 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Takeya Adachi | -- | 2980 | 2023-12-04 07:50:22 | | | |
| 2 | Jessie Wu | -4 word(s) | 2976 | 2023-12-04 07:59:54 | | | | |
| 3 | Jessie Wu | Meta information modification | 2976 | 2023-12-04 08:47:28 | | | | |
| 4 | Jessie Wu | Meta information modification | 2976 | 2023-12-04 08:50:05 | | |
Video Upload Options
The definition of rare disease (RD) varies across the world. There are about 296 definitions from 1109 organizations, most of which are explicitly or implicitly derived from prevalence thresholds. Such definitions are expressed as a fraction, a percentage, or the number of cases per population (whether that be from 10,000 or 100,000 people). Only a few countries consider a broader set of dimensions that are relevant from a healthcare policy perspective, capturing aspects of vulnerability and socioeconomic impact. This is, for example, the case in Thailand, where the RD definition used by the Universal Coverage Scheme is derived from a combination of a number of cases per population and a broader set of qualitative descriptors that include severity (defined by high morbidity and premature death); difficulties accessing adequate diagnosis, screening, treatment, and lifelong treatment; and high economic burdens on the family and society.
1. Introduction and Context
2. Burden of Disease
2.1. The Epidemiological and Economic Impact at the Global Level
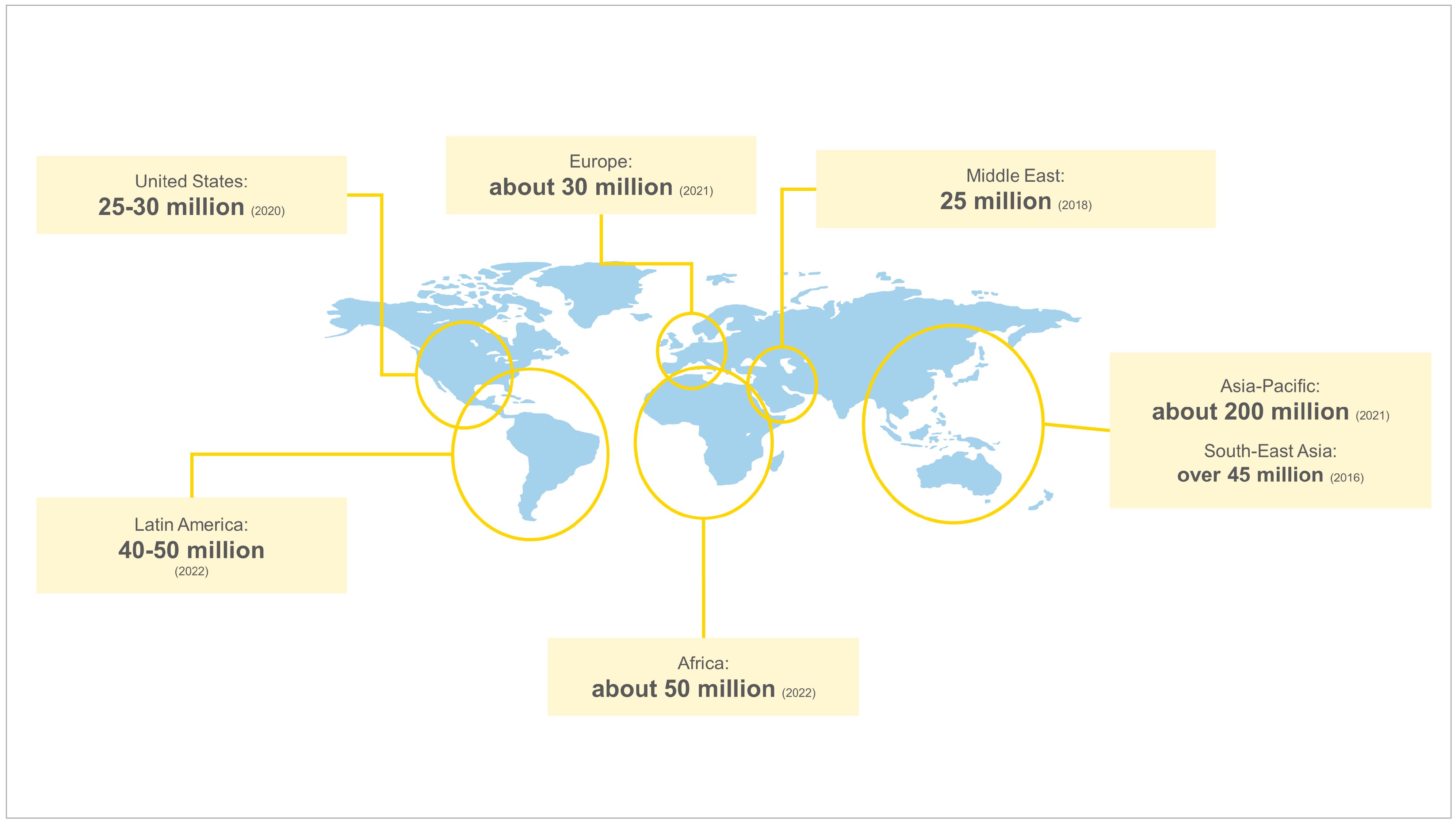
2.2. The Epidemiological and Economic Impact per Region
2.3. Gaps, Barriers, and Challenges
References
- Rare Diseases International. Agreement with the WHO . 2019. Available online: https://www.rarediseasesinternational.org/working-with-the-who/ (accessed on 4 August 2022).
- Rare Diseases International. Operational Description of Rare Diseases . 2022. Available online: https://www.rarediseasesinternational.org/wp-content/uploads/2022/08/INFOGRAPHIC-OPERATIONAL-DESCRIPTION-OF-RARE-DISEASES.pdf (accessed on 4 August 2022).
- Delaye, J.; Cacciatore, P.; Kole, A. Valuing the “Burden” and Impact of Rare Diseases: A Scoping Review. Front. Pharmacol. 2022, 13, 914338.
- Nguengang, S.W.; Lambert, D.M.; Olry, A.; Rodwell, C.; Gueydan, C.; Lanneau, V.; Murphy, D.; Le Cam, Y.; Rath, A. Estimating cumulative point prevalence of rare diseases: Analysis of the Orphanet database. Eur. J. Hum. Genet. 2020, 28, 165–173.
- World Economic Forum. Global Data Access for Solving Rare Disease—A Health Economics Value Framework. 2020. Available online: https://www3.weforum.org/docs/WEF_Global_Data_Access_for_Solving_Rare_Disease_Report_2020.pdf (accessed on 4 August 2022).
- American Association for the Advancement of Science. 7000 Challenges: The Basis and Burden of Rare Diseases . 2021. Available online: https://www.science.org/content/webinar/7000-challenges-basis-and-burden-rare-diseases (accessed on 4 August 2022).
- Rare Genomics Institute. What Are Rare Diseases? . 2021. Available online: https://www.raregenomics.org/rare-disease-facts (accessed on 4 August 2022).
- National Alliance for Caregiving. Rare Disease Caregiving in America. 2018. Available online: https://www.caregiving.org/wp-content/uploads/2020/05/NAC-RareDiseaseReport_February-2018_WEB.pdf (accessed on 4 August 2022).
- Boettcher, J.; Boettcher, M.; Wiegand-Grefe, S.; Zapf, H. Being the Pillar for Children with Rare Diseases—A Systematic Review on Parental Quality of Life. Int. J. Environ. Res. Public Health 2021, 18, 4993.
- Daly, A. Impact of Rare Disease Quality of Life: What It Means in Real Terms for PLWRD (Person Living with an RD). 2018. Available online: http://download2.eurordis.org.s3.amazonaws.com/ecrd/ECRD_2018/Speaker_Presentations/0401-Daly.pdf (accessed on 4 August 2022).
- CORD. Canada’s Rare Disease Caregivers under Immense Stress, Struggling with Mental Health Issues, Isolation and Financial Burden. . 2019. Available online: http://www.raredisorders.ca/content/uploads/CORD_NationalFamilyCaregiverDay_PressRelease_04022019_FINAL1.pdf (accessed on 30 January 2023).
- Rosselli, D.; Rueda, J.-D.; Solano, M. Ethical and economic considerations of rare diseases in ethnic minorities: The case of mucopolysaccharidosis VI in Colombia. J. Med. Ethics. 2012, 38, 699–700.
- Noonan Syndrome Awareness Association. The Challenges of Parenting A Child with a Rare Disease . 2017. Available online: https://noonansyndrome.com.au/the-challenges-of-parenting-a-child-with-a-rare-disease/ (accessed on 4 August 2022).
- Dong, D.; Wang, Y. Challenges of rare diseases in China. Lancet 2016, 387, 1906.
- Sequeira, A.R.; Mentzakis, E.; Archangelidi, O.; Paolucci, F. The economic and health impact of rare diseases: A meta-analysis. Health Policy Technol. 2021, 10, 32–44.
- Angelis, A.; Tordrup, D.; Kanavos, P. Socio-economic burden of rare diseases: A systematic review of cost of illness evidence. Health Policy 2015, 119, 964–979.
- Luzzatto, L.; I Hyry, H.; Schieppati, A.; Costa, E.; Simoens, S.; Schaefer, F.; Roos, J.C.P.; Merlini, G.; Kääriäinen, H.; Garattini, S.; et al. Outrageous prices of orphan drugs: A call for collaboration. Lancet 2018, 392, 791–794.
- Chambers, J.D.; Silver, M.C.; Berklein, F.C.; Cohen, J.T.; Neumann, P.J. Orphan drugs offer larger health gains but less favorable cost-effectiveness than non-orphan drugs. J. Gen. Intern. Med. 2020, 35, 2629–2636.
- Villa, F.; Di Filippo, A.; Pierantozzi, A.; Genazzani, A.; Addis, A.; Trifirò, G.; Cangini, A.; Tafuri, G.; Settesoldi, D.; Trotta, F. Orphan Drug Prices and Epidemiology of Rare Diseases: A Cross-Sectional Study in Italy in the Years 2014–2019. Front. Med. 2022, 9, 69.
- Andreu, P.; Karam, J.; Child, C.; Chiesi, G.; Cioffi, G. The Burden of Rare Diseases: An Economic Evaluation. 2022. Available online: https://chiesirarediseases.com/assets/pdf/chiesiglobalrarediseases.whitepaper-feb.-2022_production-proof.pdf (accessed on 30 January 2023).
- Torreya. The Future of the Global Pharmaceutical Industry 2017. Available online: https://torreya.com/publications/torreya_global_pharma_industry_study_october2017.pdf (accessed on 30 January 2023).
- Hardesty, C.; Wong, A.; Chiam, S. Giving Hope to Those Living with Rare Diseases. World Economic Forum. 2021. Available online: https://www.weforum.org/agenda/2021/02/offering-hope-to-those-with-rare-diseases/ (accessed on 4 August 2022).
- Lumaka, A.; Carstens, N.; Devriendt, K.; Krause, A.; Kulohoma, B.; Kumuthini, J.; Mubungu, G.; Mukisa, J.; Nel, M.; Olanrewaju, T.O.; et al. Increasing African genomic data generation and sharing to resolve rare and undiagnosed diseases in Africa: A call-to-action by the H3Africa rare diseases working group. Orphanet J. Rare Dis. 2022, 17, 230.
- Márquez, I.M.V. Infographic: Rare Diseases in the Americas. 2022. Available online: https://www.wilsoncenter.org/article/infographic-rare-diseases-americas (accessed on 4 August 2022).
- CML Advocates Network. Understanding CML—Chronic Myeloid Leukemia . 2022. Available online: https://www.cmladvocates.net/understanding-cml/ (accessed on 4 August 2022).
- Khosla, N.; Valdez, R. A compilation of national plans, policies and government actions for rare diseases in 23 countries. Intractable Rare Dis. Res. 2018, 7, 213–222.
- European Commission. Rare diseases. . 2021. Available online: https://research-and-innovation.ec.europa.eu/research-area/health/rare-diseases_en (accessed on 4 August 2022).
- Genetic and Rare Diseases Information Center. About GARD . 2022. Available online: https://rarediseases.info.nih.gov/about (accessed on 4 August 2022).
- The National Organization for Rare Disorders (NORD). Rare Disease Day: Frequently Asked Questions . 2019. Available online: https://rarediseases.org/wp-content/uploads/2019/01/RDD-FAQ-2019.pdf (accessed on 4 August 2022).
- Centre for Arab Genomic Studies. The Centre for Arab Studies’ Report on Rare Disease Day 2018 . 2018. Available online: https://cags.org.ae/contentfiles/publications/rarediseasecorrected2018.pdf (accessed on 4 August 2022).
- Leadley, R.M.; Lang, S.; Misso, K.; Bekkering, T.; Ross, J.; Akiyama, T.; Fietz, M.; Giugliani, R.; Hendriksz, C.J.; Hock, N.L.; et al. A systematic review of the prevalence of Morquio A syndrome: Challenges for study reporting in rare diseases. Orphanet J. Rare Dis. 2014, 9, 1–7.
- Harknett, E.; Chang, W.; Byrnes, S.; Johnson, J.; Lazor, R.; Cohen, M.; Gray, B.; Geiling, S.; Telford, H.; Tattersfield, A.; et al. Use of variability in national and regional data to estimate the prevalence of lymphangioleiomyomatosis. QJM Int. J. Med. 2011, 104, 971–979.
- Alpsoy, E.; Akman-Karakas, A.; Uzun, S. Geographic variations in epidemiology of two autoimmune bullous diseases: Pemphigus and bullous pemphigoid. Arch. Dermatol. Res. 2015, 307, 291–298.
- Auvin, S.; Irwin, J.; Abi-Aad, P.; Battersby, A. The Problem of Rarity: Estimation of Prevalence in Rare Disease. Value Health 2018, 21, 501–507.
- Angural, A.; Spolia, A.; Mahajan, A.; Verma, V.; Sharma, A.; Kumar, P.; Dhar, M.K.; Pandita, K.K.; Rai, E.; Sharma, S. Review: Understanding Rare Genetic Diseases in Low Resource Regions Like Jammu and Kashmir—India. Front. Genet. 2020, 11, 415.
- Lewin Group for the Evelyn Foundation. The National Economic Burden of Rare Disease Study. 2021. Available online: https://everylifefoundation.org/wp-content/uploads/2021/02/The_National_Economic_Burden_of_Rare_Disease_Study_Summary_Report_February_2021.pdf (accessed on 4 August 2022).
- Baldwin, Z.; Jiao, B.; Basu, A.; Roth, J.; Bender, M.A.; Elsisi, Z.; Johnson, K.M.; Cousin, E.; Ramsey, S.D.; Devine, B. Medical and Non-medical Costs of Sickle Cell Disease and Treatments from a US Perspective: A Systematic Review and Landscape Analysis. PharmacoEcon-Open 2022, 6, 469–481.
- Shrider, E.A.; Kollar, M.; Chen, F.; Semega, J. Income and Poverty in the United States: 2020. 2021. Available online: https://www.census.gov/library/publications/2021/demo/p60-273.html (accessed on 4 August 2022).
- López-Facundo, A.; Rodríguez-Castillejos, C.; Romero, Y.; Gay, J.; Prada, D. Impacto económico de los inhibidores en hemofilia tipo A pediátrica. Gac. Med. Mex. 2019, 155, 369–376.
- Ministerio de Salud Publica de Ecuador. 17 de Abril: Día Mundial de la Hemofilia. . 2017. Available online: https://www.salud.gob.ec/17-de-abril-dia-mundial-de-la-hemofilia/ (accessed on 30 January 2023).
- Ministerio de Salud. Minsa financió a más de 42 mil Personas Con Enfermedades Raras, Huérfanas y de Alto Costo . 2019. Available online: https://www.gob.pe/institucion/minsa/noticias/49122-minsa-financio-a-mas-de-42-mil-personas-con-enfermedades-raras-huerfanas-y-de-alto-costo (accessed on 4 August 2022).
- Zakzuk, J.A.; Gamero, K.; Mercado, J.F.; Guzman, N.A.; Wilchez, J.P. Costs Of Treatment of Atypical Hemolytic Uremic Syndrome in Poor Population of Colombia. Value Health 2020, 23, S330–S331.
- López-Bastida, J.; Oliva-Moreno, J.; Linertová, R.; Serrano-Aguilar, P. Social/economic costs and health-related quality of life in patients with rare diseases in Europe. Eur. J. Health Econ. 2016, 17, 1–5.
- Mestre-Ferrandiz, J.; Palaska, C.; Kelly, T.; Hutchings, A.; Parnaby, A. An analysis of orphan medicine expenditure in Europe: Is it sustainable? Orphanet J. Rare Dis. 2019, 14, 287.
- Schey, C.; Milanova, T.; Hutchings, A. Estimating the budget impact of orphan medicines in Europe: 2010–2020. Orphanet J. Rare Dis. 2011, 6, 62.
- Vogler, S.; Paris, V.; Panteli, D. Ensuring Access to Medicines: How to Redesign Pricing, Reimbursement and Procurement? World Health Organization, Regional Office for Europe. 2018. Available online: https://apps.who.int/iris/handle/10665/331972 (accessed on 30 January 2023).
- Blankart, C.R.; Stargardt, T.; Schreyögg, J. Availability of and access to orphan drugs: An international comparison of pharmaceutical treatments for pulmonary arterial hypertension, Fabry disease, hereditary angioedema and chronic myeloid leukaemia. Pharmacoeconomics 2011, 29, 63–82.
- Merlini, G.; Gribben, J.; MacIntyre, E.; Piggin, M.; Doeswijk, R. Access to Affordable Orphan Medicines in Europe: An EHA Position Paper. Hemasphere 2020, 4, e477.
- Rajasimha, H.K.; Shirol, P.B.; Ramamoorthy, P.; Hegde, M.; Barde, S.; Chandru, V.; Ravinandan, M.E.; Ramchandran, R.; Haldar, K.; Lin, J.C.; et al. Organization for rare diseases India (ORDI)—Addressing the challenges and opportunities for the Indian rare diseases’ community. Genet. Res. 2014, 96, e009.
- Taneja, A.; Shashidhara, L.S.; Bhattacharya, A. Rare Diseases in India: Time for Cure-Driven Policy Initiatives and Action. Curr. Sci. 2020, 118, 1500. Available online: https://ashoka.edu.in/static/doc_uploads/file_1591182398.pdf (accessed on 4 August 2022).
- Hsu, J.C.; Wu, H.-C.; Feng, W.-C.; Chou, C.-H.; Lai, E.C.-C.; Lu, C.Y. Disease and economic burden for rare diseases in Taiwan: A longitudinal study using Taiwan’s National Health Insurance Research Database. Tsai D-C, editor. PLoS ONE 2018, 13, e0204206.
- Conradie, E.H.; Malherbe, H.; Hendriksz, C.J.; Dercksen, M.; Vorster, B.C. An Overview of Benefits and Challenges of Rare Disease Biobanking in Africa, Focusing on South Africa. Biopreserv. Biobank. 2021, 19, 143–150.
- Rare Diseases South Africa. Our Purpose . 2021. Available online: https://www.rarediseases.co.za/our-purpose (accessed on 4 August 2022).
- Alsaqa’By, M.F.; Ibrahim, N. An Overview About Rare Diseases in Saudi Arabia and Reimbursement of Orphan Drugs. Glob. J. Med. Ther. 2019, 1, 8–13.
- Roessler, H.I.; Knoers, N.V.; van Haelst, M.M.; van Haaften, G. Drug Repurposing for Rare Diseases. Trends Pharmacol. Sci. 2021, 42, 255–267.
- Juárez-López, D.; Schcolnik-Cabrera, A. Drug Repurposing: Considerations to Surpass While Re-directing Old Compounds for New Treatments. Arch. Med. Res. 2020, 52, 243–251.
- Malik, V.; Rodino-Klapac, L.R.; Viollet, L.; Wall, C.; King, W.; Al-Dahhak, R.; Lewis, S.; Ms, C.J.S.; Kota, J.; Munuera, C.S.; et al. Gentamicin-induced readthrough of stop codons in Duchenne muscular dystrophy. Ann. Neurol. 2010, 67, 771–780.
- García-Pérez, L.; Linertová, R.; Valcárcel-Nazco, C.; Posada, M.; Gorostiza, I.; Serrano-Aguilar, P. Cost-of-illness studies in rare diseases: A scoping review. Orphanet J. Rare Dis. 2021, 16, 178.
- Pearson, I.; Rothwell, B.; Olaye, A.; Knight, C. Economic Modeling Considerations for Rare Diseases. Value Health 2018, 21, 515–524.
- Garrison, S.; Kennedy, A.; Manetto, N.; Pariser, A.R.; Rutter, J.L.; Yang, G. The Economic Burden Of Rare Diseases: Quantifying The Sizeable Collective Burden And Offering Solutions. Health Affairs. 2022. Available online: https://www.healthaffairs.org/do/10.1377/forefront.20220128.987667/ (accessed on 4 August 2022).
- Linertová, R.; García-Pérez, L.; Gorostiza, I. Cost-of-Illness in rare diseases. In Rare Diseases Epidemiology: Update and Overview; Springer: Berlin/Heidelberg, Germany, 2017; pp. 283–297.
- The Economist Intelligence Unit. Suffering in Silence: Assessing Rare Disease Awareness and Management in Asia-Pacific. 2020. Available online: https://medialib.csl.com/-/media/shared/economist-white-paper/eng_white-paper_a4_digital_final.pdf (accessed on 4 August 2022).
- Berthelot, S.; Dabic, D.; Glass, S. Rising to the Challenges of Developing Rare Disease Treatments. 2020. Available online: https://globalforum.diaglobal.org/issue/february-2020/rising-to-the-challenges-of-developing-rare-disease-treatments (accessed on 4 August 2022).
- NORD. NORD’s RareLaunch Program Announces Expanded Course Learning to Help Launch and Grow Rare Disease Nonprofits. . 2022. Available online: https://rarediseases.org/nords-rarelaunch-program-announces-expanded-course-learning-to-help-launch-and-grow-rare-disease-nonprofits/ (accessed on 30 January 2023).

