researchers have utilized the development of an in vitro model of mammary mineralization using murine mammary adenocarcinoma 4T1 cells. These studies make use of collagen-glycosaminoglycan (GAG) scaffolds to mimic the bone environment using murine mammary adenocarcinoma 4T1 cells [61].
Another use of collagen is in a gel form seeded with osteo-differentiated human bone marrow-derived mesenchymal stem cells. This model has successfully used microfluidics to evaluate the extravasation process of the triple-negative and highly metastatic MDA-MB-231 human breast cancer cells [62]. Mineralized collagen fibers were also used for developing a bone-on-a-chip with a co-culture of metastatic breast cancer cells and osteoblasts [63]. A 3D model of the bone niche was fabricated from a collagen matrix (GELFOAM), using endothelial, bone marrow stromal cells, and fetal osteoblasts. This model attempted to evaluate the genes responsible for breast cancer dormancy [59].
Polycapralactone (PCL) is a synthetic biodegradable polyester with a low melting point (~60 °C). PCL is easily degraded by hydrolysis under physiological conditions and is, hence, a commonly used polymer for biomaterial applications. HAP is a commonly used osteogenic ingredient in the scaffold composite. For bone regeneration, PCL infiltrated with various minerals has been used to enhance and/or create osteoinductive, piezoelectric, and strength properties of the polymer. Polycaprolactone (PCL) scaffolds with dispersed HAP have been fabricated using 3D printing to create bone-like models. This in vitro model is used to demonstrate the migration of MDA-MB-231, MCF-7, and MDA-MB-453 breast cancer cells toward the bone [65][66]. The 3D-printed scaffolds made of PCL infiltrated with a piezoceramic barium titanate (BaTiO3) were used to fabricate bone, specifically for load-bearing applications [64]. This bone analog was attempted for use in in vitro models to evaluate MDA MB231 breast cancer cell migration and invasion [41]. Further, microporous PCL scaffolds with polyelectrolyte layers attached to the inner pores were also suggested for use in drug delivery applications [89]. Besides in vitro models, tissue-engineered xenograft models of breast cancer bone metastasis using PCL fibers have recently been attempted [90].
The cancer pre-metastatic niche is composed of ECM proteins (e.g., fibronectin and collagen IV) that play an important role in colonization of cancer cells at the bone niche. In a recent study, microporous ECM protein-coated PCL scaffolds were used to recruit cancer cells in vivo. These models attempted to create a premetastatic niche and were specifically used to evaluate proteins that aide in cancer cell bone metastasis [67]. Researchers have also used random and aligned PCL fibers to mimic the random and organized orientation of collagen fibers in the ECM. Chemo-resistant MDA-MB-231 and T47D breast cancer cells were used to evaluate the efficacy of such an in vitro model, specifically for understanding dormancy in metastasis [68].
PCL infiltrated with nanohydroxyapatite has also been fabricated through a biomimetic process that utilized nano-clay modification with amino acids [91]. Nano-clay–HAP–PCL scaffolds prepared using freeze extraction were used to design in vitro models of breast cancer bone metastasis using a sequential culture of human mesenchymal stem cells and MCF7 and MDA MB231 breast cancer cells [69]. Using this model, the same authors were able to derive mechanics and spectroscopy-based markers of metastasis [71][72], as well as elucidate that the WnT pathway regulates osteogenesis for breast cancer bone metastasis [74].
The PCL–HAP–nano-clay model was also used with patient-derived breast cancer estrogen-receptor-positive (ER+) and triple-negative (TN) breast cancer tissues to study osteolytic and osteoblastic implications of breast cancer on bone [70] as well as evaluate drug efficacies [73]. Soft gel-like material systems incorporated with nanoHAP were used for 3D-printed structures with vasculature and seeding with multiple cell types to investigate breast cancer metastasis to bone [92]. The choice of gelatin in these models is owing to the fact that gelatin is partially denatured collagen, and the biochemical properties of gelatin are similar to the organic component of bone.
Polyethylene glycol (PEG) is an important hydrophilic polymer commonly used for biomedical applications, due to its excellent biocompatibility, non-immunogenity, and protein repulsion. PEG polymer composites with hydroxyapatite have been attempted as bone biomaterials. Polyethylene glycol hydrogel with nanocrystalline hydroxyapatite is used to make composite scaffolds to mimic the bone native environment. This in vitro model was used to study the interaction between breast cancer cells and osteoblasts [75].
The Kaplan group has pioneered the use of silk proteins for bone tissue engineering [93]. Fibrous proteins derived from natural fibers derived from silkworms and spiders have exceptional mechanical properties. Silk scaffolds seeded with bone marrow stromal cells (BMSC) were implanted in mouse models of human breast cancer metastasis [76]. The silk scaffolds represent a suitable bone niche for metastasis of human breast cancer [76][77][78]. These models have been used to study both breast and prostate cancer bone metastasis.
Polyurethanes are important engineering polymers that have found applications in biomedical engineering due to their biocompatibility, biostability, and degradability. Polyurethane foam scaffolds are investigated as bone surrogates and used as bone metastasis models [80]. The advantage of the PU foam is the apparent highly porous architecture that mimics the trabecular bone. Breast cancer cells, MCF-7-derived tumor-initiating cells (MCFS), were used to evaluate the metastasis condition in these studies.
Similarly, the highly biocompatible and degradable nature of poly (lactide-co-glycolide) (PLA-PGA) polymeric materials makes them useful as bone scaffolds. Scaffolds made using PLA-PGA reinforced with nanoHAP particles were used for the evaluation of adhesion and proliferation of MDA-MB231 breast cancer cells to bone [81][82].
Further, mimicking breast cancer-induced bone metastasis was also evaluated in vivo using human cancer cells or tissues transplanted into immunocompromised hosts to form xenografts that replicate the bone metastasis [94].
3.2. Prostate Cancer Metastasis Models
Prostate cancer cells also metastasize to bone, exhibiting osteomimicry, and are the subject of many investigations [40]. The interactions between the prostate cancer cells and the bone microenvironment are crucial for metastasis progression. Understanding the underlying mechanisms of metastasis of prostate cancer to bone was investigated [95]. Key bone modeling and remodeling process regulatory factors, such as -kappa B (RANK)/RANKL/OPG, the WnT pathways, growth factors, such as TGFb, and specifically, bone morphogenic proteins, are known to be intrinsically involved in the prostate cancer bone metastasis [74][95]. Macro-fluidic models to evaluate the process of metastasis were also attempted [96]. Many attempts have been made to create bone-mimetic environments, such as the bone-mimetic niche for prostate cancer metastasis. For reasons similar to those described for breast cancer metastasis to bone, polycaprolactone scaffolds are fabricated and used for bone scaffolds. Polymers such as PCL and gelatin are also extensively used in bone mimicry for developing bone metastasis models of prostate cancer. Table 2 summarizes the various polymeric, composite, and biological materials that are used in the development of tissue-engineered scaffolds to mimic the bone site of prostate cancer metastasis.
Table 2. List of materials and cells for developing the bone niche for prostate cancer bone metastasis models.
| Materials System | Material Form | Cell Types | References |
|---|---|---|---|
| Collagens | Collagen gel | Co-culture of human MG-63 osteoblast-like cells with highly metastatic human PC3 prostate cancer cells | [97] |
| Collagen-glycosaminoglycan and nanohydroxyapatite composites | PC3 and LNCaP | [98] | |
| Collagen nanofibers with nanohydroxyapatite grafted with SPARC | LNCaP | [99][100][101] | |
| Collagen-hydroxyapatite scaffolds | PC3 and DU145 | [102] | |
| Gelatin | 3D printing to generate a layered structure of scaffold that has an outer ring composed of tissue-engineered bone and a center composed of macroporous scaffolds that host cancer cells | PC3 | [79] |
| PCL | Medical-grade polycaprolactone–calcium phosphate (mPCL–CaP) scaffolds | PC3 and LNCaP | [103][104][105] |
| Medical-grade PCL: culturing primary human osteoprogenitor cells on melt electrowritten PCL scaffolds | LNCaP, C4-2B, and PC3 | [106] | |
| Electrospun PCL fibers and PCL/gelatin composite scaffolds modified with perlecan domain IV (PlnDIV) peptide | C4-2B cancer cells | [107] | |
| PCL–nano-clay–nanohydroxyapatite scaffolds | PC3 and PCa | [91][108][109] | |
| Tubular PCL scaffolds coated with calcium phosphate were fabricated by melt electro-writing PCL | LuCaP35 | [110] | |
| Silk Proteins | Scaffolds fabricated from silk proteins derived from Bombyx mori. | PC3 | [78] |
| Scaffolds fabricated using silk protein fibroin from Bombyx mori and recombinant spider silk protein spidroin (SSP1) with gelatin, collagen, and chitosan, indicating potential advantages | LNCaP | [111] | |
| PLA-PLGA | PLGA and nanohydroxyapatite scaffolds | PC3 | [112] |
| Curcumin-impregnated poly(lactic-co-glycolic) acid (PLGA) scaffolds | [113] | ||
| PEG | Polyethylene glycol hydrogel | PCa and LNCaP | [114] |
| Scaffolds fabricated with poly(ethylene glycol)-fibrinogen matrix supplemented with poly(ethylene glycol)-diacrylate | PC3 with BJ-5ta fibroblasts | [115] |
One of the early studies reported the development of a three-dimensional type I collagen gel cell culture system with co-culture of human MG-63 osteoblast-like cells with highly metastatic human PC3 prostate cancer cells. This model was used to study the pathophysiology of prostate cancer at the bone [97].
Recent studies using collagen 3D scaffolds include collagen composites with glycosaminoglycan and nanoHAP [98]. This model was effectively used to study chemosensitivity, cell migration, and proliferation, as well as evaluating the efficacy of delivery of nanoparticle-based gene therapeutics. Other studies reported the use of collagen–nanohydroxyapatite scaffolds containing 5-fold nanohydroxyapatite to collagen by weight, followed by seeding with prostate cancer cells, PC3 and DU145 [102]. New therapeutic studies that evaluate the efficacy of anisamide-targeted amphiphilic cyclodextrin nanoparticles for therapeutic gene silencing are enabled using this model.
Researchers have fabricated scaffolds made using collagen fibers infiltrated with nanoHAP that are further grafted with the glycoprotein SPARC (secreted protein, acidic, and rich in cysteine), known to play a role in bone mineralization. The experiments conducted on the model indicated that the addition of SPARC enabled the survival and growth of the PCa cell line (LNCaP) on the bone-mimetic scaffold.
In the same study where a layered structure with an outer layer of tissue-engineered bone and a breast cancer cell core was fabricated to mimic in vivo metastasis development [79], the authors also used the layered structure for evaluation of prostate cancer metastasis development using PC3 and LNCaP prostate cancer cells. In this study, the authors demonstrated the integration of the layered 3D in vitro model with single-cell RNA sequencing to study fundamental signaling drivers of metastasis [79].
Polycaprolactone is commonly used in bone scaffold development, as described earlier, for developing breast cancer bone metastasis models. A cell-sheet-based technique that consists of wrapping medical-grade polycaprolactone–tricalcium phosphate (mPCL-TCP) scaffolds within hOB sheets was used [103]. An innovative scaffold design consisting of assembly of porcine bone marrow stromal cell (BMSC) cell sheets with medical-grade polycaprolactone–calcium phosphate (mPCL–CaP) scaffolds was utilized to develop bone grafts [105]. Interactions between the prostate cancer cells PC3 or LNCaP with hOBs were investigated. The interactions of PC3 and LNCaP prostate cancer cells with human osteoblasts were studied on these scaffold assemblies [103], followed by animal model experiments [104]. Studies conducted using this model indicate that the prostate cancer cell–bone matrix interactions resulted in elevated levels of metastasis markers, such as elevated MMPs, PSA, and steroidogenic enzymes.
In a recent work, electrospun PCL fibers and PCL/gelatin composite scaffolds were modified with perlecan domain IV (PlnDIV) peptide and used to develop a pharmacokinetic model to evaluate the proliferation, survival, and migration of C4-2B cancer cells [107]. These studies indicated that PlnDIV peptide plays an important role in the 3D model by helping in the proliferation, survival, and migration of C4-2B cancer cells.
As described earlier for breast cancer models, PCL infiltrated with biomimetic nanohydroxyapatite using nano-clay modification with amino acids [91] was also used to develop a prostate cancer bone-mimetic model using a sequential culture of human mesenchymal stem cells, with the highly metastatic PC3 and low metastatic PCa prostate cancer cells [108][109]. This model was also used in combination with perfusion flow and horizontal flow bioreactors, indicating the role of flow-derived shear stresses in the process of metastasis [46][47][48].
Tubular PCL scaffolds coated with calcium phosphate were fabricated by melt electro-writing PCL and seeded with human osteoprogenitor cells to form bone-mimetic scaffolds [110]. These scaffolds were used to create patient-derived xenograft (PDX) models of lymph node metastasis (LuCaP35) and bone metastasis (BM18) tissues from patients with primary prostate cancer and represent a viable route to derive osteomimicry environments with patient-derived tissues. In a recent study, primary human osteoprogenitor cells were cultured on melt electro-written PCL scaffolds from medical-grade PCL [106]. On these scaffolds, the co-culture of prostate cancer cell lines (LNCaP, C4-2B, and PC3) enables the evaluation of molecular features on these cancer types, as observed in vivo.
The Kaplan group developed an in vitro model using silk proteins derived from Bombyx mori and seeded with prostate cancer cells, PC3 [78]. Experiments conducted with this model indicated that BMP-2 stimulates cancer cell migration. The 3D cultivation of epithelial prostate cancer cells (LNCaP) has also been attempted using silk protein fibroin from Bombyx mori and recombinant spider silk protein spidroin (SSP1) with gelatin, collagen, and chitosan [111], indicating potential advantages.
In a recent work, 3D PLGA and nanohydroxyapatite were fabricated using electro-spraying, compacting, and foaming techniques. These scaffolds were used to evaluate drug toxicity and PC3 cells’ proliferation in bone-like environments [112]. Researchers have also impregnated curcumin into poly(lactic-co-glycolic) acid (PLGA) scaffolds [113]. These studies indicated that curcumin-impregnated PLGA shows increased efficacy against PCa and PC3 bone metastasis using xenograft models.
Co-cultures of human PCa, LNCaP, and human osteoblast cells were seeded onto polyethylene glycol hydrogel scaffolds to study the proliferation of LNCaP prostate cancer cells [114]. These studies illustrate a paracrine effect that promotes osteomimicry and provides insight into the prostate cancer–bone crosstalk. To modulate the mechanical properties of the matrix, researchers have attempted to develop a poly (ethylene glycol)–fibrinogen matrix supplemented with excess poly(ethylene glycol)–diacrylates. In this work, the authors used PC3 prostate cancer cells with BJ-5ta fibroblasts, and presented this new model to study drug treatments and cancer progression [115].
3.3. Colon Cancer Metastasis Models
Worldwide, colon cancer remains the fourth most common cancer and the third highest cause of death [55]. Colorectal tumor cells metastasize to the liver and lungs through hematogenous processes or lymphatics. Several attempts to use biomaterials have been made toward controlled drug delivery to colorectal cancer [116][117]. Metastasis is the most common cause of death due to colorectal cancer, with the liver being the most common metastasis site. Due to the high number of fatalities due to colorectal cancer metastasis, there is interest in developing 3D models of metastasis. A detailed description of the material systems and 3D models used to create the metastatic niche of colon cancer is shown in Table 3.
Table 3. List of materials and cells for developing the colon cancer metastasis models.
| Material Class | Material Form | Cell Types | References |
|---|---|---|---|
| Decellularized tissue scaffolds | Liver decellularized scaffolds seeded with colorectal cancer cells in mice models | HT-29, CRC119, SW480, and Caco2 | [118] |
| Patient-derived decellularized colon tissue | HT-29 | [119][120][121] | |
| Decellularized porcine livers to generate scaffolds | HCT116 | [122] | |
| Decellularized porcine small intestine submucosa + mucosa scaffolds | SW480 and SW480 colon cancer cells | [123] | |
| PLGA | E-jet 3D printing of PLGA | HCT-116 and LoVo human colon cancer cell lines, and p53-null (knockout) human colon cancer cell line (HCT-116 p53−/−) | [124] |
A recent study showed promising results in the use of liver decellularized scaffolds seeded with colorectal cancer cells in mice models [118]. Some researchers have attempted to use decellularized colorectal cancer tissue from biopsies [121] and patient-derived decellularized colon tissue to recapitulate colorectal cancer liver metastasis [119][120]. Generally, decellularized matrices represent the current methodologies in in vitro development of metastasized tissue for the development of new therapeutic agents. Another recent study used decellularized porcine livers to generate scaffolds. On these scaffolds, HCT116 colorectal spheroids were created [122]. In another study, decellularized porcine small intestine submucosa + mucosa was used to create 3D scaffolds that were seeded with SW480 and SW480 colon cancer cells and presented as a tool for testing metastasis mechanisms as well as the efficacy of drugs [123].
One attempt at creating a synthetic polymeric biomaterial scaffold involved scaffolds prepared using E-jet 3D printing of PLGA seeded with HCT-116 and LoVo human colon cancer cell lines, as well as the p53-null (knockout) human colon cancer cell line (HCT-116 p53−/−) [124].
Although the advantages of a true metastatic niche using tissue engineering are known, these attempts are limited to liver metastasis of colon cancer. In vivo models have been studied to evaluate the metastasis potential of colon cancer cells [125][126][127][128]. Many recent studies have focused on use of patient-derived organoids for evaluation of metastatic potential [129]. Tissue engineering and biomaterials are needed to create 3D in vitro models of colorectal cancer metastasis [130]. There is an unmet need to develop liver mimetic tissue-engineered scaffolds to evaluate metastasis therapeutics and colon cancer progression.
3.4. Pancreatic Cancer Metastasis Models
Although the incidence of pancreatic cancer is lower, ranking fourteenth in cancer incidence worldwide, mortality is 94% of the incidence [55]. The common sites of metastasis of pancreatic cancer are the liver (76–80% of patients), peritoneum (48%), and the lungs (45%) [131]. The liver metastasis of pancreatic cancer is a multistage and multistep process. The primary pancreatic tumor is highly invasive and, hence, in vitro models are mainly developed at the primary site. Mouse models have traditionally been extensively studied to understand the pathobiology of pancreatic cancer tumors [132].
The in vitro models of pancreatic cancer create the primary site of cancer. The 3D organoid structures are currently being investigated to evaluate the pathology and migration of primary site pancreatic cancer [133][134]. Recently, 3D organoids developed from patient tissue sources or genetically engineered mouse models have been developed as tools for patient-specific therapies of primary site pancreatic cancer and are suitable as preclinical models of pancreatic cancer [135]. Decellularized tissue scaffolds have also been attempted for use as viable models of late-stage pancreatic cancer. In one study, decellularized human pancreas and livers were seeded with PANC-1 and MIA PaCa-2 cell lines and PK-1 cells (liver-derived metastatic pancreatic cancer cell line) [136]. A novel recent study used tissue engineering approaches with a porous polyurethane scaffold modified with fibronectin and seeded with pancreatic cancer cells (PANC-1). In vitro hypoxia was administered in this model to study the impact of radiotherapy treatment [137].
References
- Bray, F.; Laversanne, M.; Weiderpass, E.; Soerjomataram, I. The ever-increasing importance of cancer as a leading cause of premature death worldwide. Cancer 2021, 127, 3029–3030.
- Chen, S.; Cao, Z.; Prettner, K.; Kuhn, M.; Yang, J.; Jiao, L.; Wang, Z.; Li, W.; Geldsetzer, P.; Bärnighausen, T.; et al. Estimates and Projections of the Global Economic Cost of 29 Cancers in 204 Countries and Territories From 2020 to 2050. JAMA Oncol. 2023, 9, 465–472.
- Fares, J.; Fares, M.Y.; Khachfe, H.H.; Salhab, H.A.; Fares, Y. Molecular principles of metastasis: A hallmark of cancer revisited. Signal Transduct. Target. Ther. 2020, 5, 28.
- Gallicchio, L.; Devasia, T.P.; Tonorezos, E.; Mollica, M.A.; Mariotto, A. Estimation of the Number of Individuals Living with Metastatic Cancer in the United States. JNCI J. Natl. Cancer Inst. 2022, 114, 1476–1483.
- Schulman, K.L.; Kohles, J. Economic burden of metastatic bone disease in the U.S. Cancer 2007, 109, 2334–2342.
- DiCaprio, M.R.; Murtaza, H.; Palmer, B.; Evangelist, M. Narrative review of the epidemiology, economic burden, and societal impact of metastatic bone disease. Ann. Jt. 2022, 7.
- Brown, J.E.; Neville-Webbe, H.; Coleman, R.E. The role of bisphosphonates in breast and prostate cancers. Endocr. Relat. Cancer 2004, 11, 207–224.
- Kostenuik, P.J.; Nguyen, H.Q.; McCabe, J.; Warmington, K.S.; Kurahara, C.; Sun, N.; Chen, C.; Li, L.; Cattley, R.C.; Van, G.; et al. Denosumab, a fully human monoclonal antibody to RANKL, inhibits bone resorption and increases BMD in knock-in mice that express chimeric (murine/human) RANKL. J. Bone Min. Res. 2009, 24, 182–195.
- Chaffer, C.L.; Weinberg, R.A. A Perspective on Cancer Cell Metastasis. Science 2011, 331, 1559–1564.
- Ghandi, M.; Huang, F.W.; Jane-Valbuena, J.; Kryukov, G.V.; Lo, C.C.; McDonald, E.R.; Barretina, J.; Gelfand, E.T.; Bielski, C.M.; Li, H.; et al. Next-generation characterization of the Cancer Cell Line Encyclopedia. Nature 2019, 569, 503–508.
- Buskin, A.; Scott, E.; Nelson, R.; Gaughan, L.; Robson, C.N.; Heer, R.; Hepburn, A.C. Engineering prostate cancer in vitro: What does it take? Oncogene 2023, 11, 2417–2427.
- Justus, C.R.; Leffler, N.; Ruiz-Echevarria, M.; Yang, L.V. In vitro Cell Migration and Invasion Assays. J. Vis. Exp. JoVE 2014, 88, 51046.
- Pijuan, J.; Barcelo, C.; Moreno, D.F.; Maiques, O.; Siso, P.; Marti, R.M.; Macia, A.; Panosa, A.; Migration, C. In vitro Cell Migration, Invasion, and Adhesion Assays: From Cell Imaging to Data Analysis. Front. Cell Dev. Biol. 2019, 7, 107.
- Hu, J.; Verkman, A.S. Increased migration and metastatic potential of tumor cells expressing aquaporin water channels. FASEB J. 2006, 20, 1892–1894.
- Katt, M.E.; Placone, A.L.; Wong, A.D.; Xu, Z.S.; Searson, P.C. In Vitro Tumor Models: Advantages, Disadvantages, Variables, and Selecting the Right Platform. Front. Bioeng. Biotechnol. 2016, 4, 12.
- Holliday, D.L.; Speirs, V. Choosing the right cell line for breast cancer research. Breast Cancer Res. 2011, 13, 215.
- Neve, R.M.; Chin, K.; Fridlyand, J.; Yeh, J.; Baehner, F.L.; Fevr, T.; Clark, L.; Bayani, N.; Coppe, J.P.; Tong, F.; et al. A collection of breast cancer cell lines for the study of functionally distinct cancer subtypes. Cancer Cell 2006, 10, 515–527.
- Nusinow, D.P.; Szpyt, J.; Ghandi, M.; Rose, C.M.; McDonald, E.R.; Kalocsay, M.; Jané-Valbuena, J.; Gelfand, E.; Schweppe, D.K.; Jedrychowski, M.; et al. Quantitative Proteomics of the Cancer Cell Line Encyclopedia. Cell 2020, 180, 387–402.e16.
- Cao, S.B.; Strong, M.J.; Wang, X.; Moss, W.N.; Concha, M.; Lin, Z.; O’Grady, T.; Baddoo, M.; Fewell, C.; Renne, R.; et al. High-Throughput RNA Sequencing-Based Virome Analysis of 50 Lymphoma Cell Lines from the Cancer Cell Line Encyclopedia Project. J. Virol. 2015, 89, 713–729.
- Barretina, J.; Caponigro, G.; Stransky, N.; Venkatesan, K.; Margolin, A.A.; Kim, S.; Wilson, C.J.; Lehár, J.; Kryukov, G.V.; Sonkin, D.; et al. The Cancer Cell Line Encyclopedia enables predictive modelling of anticancer drug sensitivity. Nature 2012, 483, 603–607.
- Sharma, S.V.; Haber, D.A.; Settleman, J. Cell line-based platforms to evaluate the therapeutic efficacy of candidate anticancer agents. Nat. Rev. Cancer 2010, 10, 241–253.
- Gao, D.; Vela, I.; Sboner, A.; Iaquinta, P.J.; Karthaus, W.R.; Gopalan, A.; Dowling, C.; Wanjala, J.N.; Undvall, E.A.; Arora, V.K.; et al. Organoid Cultures Derived from Patients with Advanced Prostate Cancer. Cell 2014, 159, 176–187.
- Langer, R.; Vacanti, J.P. Tissue Engineering. Science 1993, 260, 920–926.
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The Next Generation. Cell 2011, 144, 646–674.
- Carmeliet, P.; Jain, R.K. Angiogenesis in cancer and other diseases. Nature 2000, 407, 249–257.
- Tiwari, A.; Trivedi, R.; Lin, S.Y. Tumor microenvironment: Barrier or opportunity towards effective cancer therapy. J. Biomed. Sci. 2022, 29, 27.
- Goldmann, E. The Growth of Malignant Disease in Man and the Lower Animals, with special reference to the Vascular System. Proc. R. Soc. Med. Surg. Sect. 1908, 1, 1–13.
- Yang, X.; Zhang, Y.; Hosaka, K.; Andersson, P.; Wang, J.; Tholander, F.; Cao, Z.; Morikawa, H.; Tegner, J.; Yang, Y.; et al. VEGF-B promotes cancer metastasis through a VEGF-A-independent mechanism and serves as a marker of poor prognosis for cancer patients. Proc. Natl. Acad. Sci. USA 2015, 112, E2900–E2909.
- Yang, Y.; Cao, Y. The impact of VEGF on cancer metastasis and systemic disease. Semin. Cancer Biol. 2022, 86, 251–261.
- Kaigler, D.; Wang, Z.; Horger, K.; Mooney, D.J.; Krebsbach, P.H. VEGF scaffolds enhance angiogenesis and bone regeneration in irradiated osseous defects. J. Bone Miner. Res. 2006, 21, 735–744.
- Li, B.; Wang, H.; Zhou, G.; Zhang, J.; Su, X.; Huang, Z.; Li, Q.; Wu, Z.; Qiu, G. VEGF-loaded biomimetic scaffolds: A promising approach to improve angiogenesis and osteogenesis in an ischemic environment. RSC Adv. 2017, 7, 4253–4259.
- Rawal, P.; Tripathi, D.M.; Nain, V.; Kaur, S. VEGF-mediated tumour growth and EMT in 2D and 3D cell culture models of hepatocellular carcinoma. Oncol. Lett. 2022, 24, 315.
- Tilkorn, D.J.; Lokmic, Z.; Chaffer, C.L.; Mitchell, G.M.; Morrison, W.A.; Thompson, E.W. Disparate Companions: Tissue Engineering Meets Cancer Research. Cells Tissues Organs 2010, 192, 141–157.
- Villasante, A.; Marturano-Kruik, A.; Vunjak-Novakovic, G. Bioengineered human tumor within a bone niche. Biomaterials 2014, 35, 5785–5794.
- Villasante, A.; Vunjak-Novakovic, G. Bioengineered tumors. Bioengineered 2015, 6, 73–76.
- Yang, Q.; Li, M.M.; Yang, X.M.; Xiao, Z.; Tong, X.Y.; Tuerdi, A.; Li, S.S.; Lei, L.J. Flourishing tumor organoids: History, emerging technology, and application. Bioeng. Transl. Med. 2023, 22, e10559.
- Curvello, R.; Kast, V.; Ordonez-Moran, P.; Mata, A.; Loessner, D. Biomaterial-based platforms for tumour tissue engineering. Nat. Rev. Mater. 2023, 8, 314–330.
- Unnikrishnan, K.; Thomas, L.V.; Kumar, R.M.R. Advancement of Scaffold-Based 3D Cellular Models in Cancer Tissue Engineering: An Update. Front. Oncol. 2021, 11, 11.
- da Rocha, E.L.; Porto, L.M.; Rambo, C.R. Nanotechnology meets 3D in vitro models: Tissue engineered tumors and cancer therapies. Mater. Sci. Eng. C 2014, 34, 270–279.
- Safarulla, S.; Khillar, P.S.; Kini, S.; Jaiswal, A.K. Tissue engineered scaffolds as 3D models for prostate cancer metastasis to bone. Mater. Today Commun. 2021, 28, 12.
- Shah, L.; Latif, A.; Williams, K.J.; Mancuso, E.; Tirella, A. Invasion and Secondary Site Colonization as a Function of In Vitro Primary Tumor Matrix Stiffness: Breast to Bone Metastasis. Adv. Healthc. Mater. 2023, 12, 14.
- Costard, L.S.; Hosn, R.R.; Ramanayake, H.; O’Brien, F.J.; Curtin, C.M. Influences of the 3D microenvironment on cancer cell behaviour and treatment responsiveness: A recent update on lung, breast and prostate cancer models. Acta Biomater. 2021, 132, 360–378.
- Mansouri, V.; Beheshtizadeh, N.; Gharibshahian, M.; Sabouri, L.; Varzandeh, M.; Rezaei, N. Recent advances in regenerative medicine strategies for cancer treatment. Biomed. Pharmacother. 2021, 141, 21.
- Hutmacher, D.W.; Horch, R.E.; Loessner, D.; Rizzi, S.; Sieh, S.; Reichert, J.C.; Clements, J.A.; Beier, J.P.; Arkudas, A.; Bleiziffer, O.; et al. Translating tissue engineering technology platforms into cancer research. J. Cell. Mol. Med. 2009, 13, 1417–1427.
- Goliwas, K.F.; Richter, J.R.; Pruitt, H.C.; Araysi, L.M.; Anderson, N.R.; Samant, R.S.; Lobo-Ruppert, S.M.; Berry, J.L.; Frost, A.R. Methods to Evaluate Cell Growth, Viability, and Response to Treatment in a Tissue Engineered Breast Cancer Model. Sci. Rep. 2017, 7, 14.
- Akerkouch, L.; Jasuja, H.; Katti, K.; Katti, D.; Le, T. The Influence of Fluid Shear Stress on Bone and Cancer Cells Proliferation and Distribution. Ann. Biomed. Eng. 2023, 51, 1199–1215.
- Jasuja, H.; Jaswandkar, S.V.; Katti, D.R.; Katti, K.S. Interstitial fluid flow contributes to prostate cancer invasion and migration to bone; study conducted using a novel horizontal flow bioreactor. Biofabrication 2023, 15, 025017.
- Jasuja, H.; Kar, S.; Katti, D.R.; Katti, K. Perfusion bioreactor enabled fluid-derived shear stress conditions for novel bone metastatic prostate cancer testbed. Biofabrication 2021, 13, 035004.
- Pradhan, S.; Sperduto, J.L.; Farino, C.J.; Slater, J.H. Engineered In Vitro Models of Tumor Dormancy and Reactivation. J. Biol. Eng. 2018, 12, 19.
- Montagner, M.; Sahai, E. In vitro Models of Breast Cancer Metastatic Dormancy. Front. Cell Dev. Biol. 2020, 8, 37.
- Adamowicz, J.; Kluth, L.A.; Pokrywczynska, M.; Drewa, T.A. European Assoc Urology Young, Tissue Engineering and Its Potential to Reduce Prostate Cancer Treatment Sequelae-Narrative Review. Front. Surg. 2021, 8, 11.
- Valderrama-Illana, P.; Oliveira, A.C.; Arrabal-Polo, M.A. Tissue engineering in reconstructive urological treatment of penile structures. Rev. Int. Androl. 2014, 12, 71–75.
- Tan, Q.; Liu, R.J.; Chen, X.K.; Wu, J.X.; Pan, Y.G.; Lu, S.; Weder, W.; Luo, Q. Clinic application of tissue engineered bronchus for lung cancer treatment. J. Thorac. Dis. 2017, 9, 22–29.
- Hou, Y.H.; Wang, W.G.; Bartolo, P. Application of additively manufactured 3D scaffolds for bone cancer treatment: A review. Bio-Des. Manuf. 2022, 5, 556–579.
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249.
- Sharifi, M.; Bai, Q.; Babadaei, M.M.N.; Chowdhury, F.; Hassan, M.; Taghizadeh, A.; Derakhshankhah, H.; Khan, S.; Hasan, A.; Falahati, M. 3D bioprinting of engineered breast cancer constructs for personalized and targeted cancer therapy. J. Control. Release 2021, 333, 91–106.
- Qiao, H.; Tang, T. Engineering 3D approaches to model the dynamic microenvironments of cancer bone metastasis. Bone Res. 2018, 6, 3.
- Marlow, R.; Honeth, G.; Lombardi, S.; Cariati, M.; Hessey, S.; Pipili, A.; Mariotti, V.; Buchupalli, B.; Foster, K.; Bonnet, D.; et al. A novel model of dormancy for bone metastatic breast cancer cells. Cancer Res. 2013, 73, 6886.
- McGrath, J.; Panzica, L.; Ransom, R.; Withers, H.G.; Gelman, I.H. Identification of Genes Regulating Breast Cancer Dormancy in 3D Bone Endosteal Niche Cultures. Mol. Cancer Res. 2019, 17, 860–869.
- James-Bhasin, M.; Siegel, P.M.; Nazhat, S.N. A Three-Dimensional Dense Collagen Hydrogel to Model Cancer Cell/Osteoblast Interactions. J. Funct. Biomater. 2018, 9, 72.
- Cox, R.F.; Jenkinson, A.; Pohl, K.; O’Brien, F.J.; Morgan, M.P. Osteomimicry of Mammary Adenocarcinoma Cells In Vitro; Increased Expression of Bone Matrix Proteins and Proliferation within a 3D Collagen Environment. PLoS ONE 2012, 7, e41679.
- Bersini, S.; Jeon, J.S.; Dubini, G.; Arrigoni, C.; Chung, S.; Charest, J.L.; Moretti, M.; Kamm, R.D. A microfluidic 3D in vitro model for specificity of breast cancer metastasis to bone. Biomaterials 2014, 35, 2454–2461.
- Hao, S.J.; Ha, L.R.; Cheng, G.; Wan, Y.; Xia, Y.Q.; Sosnoski, D.M.; Mastro, A.M.; Zheng, S.Y. A Spontaneous 3D Bone-On-a-Chip for Bone Metastasis Study of Breast Cancer Cells. Small 2018, 14, 10.
- Mancuso, E.; Shah, L.; Jindal, S.; Serenelli, C.; Tsikriteas, Z.M.; Khanbareh, H.; Tirella, A. Additively manufactured BaTiO3 composite scaffolds: A novel strategy for load bearing bone tissue engineering applications. Mater. Sci. Eng. C Mater. Biol. Appl. 2021, 126, 112192.
- Xiong, Q.S.; Zhang, N.Z.; Zhang, M.M.; Wang, M.; Wang, L.Z.; Fan, Y.B.; Lin, C.Y. Engineer a pre-metastatic niched microenvironment to attract breast cancer cells by utilizing a 3D printed polycaprolactone/nano-hydroxyapatite osteogenic scaffold—An in vitro model system for proof of concept. J. Biomed. Mater. Res. Part B Appl. Biomater. 2022, 110, 1604–1614.
- Xiong, Q.S.; Wang, M.; Liu, J.L.; Lin, C.Y. Breast Cancer Cells Metastasize to the Tissue-Engineered Premetastatic Niche by Using an Osteoid-Formed Polycaprolactone/Nanohydroxyapatite Scaffold. Comput. Math. Methods Med. 2021, 2021, 13.
- Aguado, B.A.; Gaffe, J.R.; Nanavati, D.; Rao, S.S.; Bushnell, G.G.; Azarin, S.M.; Shea, L.D. Extracellular matrix mediators of metastatic cell colonization characterized using scaffold mimics of the pre-metastatic niche. Acta Biomater. 2016, 33, 13–24.
- Guiro, K.; Patel, S.A.; Greco, S.J.; Rameshwar, P.; Arinzeh, T.L. Investigating Breast Cancer Cell Behavior Using Tissue Engineering Scaffolds. PLoS ONE 2015, 10, 22.
- Kar, S.; Molla, M.D.S.; Katti, D.R.; Katti, K.S. Tissue-engineered nanoclay based 3D in vitro breast cancer model for studying breast cancer metastasis to bone. J. Tissue Eng. Regen. Med. 2018, 13, 119–130.
- Jasuja, H.; Mohammadi, F.S.; Kim, J.; Gaba, A.; Katti, D.R.; Katti, K.S. Patient-Derived Breast Cancer Bone Metastasis In Vitro Model Using Bone-Mimetic Nanoclay Scaffolds. J. Tissue Eng. Regen. Med. 2023, 2023, 10.
- Kar, S.; Katti, D.R.; Katti, K.S. Fourier transform infrared spectroscopy based spectral biomarkers of metastasized breast cancer progression. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2019, 208, 85–96.
- Kar, S.; Katti, D.R.; Katti, K.S. Evaluation of quasi-static and dynamic nanomechanical properties of bone-metastatic breast cancer cells using a nanoclay cancer testbed. Sci. Rep. 2021, 11, 3096.
- Kar, S.; Katti, D.R.; Katti, K.S. Bone interface modulates drug resistance in breast cancer bone metastasis. Colloids Surf. B Biointerfaces 2020, 195, 10.
- Kar, S.; Jasuja, H.; Katti, D.R.; Katti, K.S. Wnt/beta-Catenin Signaling Pathway Regulates Osteogenesis for Breast Cancer Bone Metastasis: Experiments in an In Vitro Nanoclay Scaffold Cancer Testbed. ACS Biomater. Sci. Eng. 2020, 6, 2600–2611.
- Zhou, X.; Zhu, W.; Nowicki, M.; Miao, S.; Cui, H.T.; Holmes, B.; Glazer, R.I.; Zhang, L.G. 3D Bioprinting a Cell-Laden Bone Matrix for Breast Cancer Metastasis Study. ACS Appl. Mater. Interfaces 2016, 8, 30017–30026.
- Moreau, J.E.; Anderson, K.; Mauney, J.R.; Nguyen, T.; Kaplan, D.L.; Rosenblatt, M. Tissue-engineered bone serves as a target for metastasis of human breast cancer in a mouse model. Cancer Res. 2007, 67, 10304–10308.
- Seib, F.P.; Berry, J.E.; Shiozawa, Y.; Taichman, R.S.; Kaplan, D.L. Tissue engineering a surrogate niche for metastatic cancer cells. Biomaterials 2015, 51, 313–319.
- Kwon, H.; Kim, H.J.; Rice, W.L.; Subramanian, B.; Park, S.H.; Georgakoudi, I.; Kaplan, D.L. Development of an in vitro model to study the impact of BMP-2 on metastasis to bone. J. Tissue Eng. Regen. Med. 2010, 4, 590–599.
- Díaz, E.C.G.; Tai, M.; Monette, C.E.F.; Wu, J.Y.; Yang, F. Spatially patterned 3D model mimics key features of cancer metastasis to bone. Biomaterials 2023, 299, 122163.
- Angeloni, V.; Contessi, N.; De Marco, C.; Bertoldi, S.; Tanzi, M.C.; Daidone, M.G.; Fare, S. Polyurethane foam scaffold as in vitro model for breast cancer bone metastasis. Acta Biomater. 2017, 63, 306–316.
- Pathi, S.P.; Kowalczewski, C.; Tadipatri, R.; Fischbach, C. A Novel 3-D Mineralized Tumor Model to Study Breast Cancer Bone Metastasis. PLoS ONE 2010, 5, 10.
- Pathi, S.P.; Lin, D.D.W.; Dorvee, J.R.; Estroff, L.A.; Fischbach, C. Hydroxyapatite nanoparticle-containing scaffolds for the study of breast cancer bone metastasis. Biomaterials 2011, 32, 5112–5122.
- Zhu, W.; Wang, M.; Fu, Y.B.; Castro, N.J.; Fu, S.W.; Zhang, L.G. Engineering a biomimetic three-dimensional nanostructured bone model for breast cancer bone metastasis study. Acta Biomater. 2015, 14, 164–174.
- Kolb, A.D.; Bussard, K.M. The Bone Extracellular Matrix as an Ideal Milieu for Cancer Cell Metastases. Cancers 2019, 11, 1020.
- Sotome, S.; Ae, K.; Okawa, A.; Ishizuki, M.; Morioka, H.; Matsumoto, S.; Nakamura, T.; Abe, S.; Beppu, Y.; Shinomiya, K. Efficacy and safety of porous hydroxyapatite/type 1 collagen composite implantation for bone regeneration: A randomized controlled study. J. Orthop. Sci. 2016, 21, 373–380.
- Maehara, H.; Sotome, S.; Yoshii, T.; Torigoe, I.; Kawasaki, Y.; Sugata, Y.; Yuasa, M.; Hirano, M.; Mochizuki, N.; Kikuchi, M.; et al. Repair of large osteochondral defects in rabbits using porous hydroxyapatite/collagen (HAp/Col) and fibroblast growth factor-2 (FGF-2). J. Orthop. Res. 2010, 28, 677–686.
- Tsuchiya, A.; Sotome, S.; Asou, Y.; Kikuchi, M.; Koyama, Y.; Ogawa, T.; Tanaka, J.; Shinomiya, K. Effects of pore size and implant volume of porous hydroxyapatite/collagen (HAp/Col) on bone formation in a rabbit bone defect model. J. Med. Dent. Sci. 2008, 55, 91–99.
- Matsumoto, R.; Yoshii, T.; Egawa, S.; Hashimoto, M.; Hirai, T.; Inose, H.; Oh, Y.; Fujita, K.; Okawa, A.; Sotome, S. Local Suppression Effect of Paclitaxel-Impregnated Hydroxyapatite/Collagen on Breast Cancer Bone Metastasis in a Rat Model. Spine Surg. Relat. Res. 2022, 6, 294–302.
- Palamà, I.E.; Arcadio, V.; D’Amone, S.; Biasiucci, M.; Gigli, G.; Cortese, B. Therapeutic PCL scaffold for reparation of resected osteosarcoma defect. Sci. Rep. 2017, 7, 12.
- Thibaudeau, L.; Taubenberger, A.V.; Holzapfel, B.M.; Quent, V.M.; Fuehrmann, T.; Hesami, P.; Brown, T.D.; Dalton, P.D.; Power, C.A.; Hollier, B.G.; et al. A tissue-engineered humanized xenograft model of human breast cancer metastasis to bone. Dis. Models Mech. 2014, 7, 299–309.
- Ambre, A.H.; Katti, D.R.; Katti, K.S. Biomineralized hydroxyapatite nanoclay composite scaffolds with polycaprolactone for stem cell-based bone tissue engineering. J. Biomed. Mater. Res. Part A 2015, 103, 2077–2101.
- Cui, H.T.; Esworthy, T.; Zhou, X.; Hann, S.Y.; Glazer, R.I.; Li, R.; Zhang, L.G. Engineering a Novel 3D Printed Vascularized Tissue Model for Investigating Breast Cancer Metastasis to Bone. Adv. Healthc. Mater. 2020, 9, 11.
- Vepari, C.; Kaplan, D.L. Silk as a biomaterial. Prog. Polym. Sci. 2007, 32, 991–1007.
- Thibaudeau, L.; Quent, V.M.; Holzapfel, B.M.; Taubenberger, A.V.; Straub, M.; Hutmacher, D.W. Mimicking breast cancer-induced bone metastasis in vivo: Current transplantation models and advanced humanized strategies. Cancer Metastasis Rev. 2014, 33, 721–735.
- Wong, S.K.; Mohamad, N.-V.; Giaze, T.R.; Chin, K.-Y.; Mohamed, N.; Ima-Nirwana, S. Prostate Cancer and Bone Metastases: The Underlying Mechanisms. Int. J. Mol. Sci. 2019, 20, 2587.
- Osawa, T.; Wang, W.; Dai, J.; Keller, E.T. Macrofluidic recirculating model of skeletal metastasis. Sci. Rep. 2019, 9, 14979.
- Koutsilieris, M.; Sourla, A.; Pelletier, G.; Doillon, C.J. Three-dimensional type I collagen gel system for the study of osteoblastic metastases produced by metastatic prostate cancer. J. Bone Miner. Res. 1994, 9, 1823–1832.
- Fitzgerald, K.A.; Guo, J.; Tierney, E.G.; Curtin, C.M.; Malhotra, M.; Darcy, R.; O’Brien, F.J.; O’Driscoll, C.M. The use of collagen-based scaffolds to simulate prostate cancer bone metastases with potential for evaluating delivery of nanoparticulate gene therapeutics. Biomaterials 2015, 66, 53–66.
- Ribeiro, N.; Sousa, S.R.; Monteiro, F.J. A 3D synthetic model of collagen fibers with nanohydroxyapatite grafted with SPARC for bone regeneration and prevention of cancer related bone metastasis. J. Tissue Eng. Regen. Med. 2012, 6, 165.
- Cruz-Neves, S.; Ribeiro, N.; Graca, I.; Jeronimo, C.; Sousa, S.R.; Monteiro, F.J. Behavior of prostate cancer cells in a nanohydroxyapatite/collagen bone scaffold. J. Biomed. Mater. Res. Part A 2017, 105, 2035–2046.
- Ribeiro, N.; Costa-Pinheiro, P.; Henrique, R.; Gomez-Lazaro, M.; Pereira, M.P.; Mansur, A.A.P.; Mansur, H.S.; Jerónimo, C.; Sousa, S.R.; Monteiro, F.J. Comprehensive Analysis of Secreted Protein, Acidic and Rich in Cysteine in Prostate Carcinogenesis: Development of a 3D Nanostructured Bone-Like Model. J. Biomed. Nanotechnol. 2016, 12, 1667–1678.
- Evans, J.C.; Malhotra, M.; Fitzgerald, K.A.; Guo, J.; Cronin, M.F.; Curtin, C.M.; O’Brien, F.J.; Darcy, R.; O’Driscoll, C.M. Formulation and Evaluation of Anisamide-Targeted Amphiphilic Cyclodextrin Nanoparticles to Promote Therapeutic Gene Silencing in a 3D Prostate Cancer Bone Metastases Model. Mol. Pharm. 2017, 14, 42–52.
- Sieh, S.; Lubik, A.A.; Clements, J.A.; Nelson, C.C.; Hutmacher, D.W. Interactions between human osteoblasts and prostate cancer cells in a novel 3D in vitro model. Organogenesis 2010, 6, 181–188.
- Hesami, P.; Holzapfel, B.M.; Taubenberger, A.; Roudier, M.; Fazli, L.; Sieh, S.; Thibaudeau, L.; Gregory, L.S.; Hutmacher, D.W.; Clements, J.A. A humanized tissue-engineered in vivo model to dissect interactions between human prostate cancer cells and human bone. Clin. Exp. Metastasis 2014, 31, 435–446.
- Zhou, Y.; Chen, F.; Ho, S.T.; Woodruff, M.A.; Lim, T.M.; Hutmacher, D.W. Combined marrow stromal cell-sheet techniques and high-strength biodegradable composite scaffolds for engineered functional bone grafts. Biomaterials 2007, 28, 814–824.
- Bock, N.; Shokoohmand, A.; Kryza, T.; Röhl, J.; Meijer, J.; Tran, P.A.; Nelson, C.C.; Clements, J.A.; Hutmacher, D.W. Engineering osteoblastic metastases to delineate the adaptive response of androgen-deprived prostate cancer in the bone metastatic microenvironment. Bone Res. 2019, 7, 13.
- Hartman, O.; Zhang, C.; Adams, E.L.; Farach-Carson, M.C.; Petrelli, N.J.; Chase, B.D.; Rabolt, J.E. Biofunctionalization of electrospun PCL-based scaffolds with perlecan domain IV peptide to create a 3-D pharmacokinetic cancer model. Biomaterials 2010, 31, 5700–5718.
- Katti, K.S.; Molla, M.D.S.; Karandish, F.; Haldar, M.K.; Mallik, S.; Katti, D.R. Sequential culture on biomimetic nanoclay scaffolds forms three-dimensional tumoroids. J. Biomed. Mater. Res. Part A 2016, 104, 1591–1602.
- Molla, M.D.S.; Katti, D.R.; Iswara, J.; Venkatesan, R.; Paulmurugan, R.; Katti, K.S. Prostate Cancer Phenotype Influences Bone Mineralization at Metastasis: A Study Using an In Vitro Prostate Cancer Metastasis Testbed. JBMR Plus 2020, 4, e10256.
- Shokoohmand, A.; Ren, J.; Baldwin, J.; Atack, A.; Shafiee, A.; Theodoropoulos, C.; Wille, M.L.; Tran, P.A.; Bray, L.J.; Smith, D.; et al. Microenvironment engineering of osteoblastic bone metastases reveals osteomimicry of patient-derived prostate cancer xenografts. Biomaterials 2019, 220, 17.
- Bäcker, A.; Erhardt, O.; Wietbrock, L.; Schel, N.; Göppert, B.; Dirschka, M.; Abaffy, P.; Sollich, T.; Cecilia, A.; Gruhl, F.J. Silk scaffolds connected with different naturally occurring biomaterials for prostate cancer cell cultivation in 3D. Biopolymers 2017, 107, 70–79.
- Dozzo, A.; Chullipalliyalil, K.; McAuliffe, M.; O’Driscoll, C.M.; Ryan, K.B. Nano-Hydroxyapatite/PLGA Mixed Scaffolds as a Tool for Drug Development and to Study Metastatic Prostate Cancer in the Bone. Pharmaceutics 2023, 15, 242.
- Gracia, E.; Mancini, A.; Colapietro, A.; Mateo, C.; Gracia, I.; Festuccia, C.; Carmona, M. Impregnation of Curcumin into a Biodegradable (Poly-lactic-co-glycolic acid, PLGA) Support, to Transfer Its Well Known In Vitro Effect to an In Vivo Prostate Cancer Model. Nutrients 2019, 11, 2312.
- Sieh, S.; Taubenberger, A.V.; Lehman, M.L.; Clements, J.A.; Nelson, C.C.; Hutmacher, D.W. Paracrine interactions between LNCaP prostate cancer cells and bioengineered bone in 3D in vitro culture reflect molecular changes during bone metastasis. Bone 2014, 63, 121–131.
- Habbit, N.L.; Anbiah, B.; Anderson, L.; Suresh, J.; Hassani, I.; Eggert, M.; Brannen, A.; Davis, J.; Tian, Y.; Prabhakarpandian, B.; et al. Tunable three-dimensional engineered prostate cancer tissues for in vitro recapitulation of heterogeneous in vivo prostate tumor stiffness. Acta Biomater. 2022, 147, 73–90.
- Chen, C.-H.; Kuo, C.-Y.; Chen, S.-H.; Mao, S.-H.; Chang, C.-Y.; Shalumon, K.T.; Chen, J.-P. Thermosensitive Injectable Hydrogel for Simultaneous Intraperitoneal Delivery of Doxorubicin and Prevention of Peritoneal Adhesion. Int. J. Mol. Sci. 2018, 19, 1375.
- Wang, Y.; Gong, C.; Yang, L.; Wu, Q.; Shi, S.; Shi, H.; Qian, Z.; Wei, Y. 5-FU-hydrogel inhibits colorectal peritoneal carcinomatosis and tumor growth in mice. BMC Cancer 2010, 10, 402.
- Tian, X.; Werner, M.E.; Roche, K.C.; Hanson, A.D.; Foote, H.P.; Yu, S.K.; Warner, S.B.; Copp, J.A.; Lara, H.; Wauthier, E.L.; et al. Organ-specific metastases obtained by culturing colorectal cancer cells on tissue-specific decellularized scaffolds. Nat. Biomed. Eng. 2018, 2, 443–452.
- D’Angelo, E.; Natarajan, D.; Sensi, F.; Ajayi, O.; Fassan, M.; Mammano, E.; Pilati, P.; Pavan, P.; Bresolin, S.; Preziosi, M.; et al. Patient-Derived Scaffolds of Colorectal Cancer Metastases as an Organotypic 3D Model of the Liver Metastatic Microenvironment. Cancers 2020, 12, 364.
- Chen, H.J.; Wei, Z.; Sun, J.; Bhattacharya, A.; Savage, D.J.; Serda, R.; Mackeyev, Y.; Curley, S.A.; Bu, P.; Wang, L.; et al. A recellularized human colon model identifies cancer driver genes. Nat. Biotechnol. 2016, 34, 845–851.
- Piccoli, M.; D’Angelo, E.; Crotti, S.; Sensi, F.; Urbani, L.; Maghin, E.; Burns, A.; De Coppi, P.; Fassan, M.; Rugge, M.; et al. Decellularized colorectal cancer matrix as bioactive microenvironment for in vitro 3D cancer research. J. Cell. Physiol. 2018, 233, 5937–5948.
- VandenHeuvel, S.N.; Farris, H.A.; Noltensmeyer, D.A.; Roy, S.; Donehoo, D.A.; Kopetz, S.; Haricharan, S.; Walsh, A.J.; Raghavan, S. Decellularized organ biomatrices facilitate quantifiable in vitro 3D cancer metastasis models. Soft Matter 2022, 18, 5791–5806.
- Nietzer, S.; Baur, F.; Sieber, S.; Hansmann, J.; Schwarz, T.; Stoffer, C.; Häfner, H.; Gasser, M.; Waaga-Gasser, A.M.; Walles, H.; et al. Mimicking Metastases Including Tumor Stroma: A New Technique to Generate a Three-Dimensional Colorectal Cancer Model Based on a Biological Decellularized Intestinal Scaffold. Tissue Eng. Part C Methods 2016, 22, 621–635.
- Zhong, J.C.; Zhang, Y.J.; Chen, J.F.; Huang, R.Y.; Yang, Y.K.; Chen, H.X.; Huang, Y.; Tan, W.H.; Tan, Z.K. In Vitro Study of Colon Cancer Cell Migration Using E-Jet 3D Printed Cell Culture Platforms. Macromol. Biosci. 2018, 18, 1800205.
- Barnett, K.T.; Fokum, F.D.; Malafa, M.P. Vitamin E Succinate Inhibits Colon Cancer Liver Metastases. J. Surg. Res. 2002, 106, 292–298.
- Nie, S.; Zhou, J.; Bai, F.; Jiang, B.; Chen, J.; Zhou, J. Role of Endothelin A Receptor in Colon Cancer Metastasis: In Vitro and In Vivo Evidence. Mol. Carcinog. 2014, 53, E85–E91.
- Liu, J.-J.; Li, L.-Z.; Xu, P. Upregulation of TRPM8 can promote the colon cancer liver metastasis through mediating Akt/GSK-3 signal pathway. Biotechnol. Appl. Biochem. 2022, 69, 230–239.
- Abedini, F.; Hosseinkhani, H.; Ismail, M.; Domb, A.J.; Omar, A.R.; Chong, P.P.; Hong, P.-D.; Yu, D.-S.; Farber, I.-Y. Cationized dextran nanoparticle-encapsulated CXCR4-siRNA enhanced correlation between CXCR4 expression and serum alkaline phosphatase in a mouse model of colorectal cancer. Int. J. Nanomed. 2012, 7, 4159–4168.
- Furbo, S.; Urbano, P.C.; Raskov, H.H.; Troelsen, J.T.; Fiehn, A.-M.K.; Gögenur, I. Use of Patient-Derived Organoids as a Treatment Selection Model for Colorectal Cancer: A Narrative Review. Cancers 2022, 14, 1069.
- Sarvestani, S.K.; DeHaan, R.K.; Miller, P.G.; Bose, S.; Shen, X.L.; Shuler, M.L.; Huang, E.H. A Tissue Engineering Approach to Metastatic Colon Cancer. iScience 2020, 23, 101719.
- Yachida, S.; White, C.M.; Naito, Y.; Zhong, Y.; Brosnan, J.A.; Macgregor-Das, A.M.; Morgan, R.A.; Saunders, T.; Laheru, D.A.; Herman, J.M.; et al. Clinical Significance of the Genetic Landscape of Pancreatic Cancer and Implications for Identification of Potential Long-term Survivors. Clin. Cancer Res. 2012, 18, 6339–6347.
- Mallya, K.; Gautam, S.K.; Aithal, A.; Batra, S.K.; Jain, M. Modeling pancreatic cancer in mice for experimental therapeutics. Biochim. Biophys. Acta Rev. Cancer 2021, 1876, 18.
- Qu, J.J.; Kalyani, F.S.; Liu, L.; Cheng, T.L.; Chen, L.J. Tumor organoids: Synergistic applications; current challenges, and future prospects in cancer therapy. Cancer Commun. 2021, 41, 1331–1353.
- Sekine, K. Human Organoid and Supporting Technologies for Cancer and Toxicological Research. Front. Genet. 2021, 12, 7.
- Miquel, M.; Zhang, S.M.; Pilarsky, C. Pre-clinical Models of Metastasis in Pancreatic Cancer. Front. Cell Dev. Biol. 2021, 9, 21.
- Al-Akkad, W.; Acedo, P.; Vilia, M.G.; Frenguelli, L.; Ney, A.; Rodriguez-Hernandez, I.; Labib, P.L.; Tamburrino, D.; Spoletini, G.; Hall, A.R.; et al. Tissue-Specific Human Extracellular Matrix Scaffolds Promote Pancreatic Tumour Progression and Chemotherapy Resistance. Cells 2022, 11, 3652.
- Wishart, G.; Gupta, P.; Nisbet, A.; Schettino, G.; Velliou, E. On the Evaluation of a Novel Hypoxic 3D Pancreatic Cancer Model as a Tool for Radiotherapy Treatment Screening. Cancers 2021, 13, 6080.
More
Information
Subjects:
Cell & Tissue Engineering
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
449
Revisions:
2 times
(View History)
Update Date:
05 Mar 2024
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No