Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Haneesh Jasuja and Version 2 by Camila Xu.
Tissue engineering is a promising field for regenerative medicine that is likely to be able to provide rehabilitation procedures to patients who have undergone surgeries, such as mastectomy and other reconstructive procedures. Another important use of tissue engineering has emerged recently that involves the development of realistic and robust in vitro models of cancer metastasis, to aid in drug discovery and new metastasis therapeutics, as well as evaluate cancer biology at metastasis.
- tissue engineering
- cancer
- metastasis
- in vitro models
- 3D models
1. Introduction
Cancer is emerging as a leading cause of premature death worldwide [1]. Globally, the World Health Organization reported 9.6 million deaths in 2018, making cancer the second leading cause of death worldwide. The large global economic burden of cancer from 2020 to 2050 was estimated to be USD 25.2 trillion [2]. Metastasis remains the primary cause of death due to cancer [3]. In a 2022 study, it was estimated that 623,405 people were living with metastatic cancers or metastatic melanoma in the US, and that number is expected to increase to 693,452 by the year 2025 [4]. A 2007 study reported that the economic burden for patients with metastatic bone diseases is USD 12.6 billion. This number represents 17% of the total medical burden estimated by the National Institutes of Health [5]. A more recent 2022 study estimated that the bone metastasis burden has increased to 20% of the overall oncology costs [6]. Alarmingly, most survivors with metastatic cancer of various types, except melanoma, have a life expectance of less than five years [4]. Palliative treatments are often the only course of treatment for metastasis. For example, at bone metastasis, palliative treatment includes the use of drugs, such as bisphosphonates and Denosumab, which are used to stabilize skeletal issues [7][8][7,8]. The complex cascade of biochemical and resulting pathological events that lead to metastasis to bone is still mostly unknown. This knowledge is further hampered by the lack of appropriate and relevant model systems for testing new drugs and therapies. In vitro models mimicking bone metastasis are much needed for this purpose.
All types of cancers can spread. The mechanisms of spreading cancer are varied. These range from cancer invading normal tissue in its proximity, traveling through either the lymphatic system or blood vessels to other parts of the body, attaching to invading blood vessel walls and forming tumors, to the growth of new blood vessels that enable metastatic tumor growth. Different cancers have the propensity to metastasize to specific locations in the body, e.g., breast cancer and prostate cancer tend to spread to the bones, and colon cancer and pancreatic cancer spread to the liver, as shown in Figure 1. Metastasis is the cause of most patient deaths, yet the mechanisms of metastasis remain primarily unknown. The process is fundamentally described as a two-step process, with the initial dislocation of cancer from its primary site and transportation of cells to a distant site through blood and lymph systems, and the phenomenon of recolonization of cancer at the remote site [9].
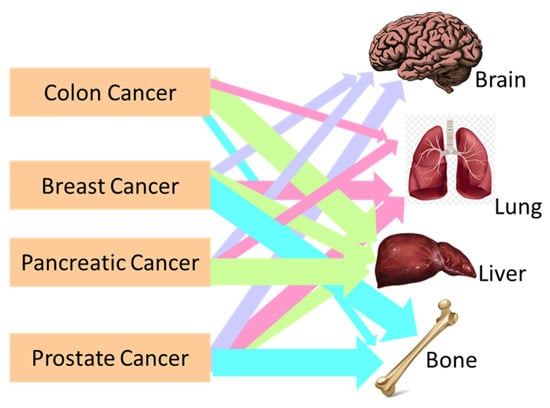
Figure 1. Schematic representation showing the metastasis locations of colon, breast, pancreatic, and prostate cancer in the human body.
Tumorigenesis has been traditionally studied in 2D cultures of cancer cells. Although many characteristics of cancer cells have been well explored using these 2D cell culture systems, they do not replicate the realistic tumor microenvironment. The 3D culture systems have been increasingly gaining attention for the past few years. These systems include 3D spheroids of cancer cells. Extensive studies report using 3D spheroid models of cancer [10], and their important use in screening drugs. The spheroids are fundamentally clusters of cancer cells that are grown either in suspension or embedded in a matrix. Although the spheroids have 3D structures, they do not accurately capture the mechanical, biological, and chemical characteristics of the metastasis site. While extensive studies are undertaken on the development of the complex chemo-physio-mechanical analogs of the primary site of cancer [11], efforts in producing accurate 3D models of metastasis are rare, as they do not represent the migration characteristics of metastasis well.
Further, transwell-based assays are useful to assess the inherent migratory and invasion characteristics of cancer cells [12][13][14][12,13,14]. Migration is an important characteristic of cancer cells that are likely to arrive at the metastatic site—they do not capture the behavior of the cells at metastasis. Several detailed reviews illustrate the important use of transwell assay-based models [15]. To develop a deeper understanding of the process of cancer metastasis and to be able to aid in the development of effective therapies for metastasis prevention and cure, in vitro and in vivo models are extensively investigated. While in vivo models can capture the complexity of living systems and are generally considered useful models for studying primary cancer types, they often fail to develop into cancer metastasis.
Robust in vitro models present themselves as a fast, inexpensive evaluation route for the study of cancer metastasis. The extremely high-cost and time-intensive nature of PDX models further necessitates robust in vitro systems that effectively represent cancer and metastasis stages. Many in vitro models have been developed for capturing various aspects of tumor growth, proliferation, invasion into tissues, intra and extravasation through blood vessels, angiogenic characteristics, and also delivery of drugs and their efficacies [15]. The source of cancer cells, either commercial or patient-derived origins, for seeding the in vitro models is just as important. Many commercial cell lines of several cancer types are easily available and are used to study tumor cell biology and proliferation [16][17][16,17]. The molecular profiles and various characterizations of human cancer cell lines are available in the Cancer Line Encyclopedia [10][18][19][20][10,18,19,20]. Often, the spectrum of variabilities within a particular cancer type is very vast, and the commercial cell lines are not able to capture such a wide spectrum of variabilities and, thus, achieve limited clinical relevance for patients [21]. Patient-derived cell lines are thus increasingly popular as a source in the development of in vitro cancer models. While cell lines from patients, even with advanced cancer stages, are available [22], the availability of cancer cell lines from metastasized tissue types is rare.
2. Tissue Engineering
Tissue engineering provides an important platform for the design of site-specific structural and biological similarity of metastasis. Tissue engineering is an interdisciplinary field that aims to develop new tissue and organ substitutes using biological sciences and engineering. The primary components of tissue engineering include biomaterials and scaffolds, cells, and regulatory signals, such as the use of growth factors (Figure 2).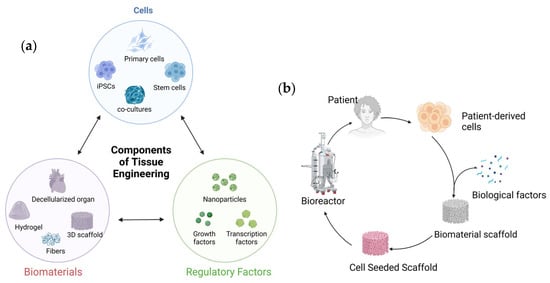
Figure 2. Schematic showing tissue engineering: (a) three important components of tissue engineering and (b) the tissue engineering process.
3. Cancer Metastasis 3D In Vitro Models
3.1. Breast Cancer Metastasis Models
Female breast cancer is reported as the most common cancer and the fourth highest in mortality due to cancer [55]. Cancer originating in the breast can metastasize to the lungs, brain, and bone. Therapies and treatments for bone metastasis of breast cancer are primarily palliative. Metastasis of breast cancer to bone is not curable. The blood-induced mechanical stresses and cancer cell–host (bone) interactions are the major players in bone metastasis of breast cancer. Various material systems are used to develop scaffolds that mimic bone sites. While extensive studies remain underway on the design of primary breast cancer with co-cultures of various cells [56], recent works also report tissue-engineered bone metastasis models. Mimicking the complex dynamic environment of the bone site on arrival of the cancer cells is a useful and valuable approach currently being investigated [57]. Many unique material models have been used to develop tissue-engineered bone structures to evaluate the bone metastasis of breast cancer. These models use a variety of polymeric scaffolds with and without infiltration with bone-forming minerals. A detailed overview of the various materials used to develop the bone niche and cell lines investigated is shown in Table 1. Each material model is tested with in vitro experimentations that validate some hallmarks of breast/prostate cancer colonization to bone.Table 1.
List of materials and cells for developing the bone niche for breast cancer bone metastasis models.
3.3. Colon Cancer Metastasis Models
Worldwide, colon cancer remains the fourth most common cancer and the third highest cause of death [55]. Colorectal tumor cells metastasize to the liver and lungs through hematogenous processes or lymphatics. Several attempts to use biomaterials have been made toward controlled drug delivery to colorectal cancer [116][117][116,117]. Metastasis is the most common cause of death due to colorectal cancer, with the liver being the most common metastasis site. Due to the high number of fatalities due to colorectal cancer metastasis, there is interest in developing 3D models of metastasis. A detailed description of the material systems and 3D models used to create the metastatic niche of colon cancer is shown in Table 3.Table 3.
List of materials and cells for developing the colon cancer metastasis models.
| Material Class | Material Form | Cell Types | References | ||||
|---|---|---|---|---|---|---|---|
| Decellularized tissue scaffolds | Liver decellularized scaffolds seeded with colorectal cancer cells in mice models | HT-29, CRC119, SW480, and Caco2 | [118] | ||||
| Dense collagen hydrogel | MDA-MB-231 breast cancer cells and MC3T3-E1 pre-osteoblasts | [60] | |||||
| Patient-derived decellularized colon tissue | HT-29 | [119][120][121][119,120,121] | Collagen-glycosaminoglycan (GAG) | Murine mammary adenocarcinoma 4T1 cells | [61] | ||
| Decellularized porcine livers to generate scaffolds | HCT116 | [122] | Collagen gel seeded with osteo-differentiated human bone marrow-derived mesenchymal stem cells | MDA-MB-231 human breast cancer cells | [62] | ||
| Decellularized porcine small intestine submucosa + mucosa scaffolds | SW480 and SW480 colon cancer cells | [123] | Heavily mineralized collagen fibers for a bone-on-a-chip | A co-culture of metastatic breast cancer cells and osteoblasts GFP-labeled metastatic breast cancer cell line, MDA-MB-231GFP cells, and metastasis-suppressed breast cancer cell line, MDA-MB-231-BRMS1GFP cells |
|||
| PLGA | E-jet 3D printing of PLGA | HCT-116 and LoVo human colon cancer cell lines, and p53-null (knockout) human colon cancer cell line (HCT-116 p53−/− | [63] | ||||
| ) | [ | 124 | ] | 3D Collagen matrix (GELFOAM), seeded with endothelial, bone marrow stromal cells, and fetal osteoblasts | MDA-MB-231, BoM1833 | [59] | |
| PCL | 3D-printed scaffolds made of Piezo-electro-ceramics, such as BaTiO3 with polycaprolactone | In vitro models of MDA MB231 breast cancer cell migration and invasion studies | [41][64][41,64] | ||||
| 3D-printed polycaprolactone (PCL) scaffolds with dispersed HAP | This in vitro model shows migration of MDA-MB-231, MCF-7, and MDA-MB-453 breast cancer cells toward the bone | [65][66][65,66] | |||||
| PCL scaffolds coated with fibronectin and collagen IV | Human LM2-4 cells derived from MDA-MB-231 cells and mouse 4T1 cells | [67] | |||||
| Random and aligned PCL fibers | Chemo-resistant MDA-MB-231 and T47D breast cancer cells | [68] | |||||
| PCL with nano-clay–biomimetic hydroxyapatite | MCF 7, MDA 231, patient-derived cell lines | [69][70][71][72][73][74][69,70,71,72,73,74] | |||||
| PEG | Polyethylene glycol hydrogel and nanocrystalline hydroxyapatite composite scaffolds |
MDA-MB-231 | [75] | ||||
| Silk Proteins | Fibrous proteins derived from natural fibers derived from silkworms and spiders | MDA MB 231, MCF 7 | [76][77][78][76,77,78] | ||||
| Silk protein scaffolds | Human breast cancer cells injected into the mammary fat pads of mice | [49][50][51][77][49,50,51,77] | |||||
| 3D-printed spatially layered bone tissues with gelatin to generate a layered structure of scaffold that has an outer ring composed of tissue-engineered bone and a center composed of macroporous scaffolds that host cancer cells | MDA MB 231 | [79] | |||||
| Polyurethane | Polyurethane foam scaffold | MCF7 | [80] | ||||
| PLA-PGA | Poly (lactide-co-glycolide) PLA-PGA scaffolds dispersed with nanoHAP particles | MDA-MB231 | [81][82][81,82] | ||||
| Chitosan | NanoHAP inside a chitosan gel | MDA-MB-231, MCF-7, and transfected MDA-MB-231 | [83] |
The PCL–HAP–nano-clay model was also used with patient-derived breast cancer estrogen-receptor-positive (ER+) and triple-negative (TN) breast cancer tissues to study osteolytic and osteoblastic implications of breast cancer on bone [70] as well as evaluate drug efficacies [73]. Soft gel-like material systems incorporated with nanoHAP were used for 3D-printed structures with vasculature and seeding with multiple cell types to investigate breast cancer metastasis to bone [92]. The choice of gelatin in these models is owing to the fact that gelatin is partially denatured collagen, and the biochemical properties of gelatin are similar to the organic component of bone.
Polyurethanes are important engineering polymers that have found applications in biomedical engineering due to their biocompatibility, biostability, and degradability. Polyurethane foam scaffolds are investigated as bone surrogates and used as bone metastasis models [80]. The advantage of the PU foam is the apparent highly porous architecture that mimics the trabecular bone. Breast cancer cells, MCF-7-derived tumor-initiating cells (MCFS), were used to evaluate the metastasis condition in these studies.
3.2. Prostate Cancer Metastasis Models
Prostate cancer cells also metastasize to bone, exhibiting osteomimicry, and are the subject of many investigations [40]. The interactions between the prostate cancer cells and the bone microenvironment are crucial for metastasis progression. Understanding the underlying mechanisms of metastasis of prostate cancer to bone was investigated [95]. Key bone modeling and remodeling process regulatory factors, such as -kappa B (RANK)/RANKL/OPG, the WnT pathways, growth factors, such as TGFb, and specifically, bone morphogenic proteins, are known to be intrinsically involved in the prostate cancer bone metastasis [74][95][74,95]. Macro-fluidic models to evaluate the process of metastasis were also attempted [96]. Many attempts have been made to create bone-mimetic environments, such as the bone-mimetic niche for prostate cancer metastasis. For reasons similar to those described for breast cancer metastasis to bone, polycaprolactone scaffolds are fabricated and used for bone scaffolds. Polymers such as PCL and gelatin are also extensively used in bone mimicry for developing bone metastasis models of prostate cancer. Table 2 summarizes the various polymeric, composite, and biological materials that are used in the development of tissue-engineered scaffolds to mimic the bone site of prostate cancer metastasis.Table 2.
List of materials and cells for developing the bone niche for prostate cancer bone metastasis models.
| Materials System | Material Form | Cell Types | References |
|---|---|---|---|
| Collagens | Collagen gel | Co-culture of human MG-63 osteoblast-like cells with highly metastatic human PC3 prostate cancer cells | [97] |
| Collagen-glycosaminoglycan and nanohydroxyapatite composites | PC3 and LNCaP | [98] | |
| Collagen nanofibers with nanohydroxyapatite grafted with SPARC | LNCaP | [99][100][101][99,100,101] | |
| Collagen-hydroxyapatite scaffolds | PC3 and DU145 | [102] | |
| Gelatin | 3D printing to generate a layered structure of scaffold that has an outer ring composed of tissue-engineered bone and a center composed of macroporous scaffolds that host cancer cells | PC3 | [79] |
| PCL | Medical-grade polycaprolactone–calcium phosphate (mPCL–CaP) scaffolds | PC3 and LNCaP | [103][104][105][103,104,105] |
| Medical-grade PCL: culturing primary human osteoprogenitor cells on melt electrowritten PCL scaffolds | LNCaP, C4-2B, and PC3 | [106] | |
| Electrospun PCL fibers and PCL/gelatin composite scaffolds modified with perlecan domain IV (PlnDIV) peptide | C4-2B cancer cells | [107] | |
| PCL–nano-clay–nanohydroxyapatite scaffolds | PC3 and PCa | [91][108][109][91,108,109] | |
| Tubular PCL scaffolds coated with calcium phosphate were fabricated by melt electro-writing PCL | LuCaP35 | [110] | |
| Silk Proteins | Scaffolds fabricated from silk proteins derived from Bombyx mori. | PC3 | [78] |
| Scaffolds fabricated using silk protein fibroin from Bombyx mori and recombinant spider silk protein spidroin (SSP1) with gelatin, collagen, and chitosan, indicating potential advantages | LNCaP | [111] | |
| PLA-PLGA | PLGA and nanohydroxyapatite scaffolds | PC3 | [112] |
| Curcumin-impregnated poly(lactic-co-glycolic) acid (PLGA) scaffolds | [113] | ||
| PEG | Polyethylene glycol hydrogel | PCa and LNCaP | [114] |
| Scaffolds fabricated with poly(ethylene glycol)-fibrinogen matrix supplemented with poly(ethylene glycol)-diacrylate | PC3 with BJ-5ta fibroblasts | [115] |
As described earlier for breast cancer models, PCL infiltrated with biomimetic nanohydroxyapatite using nano-clay modification with amino acids [91] was also used to develop a prostate cancer bone-mimetic model using a sequential culture of human mesenchymal stem cells, with the highly metastatic PC3 and low metastatic PCa prostate cancer cells [108][109][108,109]. This model was also used in combination with perfusion flow and horizontal flow bioreactors, indicating the role of flow-derived shear stresses in the process of metastasis [46][47][48][46,47,48].