Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Aránzazu Díaz-Cuenca | -- | 2504 | 2023-10-24 14:18:38 | | | |
| 2 | Wendy Huang | Meta information modification | 2504 | 2023-10-24 14:30:36 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Song, X.; Segura-Egea, J.J.; Díaz-Cuenca, A. Bioceramic Materials Used in Regenerative Dentistry. Encyclopedia. Available online: https://encyclopedia.pub/entry/50743 (accessed on 24 July 2026).
Song X, Segura-Egea JJ, Díaz-Cuenca A. Bioceramic Materials Used in Regenerative Dentistry. Encyclopedia. Available at: https://encyclopedia.pub/entry/50743. Accessed July 24, 2026.
Song, Xiaozhe, Juan J. Segura-Egea, Aránzazu Díaz-Cuenca. "Bioceramic Materials Used in Regenerative Dentistry" Encyclopedia, https://encyclopedia.pub/entry/50743 (accessed July 24, 2026).
Song, X., Segura-Egea, J.J., & Díaz-Cuenca, A. (2023, October 24). Bioceramic Materials Used in Regenerative Dentistry. In Encyclopedia. https://encyclopedia.pub/entry/50743
Song, Xiaozhe, et al. "Bioceramic Materials Used in Regenerative Dentistry." Encyclopedia. Web. 24 October, 2023.
Copy Citation
To improve the oral and dental health of the population, regenerative dentistry is a very promising approach that aims both to prevent oral–dental deterioration and to restore the anatomy and functionality of diseased teeth. To this end, it draws on new advances in procedures based on cell biology and new biomaterials. Synthetic biomimetic materials, and particularly bioceramics are undoubtedly fundamental elements in the development of these advanced dental therapies, as the calcium phosphate type formulations are the natural bioceramic components of dental and bone tissues. To this must be added the breakthrough achieved with the new silica-based bioactive ceramic compositions, capable of stimulating biological mineralization processes.
bioactive glasses
calcium phosphates
calcium silicates
bioceramics
regenerative dentistry
1. Introduction
Oral diseases remain the most dominant conditions globally [1]. Overall, the estimated number of cases of oral diseases is about 1 billion times higher than the cases for all five of the main noncommunicable diseases (NCDs) combined: mental disorders, cardiovascular disease, diabetes mellitus, chronic respiratory diseases and cancers [2]. Untreated caries in permanent teeth are the most prevalent, which is followed by severe periodontal disease, and then untreated caries in deciduous teeth and edentulism [2]. In addition, one of the most interesting aspects currently facing dentistry is the possible connection between chronic oral inflammatory processes of infectious origin (chronic apical periodontitis and periodontal disease) and systemic health status [1][3][4]. Several epidemiological studies highlight the connection between chronic oral inflammation and systemic diseases, such as ischemic heart disease [5], hypertension [6], diabetes [7], metabolic syndrome [8], renal disease [9][10], inflammatory bowel disease [11][12], rheumatoid arthritis [13], osteoporosis [14], memory loss [15], adverse pregnancy outcomes [16], cancer [17][18], respiratory diseases [19] and COVID-19 [20].
Initially, and still in use in most of the products that are currently applied in the clinic, bioceramic materials have been synthesized from precursor salts using traditional industrial processes that required high temperatures, followed by the casting of bulk implants or the quenching of powders. However, since the early 1990s, research has begun on bioactive ceramics using an alternative process, the sol–gel technique [21][22]. The synthesis of nanomaterials can be broadly classified into two approaches: “top-down” and “bottom up”. Top-down synthesis involves the deconstruction of larger materials to produce nanostructures. Bottom-up synthesis constructs nanomaterials from basic building blocks like atoms and molecules. The sol–gel technique is an example of a bottom-up approach for producing bioceramics from small molecules. The method consists of several stages involving chemical and physical processes. The chemical process begins with the reaction of precursor monomers to form oligomers in solution (sol), which in turn polymerize into a network (gel) in the form of an integrated network of discrete particles or network polymers [23]. In general, the mechanism of hydrolysis of the precursor monomers and their condensation to oligomers are the most critical steps in sol–gel chemical synthesis. These mechanisms determine the structure and composition of the resulting material. The synthesis parameters that bias the structure toward linear or branched structures are also critical issues, which play a crucial role in determining the properties and performance of the final material.
A major advantage of the sol–gel method is that it is possible to obtain materials with high purity and homogeneity at the molecular scale and to control the surfaces, interfaces and porosity of the materials obtained at the nanometric scale [24]. The sol–gel method produces homogeneous sols that can be converted into gels with a very high volume of nanopores. This nanoporosity is undoubtedly one of the most important characteristics of advanced bioceramics, as it translates into a higher specific surface area, greater reactivity and, therefore, faster kinetics in the bioactive response [25]. The sol–gel method can be used to synthesize bioceramics with different chemical compositions, which enables the production of a wide range of materials. Besides, it is a cost-effective technique, as it requires lower reaction temperatures and simpler equipment than other high temperature burning and thermal industrial processes. The low reaction temperature reduces the energy consumption and gas emissions, which contribute to its environmental sustainability.
On the other hand, control of the processing method makes it possible to vary the morphology of the synthesized materials and, thus, obtain particles, films, monoliths or fibers [26][27]. Additionally, the whole process can be easily scaled up for large-scale production. All these characteristics make it possible to obtain bioceramics with high added value, and there is much interest in finding new synthesis routes and processes that align these advantages with other equally important commercial aspects, with respect to the economic viability of scaling up sol–gel production [24].
There are a large number of bioceramic materials on the market that are used in dentistry to stimulate the repair and regeneration of dental tissues, such as enamel, dentin and pulp, as well as bone defects in oral and maxillofacial surgeries. Most of them correspond to ceramic products obtained by conventional methods, such as melting in the case of vitreous materials or high temperature heat treatment of precursor salts. There are, however, a few commercially available products, such as NovaBone or NanoBone, that have begun to incorporate advances in sol–gel synthesis, giving them new textural properties in terms of surface and porosity. Figure 1 represents the commercial products based on bioceramics in clinical use that are most studied in the literature, marked in different colors according to the main type of bioceramic material component, namely bioactive glass (BG), calcium phosphate (CaP) or calcium silicate (CaSi), as detailed in the following sections.
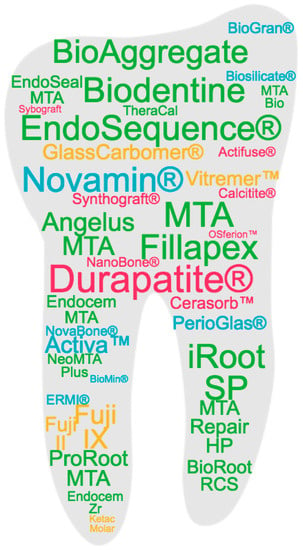
Figure 1. Commercial products based on bioceramics in clinical use that are most studied in the literature. Based on a search of the Scopus database, the products are represented with a font size according to their frequency in the title of an article and with a color code corresponding to the different types of bioceramics classified in the work: blue for bioactive glass (BG); yellow for glass ionomeric; pink for calcium phosphate (CaP); green for calcium silicate (CaSi).
2. Bioactive Glasses
Bioactive glasses (BGs) were discovered by Hench in 1969 [28]. His team at the University of Florida found that these materials elicited a biological response when they came into contact with the physiological environment, which led to a new approach for the application of biomaterials in clinical practice [29][30][31]. The original bioactive glass composition, 45S5, formulated on weight bases from 45% SiO2, 24.5% Na2O, 24.5% CaO and 6% P2O5, was commercially trademarked as Bioglass® [28] and many of the commercial products still available use this composition. Variations in this formulation, including other compounds such as K2O, MgO, CaF2 and B2O3, have been implemented and have shown altered properties such as dissolution rates and bioactivity. In addition to variations in their composition, different processing methods have also been reformed, such as their manufacture in the form of implant-like monoliths, granules or particles, pastes and cements. An excellent recent paper reviews all of the commercial BGs devices approved for therapeutic application, including hard tissue scaffolding, dental remineralization, soft tissue repair and cancer treatment [32].
In the field of dentistry, Endosseous Ridge Maintenance Implant (ERMI®), PerioGlas®, BioGran®, NovaBone® and NovaMin® are commercialized bioactive glass products based on the 45S5 composition. ERMI® is used in the form of a monolith to be implanted into the void left following tooth extraction to encourage bone formation and to provide a stable ridge for future tooth replacement [33][34][35]. PerioGlas® is used for the repair of periodontal and smaller oral defects. It was the first product to be delivered as glass powder, ranging from 90 to 710 μm, which makes surgery easier by allowing the operator to pack the wound with powder rather than fit a premade product into the void [36][37][38]. BioGran® has a similar application to PerioGlas®, but with a narrow particle size of 300 to 360 μm [39][40][41][42]. NovaBone® is available in the form of dental putty combined with a binder to improve handling for grafting, and also as interconnected porous granules for faster bone integration and remodeling for reconstructive surgeries, such as ridge maintenance and augmentation, extraction sites, implant preparation and placement [43][44][45]. NovaMin® is applied to toothpaste for treating tooth hypersensitivity. It has a fine particle size with a D50 of 18 μm, which allows the glass to have a higher probability of entering the dentin tubules in the teeth [46][47][48][49][50][51]. Besides, NovaMin® is used in polishing and teeth whitening procedures to stimulate mineralization [26] and has been shown to help to treat gingivitis [52]. BioMin® is a modification of the 45S5 composition containing either fluorine (BioMin F) or chlorine (BioMin C) to aid in apatite precipitation for dentin hypersensitivity [53][54]. Another glass composition variation (wt.%), 48.5% SiO2, 23.75% Na2O, 23.75% CaO and 4% P2O5, is used to produce the Biosilicate® glass ceramic. Biosilicate, engineered under a controlled double-stage heat treatment, is effective in the clinical reduction of sensitivity in enamel and dentine [55][56][57].
Bioactive glasses of undisclosed exact composition are also marketed as components in composite formulations with resins, polymers and other agents for use as restorative esthetic composites and biomaterials for endodontics. Activa™ BioACTIVE contains a shock-absorbing component, making it resistant to fracture and wear. It chemically bonds to the tooth and releases and recharges calcium, phosphate and fluoride ions, providing long-term benefits [58][59]. GuttaFlow® is composed of gutta-percha, polydimethylsiloxane, platinum catalyzer, zirconium dioxide and BG, showing low solubility, low porosity, alkalization capacity, dentin penetrability and cytocompatibility [60]. A newly developed bioactive glass-based cement, Nishita Canal Sealer BG (NCS-BG), is now being commercially marketed as a root canal sealer and applied within clinical endodontic treatments [61].
Finally, Ting et al. [62] reported that the 58S glass (nominal composition 60 mol% SiO2, 36 mol% CaO and 4 mol% P2O5) was one of the first sol–gel-derived bioactive glass compositions developed and commercialized by NovaBone Products LLC (Alachua, FL, USA), although hydroxyapatite (HA) was found to form within the 58S glass during sol–gel synthesis after thermal stabilization, where it was heated to 700 °C.
Although with a distinctive bioactive ability in restorative dentistry, glass-ionomer materials also deserve a separate mention. They are a group of materials composed of silicate glass powder and an aqueous solution containing polyacrylic acid that solidifies due to an acid–base reaction [63]. Glass-ionomer cements (GICs) are considered bioactive because they release biologically active ions, such as fluoride, calcium, strontium, sodium, phosphate or silicon, that result in long-term durable bonds at the tooth–restoration interface [64][65]. Commercial GICs, Fuji IX [66][67][68][69], Ketac Molar [70][71], Glass Carbomer® [72][73][74][75], have been shown to promote remineralization in the mouth. Resin-modified products, Fuji II [76][77][78] and Vitremer™ [79][80][81], also contain ion-leachable glass powder, as well as the water-soluble organic monomer 2-hydroxyethyl methacrylate (HEMA), and are widely used as alternatives to amalgam.
3. Calcium Phosphates
Synthetic calcium ortho-phosphate (CaP) materials can be prepared with a chemical composition very similar to that of the inorganic part of human bones and teeth. They are widely used in medicine for their biocompatibility, bioactivity and osteoconductivity properties [82]. Bone and dentine contain about 70% calcium phosphate (CaP) mineral in the form of a poorly crystalline, highly substitute apatite phase, consisting of very small crystallites, with a thickness of only 5 nm. Enamel, on the other hand, consists almost exclusively of hydroxyapatite prisms up to 100 µm in length and oriented in structures that confer resistance to abrasion [83]. Several dental specialties deal with the invasion into or the treatment of the surrounding bones, such as the filling and/or reconstruction of a traumatic or degenerative multi-walled bone defect, augmentation of the sinus floor, augmentation of alveolar ridges, the filling of periodontal or other alveolar bone defects, tooth sockets, osteotomies and the preservation of the alveolus for the preparation of an implant site. Depending on the application, different compounds, such as monocalcium phosphate (MCP; Ca(H2PO4)2), dicalcium phosphate (DCPA; CaHPO4), tricalcium phosphate (TCP; Ca3(PO4)2) or hydroxyapatite (HA; Ca10(PO4)6(OH)2), as well as their processing in different formats, such as particles, granulates, dense blocks, porous parts, pastes or coatings, have been developed. Research on this type of material is very extensive, as some recent reviews in the bibliography show [84][85][86]. Dorozhkin [84] highlights that the first publications on the application of CaPs in dentistry deal with their inclusion in toothpaste formulations to promote remineralization and reduce tooth sensitivity, and reviews these materials according to two types of classification, namely the CaP compound formulation and the specific application for the different specialties in dentistry [84].
The first reported commercial CaP products are based on β-TCP and HA, such as Synthograft® (β-TCP) [87][88][89][90], Durapatite® (HA) [91][92][93][94], Calcitite® (HA) [95][96] and Alveograft® (HA) [97]. Also, β-TCP based products are subsequent to Cerasorb™ [98][99][100] and OSferion™ [101]. Actifuse® is a porous silicate-substituted calcium phosphate [102][103]. Synthetic nano-crystalline HA is commercialized as a single component bone graft by Sybograft® [104], and as a composite formulation NanoBone® consisting of nanocrystalline HA embedded in a silica gel matrix, produced using a sol–gel process [105][106][107]. Besides, CaPs are incorporated as components in self-setting products, such as Endo Sequence® BD Sealer, a premixed ready-to-use injectable cement for sealing applications, which contains MCP [84][108].
4. Calcium Silicates
Calcium silicates, mainly Ca3SiO5 and Ca2SiO4, are the basic compounds in bioactive endodontic cements (BECs) [109][110]. BECs are bioceramics widely used in endodontics as restorative cements used in vital pulp therapy and endodontic sealers, due to their high biocompatibility, intrinsic osteoconductive activity and ability to induce regenerative responses as dentin bridges that promote better sealing of the pulp-capped site [59][111]. These calcium silicates compounds are capable of reacting with water at a physiological temperature, causing a hydraulic setting reaction. Originally the first product formulation was described as a powder composed of calcia, silica and alumina oxides and was then named mineral trioxide aggregate (MTA), which is still a generic name used for BECs in dentistry [112]. In fact, MTA is based on Portland cement, which was revisited by Torabinejad et al. [113] for its use in endodontics. Despite its excellent properties, some problems in its clinical application, such as the long setting time, tooth discoloration, high cost and difficult handling, have driven the development of new formulations.
The first clinically approved formulation was ProRoot MTA [114]. The initial setting time has been reported from 70 to 74 min [110]. In 2002, the gray ProRoot MTA (GMTA) was substituted by the new white ProRoot MTA (WMTA), free from tetracalcium aluminoferrite to reduce the problems concerning tooth discoloration [115]. MTA Angelus [116][117] followed with a similar composition based on Portland cement, but without the calcium sulphate dehydrate (gypsum). Further products marketed with shorter setting times are Biodentine [118][119][120][121][122][123][124][125], Endocem MTA [126][127][128][129], MTA Bio [130][131], EndoSeal MTA [132][133] and MTA Fillapex [134][135][136][137][138][139]. A setting time of as little as 0.3 min has been reported for TheraCal [140][141][142][143][144] because of the use of resin and light cure technology. The radiopacifying agent used is another important element that has been studied for the improvement of these products. ProRoot MTA contains about 2 at.% Bi [115], which may not only produce tooth discoloration but also reduce its biocompatibility [145]. As an alternative to bismuth oxide, other compounds have been used, such as tantalum oxide Ta2O5, which is used in BioAggregate [146][147][148][149][150] and NeoMTA Plus [109][151][152][153]. ZrO2 is another agent widely used in products such as Endocem Zr [127][154], EndoSequence [155][156], iRoot SP [157][158][159][160], BioRoot RCS [161][162][163][164] and the previously mentioned Biodentine. MTA Repair HP, notable for its low setting time and fast bioactive response in vitro [165], contains CaWO4 as a radiopacifying agent and consists of tricalcium silicate nanoparticles with high aspect ratio, which provide to the precursor material an elevated surface area to maximize the hydration reaction [166][167].
References
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260.
- World Health Organization. Global Oral Health Status Report: Towards Universal Health Coverage for Oral Health by 2030; World Health Organization: Geneva, Switzerland, 2022.
- Seymour, R.A. Is gum disease killing your patient? Br. Dent. J. 2009, 206, 551–552.
- Botelho, J.; Mascarenhas, P.; Viana, J.; Proença, L.; Orlandi, M.; Leira, Y.; Chambrone, L.; Mendes, J.J.; Machado, V. An umbrella review of the evidence linking oral health and systemic noncommunicable diseases. Nat. Commun. 2022, 13, 7614.
- Aminoshariae, A.; Kulild, J.C.; Fouad, A.F. The Impact of Endodontic Infections on the Pathogenesis of Cardiovascular Disease(s): A Systematic Review with Meta-analysis Using GRADE. J. Endod. 2018, 44, 1361–1366.e3.
- Segura-Egea, J.J.; Jimenez-Moreno, E.; Calvo-Monroy, C.; Ríos-Santos, J.V.; Velasco-Ortega, E.; Sánchez-Domínguez, B.; Castellanos-Cosano, L.; Llamas-Carreras, J.M. Hypertension and dental periapical condition. J. Endod. 2010, 36, 1800–1804.
- Cabanillas-Balsera, D.; Martín-González, J.; Montero-Miralles, P.; Sánchez-Domínguez, B.; Jiménez-Sánchez, M.C.; Segura-Egea, J.J. Association between diabetes and nonretention of root filled teeth: A systematic review and meta-analysis. Int. Endod. J. 2019, 52, 297–306.
- Velioğlu, E.M.; Aydındoğan, S.; Hakkı, S.S. Metabolic Syndrome and Periodontal Disease. Curr. Oral Health Rep. 2023, 10, 43–51.
- Palmeira, E.; de Liz Pérez-Losada, F.; Díaz-Flores-García, V.; Segura-Sampedro, J.J.; Segura-Egea, J.J.; López-López, J. Prevalence of oral infections in chronic kidney disease patients: A cross-sectional study. Oral Dis. 2023.
- Shimizu, Y.; Yamanashi, H.; Kitamura, M.; Miyata, J.; Nonaka, F.; Nakamichi, S.; Saito, T.; Nagata, Y.; Maeda, T. Association between periodontitis and chronic kidney disease by functional atherosclerosis status among older Japanese individuals: A cross-sectional study. J. Clin. Periodontol. 2023, 50, 430–439.
- Segura-Sampedro, J.J.; Jiménez-Giménez, C.; Jane-Salas, E.; Cabanillas-Balsera, D.; Martín-González, J.; Segura-Egea, J.J.; López-López, J. Periapical and endodontic status of patients with inflammatory bowel disease: Age- and sex-matched case–control study. Int. Endod. J. 2022, 55, 748–757.
- Madsen, G.R.; Bertl, K.; Pandis, N.; Stavropoulos, A.; Burisch, J. The Impact of Periodontitis on Inflammatory Bowel Disease Activity. Inflamm. Bowel Dis. 2023, 29, 396–404.
- Leech, M.T.; Bartold, P.M. The association between rheumatoid arthritis and periodontitis. Best Pract. Res. Clin. Rheumatol. 2015, 29, 189–201.
- Hong, S.W.; Lee, J.Y.; Kang, J.H. Associations between oral health status and risk of fractures in elder adults. Sci. Rep. 2023, 13, 1361.
- Noble, J.M.; Borrell, L.N.; Papapanou, P.N.; Elkind, M.S.V.; Scarmeas, N.; Wright, C.B. Periodontitis is associated with cognitive impairment among older adults: Analysis of NHANES-III. J. Neurol. Neurosurg. Psychiatry 2009, 80, 1206–1211.
- Xu, B.; Han, Y.W. Oral bacteria, oral health, and adverse pregnancy outcomes. Periodontology 2000 2022, 89, 181–189.
- Shi, T.; Min, M.; Sun, C.; Zhang, Y.; Liang, M.; Sun, Y. Periodontal disease and susceptibility to breast cancer: A meta-analysis of observational studies. J. Clin. Periodontol. 2018, 45, 1025–1033.
- Nwizu, N.N.; Marshall, J.R.; Moysich, K.; Genco, R.J.; Hovey, K.M.; Mai, X.; LaMonte, M.J.; Freudenheim, J.L.; Wactawski-Wende, J. Periodontal disease and incident cancer risk among postmenopausal women: Results from the women’s health initiative observational cohort. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1255–1265.
- Scannapieco, F.A.; Bush, R.B.; Paju, S. In Associations between periodontal disease and risk for nosocomial bacterial pneumonia and chronic obstructive pulmonary disease. A systematic review. Ann. Periodontol./Am. Acad. Periodontol. 2003, 8, 54–69.
- Costa, C.A.; Vilela, A.C.S.; Oliveira, S.A.; Gomes, T.D.; Andrade, A.A.C.; Leles, C.R.; Costa, N.L. Poor oral health status and adverse COVID-19 outcomes: A preliminary study in hospitalized patients. J. Periodontol. 2022, 93, 1889–1901.
- Li, R.; Clark, A.E.; Hench, L.L. An investigation of bioactive glass powders by sol-gel processing. J. Appl. Biomater. Off. J. Soc. Biomater. 1991, 2, 231–239.
- Hench, L.L.; Wheeler, D.L.; Greenspan, D.C. Molecular Control of Bioactivity in Sol-Gel Glasses. J. Sol-Gel Sci. Technol. 1998, 13, 245–250.
- Hench, L.L.; West, J.K. The Sol-Gel Process. Chem. Rev. 1990, 90, 33–72.
- Owens, G.J.; Singh, R.K.; Foroutan, F.; Alqaysi, M.; Han, C.M.; Mahapatra, C.; Kim, H.W.; Knowles, J.C. Sol-gel based materials for biomedical applications. Prog. Mater. Sci. 2016, 77, 1–79.
- Ramiro-Gutiérrez, M.L.; Will, J.; Boccaccini, A.R.; Díaz-Cuenca, A. Reticulated bioactive scaffolds with improved textural properties for bone tissue engineering: Nanostructured surfaces and porosity. J. Biomed. Mater. Res.-Part A 2014, 102, 2982–2992.
- Jones, J.R. Review of bioactive glass: From Hench to hybrids. Acta Biomater. 2013, 9, 4457–4486.
- Borrego-González, S.; Romero-Sánchez, L.B.; Blázquez, J.; Díaz-Cuenca, A. Nanostructured hybrid device mimicking bone extracellular matrix as local and sustained antibiotic delivery system. Microporous Mesoporous Mater. 2018, 256, 165–176.
- Hench, L.L. The story of Bioglass®. J. Mater. Sci. Mater. Med. 2006, 17, 967–978.
- Hench, L.L.; Splinter, R.J.; Allen, W.C.; Greenlee, T.K. Bonding mechanisms at the interface of ceramic prosthetic materials. J. Biomed. Mater. Res. 1971, 5, 117–141.
- Hench, L.L.; Paschall, H.A. Direct chemical bond of bioactive glass-ceramic materials to bone and muscle. J. Biomed. Mater. Res. 1973, 7, 25–42.
- Hench, L.L.; Paschall, H.A. Histochemical responses at a biomaterial’s interface. J. Biomed. Mater. Res. 1974, 8, 49–64.
- Shearer, A.; Montazerian, M.; Sly, J.J.; Hill, R.G.; Mauro, J.C. Trends and perspectives on the commercialization of bioactive glasses. Acta Biomater. 2023, 160, 14–31.
- Stanley, H.R.; Hall, M.B.; Colaizzi, F.; Clark, A.E. Residual alveolar ridge maintenance with a new endosseous implant material. J. Prosthet. Dent. 1987, 58, 607–613.
- Wilson, J.; Clark, A.E.; Hall, M.; Hench, L.L. Tissue response to Bioglass endosseous ridge maintenance implants. J. Oral Implantol. 1993, 19, 295–302.
- Stanley, H.R.; Hall, M.B.; Clark, A.E.; King Iii, C.J.; Hench, L.L.; Berte, J.J. Using 45S5 Bioglass Cones as Endosseous Ridge Maintenance Implants to Prevent Alveolar Ridge Resorption: A 5-Year Evaluation. Int. J. Oral Maxillofac. Implant. 1997, 12, 95–105.
- Carinci, F.; Palmieri, A.; Martinelli, M.; Perrotti, V.; Piattelli, A.; Brunelli, G.; Arlotti, M.; Pezzetti, F. Genetic portrait of osteoblast-like cells cultured on PerioGlas. J. Oral Implantol. 2007, 33, 327–333.
- Carmagnola, D.; Abati, S.; Celestino, S.; Chiapasco, M.; Bosshardt, D.; Lang, N.P. Oral implants placed in bone defects treated with Bio-Oss®, Ostim®-Paste or PerioGlas: An experimental study in the rabbit tibiae. Clin. Oral Implant. Res. 2008, 19, 1246–1253.
- Pantchev, A.; Nohlert, E.; Tegelberg, Å. Endodontic surgery with and without inserts of bioactive glass PerioGlas®—A clinical and radiographic follow-up. Oral Maxillofac. Surg. 2009, 13, 21–26.
- Cancian, D.C.J.; Hochuli-Vieira, E.; Marcantonio, R.A.C.; Marcantonio, E., Jr. Use of BioGran and Calcitite in Bone Defects: Histologic Study in Monkeys (Cebus apella). Int. J. Oral Maxillofac. Implant. 1999, 14, 859–864.
- Trisi, P.; Rebaudi, A.; Calvari, F.; Lazzara, R.J. Sinus graft with biogran, autogenous bone, and PRP: A report of three cases with histology and micro-CT. Int. J. Periodontics Restor. Dent. 2006, 26, 113–125.
- Pereira, R.D.S.; Menezes, J.D.; Bonardi, J.P.; Griza, G.L.; Okamoto, R.; Hochuli-Vieira, E. Histomorphometric and immunohistochemical assessment of RUNX2 and VEGF of Biogran™ and autogenous bone graft in human maxillary sinus bone augmentation: A prospective and randomized study. Clin. Implant Dent. Relat. Res. 2017, 19, 867–875.
- Frigério, P.B.; Gomes-Ferreira, P.H.S.; de Souza Batista, F.R.; Moura, J.; Júnior, I.R.G.; Botticelli, D.; Lisboa-Filho, P.N.; Okamoto, R. Effect of topical PTH 1-34 functionalized to biogran® in the process of alveolar repair in rats submitted to orchiectomy. Materials 2022, 15, 207.
- Wotiz, A.W. Novabone may stimulate new bone growth as well as BMP-2. Adv. Mater. Process. 2005, 163, 60–61.
- Qiu, Z.; Yang, H.; Wu, J.; Wei, L.; Li, J. Ionic dissolution products of NovaBone® promote osteoblastic proliferation via influences on the cell cycle. J. Int. Med. Res. 2009, 37, 737–745.
- Malik, R.; Gupta, A.; Bansal, P.; Sharma, R.; Sharma, S. Evaluation of Alveolar Ridge Height Gained by Vertical Ridge Augmentation Using Titanium Mesh and Novabone Putty in Posterior Mandible. J. Maxillofac. Oral Surg. 2020, 19, 32–39.
- Du, M.Q.; Bian, Z.; Jiang, H.; Greenspan, D.C.; Burwell, A.K.; Zhong, J.; Tai, B.J. Clinical evaluation of a dentifrice containing calcium sodium phosphosilicate (NovaMin) for the treatment of dentin hypersensitivity. Am. J. Dent. 2008, 21, 210–214.
- Greenspan, D.C. NovaMin® and tooth sensitivity-An overview. J. Clin. Dent. 2010, 21, 61–65.
- LaTorre, G.; Greenspan, D.C. The role of ionic release from NovaMin® (calcium sodium phosphosilicate) in tubule occlusion: An exploratory in vitro study using radio-labeled isotopes. J. Clin. Dent. 2010, 21, 72–76.
- Earl, J.S.; Leary, R.K.; Muller, K.H.; Langford, R.M.; Greenspan, D.C. Physical and chemical characterization of dentin surface following treatment with NovaMin® technology. J. Clin. Dent. 2011, 22, 62–67.
- Layer, T.M. Development of a fluoridated, daily-use toothpaste containing novamin® technology for the treatment of dentin hypersensitivity. J. Clin. Dent. 2011, 22, 59–61.
- Tiwari, A.; Jain, R.K. Comparative Evaluation of White Spot Lesion incidence between NovaMin, Probiotic, And Fluoride containing Dentifrices during Orthodontic treatment Using Laser Fluorescence—A Prospective Randomized Controlled Clinical Trial. Clin. Investig. Orthod. 2023, 82, 75–82.
- Tai, B.J.; Bian, Z.; Jiang, H.; Greenspan, D.C.; Zhong, J.; Clark, A.E.; Du, M.Q. Anti-gingivitis effect of a dentifrice containing bioactive glass (NovaMin®) particulate. J. Clin. Periodontol. 2006, 33, 86–91.
- Bakry, A.S.; Abbassy, M.A.; Alharkan, H.F.; Basuhail, S.; Al-Ghamdi, K.; Hill, R. A novel fluoride containing bioactive glass paste is capable of re-mineralizing early caries lesions. Materials 2018, 11, 1636.
- Bakry, A.S.; Al-Harbi, N.; Al-Hadeethi, Y.; Abbassy, M.A.; Katturi, N.K.; Xin, B.; Roqan, I.S.; Mohammed, H.; Hill, R. Invitro evaluation of new treatment for dentin hypersensitivity using BioMin F and BioMin C. J. Non-Cryst. Solids 2023, 602, 122072.
- Pintado-Palomino, K.; Peitl Filho, O.; Zanotto, E.D.; Tirapelli, C. A clinical, randomized, controlled study on the use of desensitizing agents during tooth bleaching. J. Dent. 2015, 43, 1099–1105.
- Pintado-Palomino, K.; Tirapelli, C. The effect of home-use and in-office bleaching treatments combined with experimental desensitizing agents on enamel and dentin. Eur. J. Dent. 2015, 9, 66–73.
- Crovace, M.C.; Souza, M.T.; Chinaglia, C.R.; Peitl, O.; Zanotto, E.D. Biosilicate®—A multipurpose, highly bioactive glass-ceramic. in vitro, in vivo and clinical trials. J. Non-Cryst. Solids 2016, 432, 90–110.
- Garoushi, S.; Vallittu, P.K.; Lassila, L. Characterization of fluoride releasing restorative dental materials. Dent. Mater. J. 2018, 37, 293–300.
- Kunert, M.; Lukomska-Szymanska, M. Bio-Inductive Materials in Direct and Indirect Pulp Capping—A Review Article. Materials 2020, 13, 1204.
- Washio, A.; Morotomi, T.; Yoshii, S.; Kitamura, C. Bioactive glass-based endodontic sealer as a promising root canal filling material without semisolid core materials. Materials 2019, 12, 3967.
- Hanada, K.; Morotomi, T.; Washio, A.; Yada, N.; Matsuo, K.; Teshima, H.; Yokota, K.; Kitamura, C. In vitro and in vivo effects of a novel bioactive glass-based cement used as a direct pulp capping agent. J. Biomed. Mater. Res.-Part B Appl. Biomater. 2019, 107, 161–168.
- Ting, H.K.; Page, S.J.; Poologasundarampillai, G.; Chen, S.; Yu, B.; Hanna, J.V.; Jones, J.R. Phosphate content affects structure and bioactivity of sol-gel silicate bioactive glasses. Int. J. Appl. Glass Sci. 2017, 8, 372–382.
- Singer, L.; Fouda, A.; Bourauel, C. Biomimetic approaches and materials in restorative and regenerative dentistry: Review article. BMC Oral Health 2023, 23, 105.
- Kim, H.J.; Bae, H.E.; Lee, J.E.; Park, I.S.; Kim, H.G.; Kwon, J.; Kim, D.S. Effects of bioactive glass incorporation into glass ionomer cement on demineralized dentin. Sci. Rep. 2021, 11, 7016.
- Makanjuola, J.; Deb, S. Chemically Activated Glass-Ionomer Cements as Bioactive Materials in Dentistry: A Review. Prosthesis 2023, 5, 327–345.
- Six, N.; Lasfargues, J.J.; Goldberg, M. In vivo study of the pulp reaction to Fuji IX, a glass ionomer cement. J. Dent. 2000, 28, 413–422.
- Marczuk-Kolada, G.; Waszkiel, D.; Luczaj-Cepowicz, E.; Kierklo, A.; Pawińska, M.; Mystkowska, J. The effect of glass ionomer cement Fuji IX on the hard tissues of teeth treated by sparing methods (ART and CMCR). Adv. Med. Sci. 2006, 51 (Suppl. 1), 138–141.
- Munhoz, T.; Karpukhina, N.; Hill, R.G.; Law, R.V.; De Almeida, L.H. Setting of commercial glass ionomer cement Fuji IX by 27Al and 19F MAS-NMR. J. Dent. 2010, 38, 325–330.
- Kukreja, R.; Singla, S.; Bhadoria, N.; Pawar, P.; Gupta, K.; Khandelwal, D.; Dewani, N. An In Vitro Study to Compare the Release of Fluoride from Glass Ionomer Cement (Fuji IX) and Zirconomer. Int. J. Clin. Pediatr. Dent. 2022, 15, 35–57.
- Hosoya, Y.; García-Godoy, F. Bonding mechanism of Ketac-Molar Aplicap and Fuji IX GP to enamel and dentin. Am. J. Dent. 1998, 11, 235–239.
- Peez, R.; Frank, S. The physical-mechanical performance of the new Ketac™ Molar Easymix compared to commercially available glass ionomer restoratives. J. Dent. 2006, 34, 582–587.
- Zainuddin, N.; Karpukhina, N.; Law, R.V.; Hill, R.G. Characterisation of a remineralising Glass Carbomer® ionomer cement by MAS-NMR Spectroscopy. Dent. Mater. 2012, 28, 1051–1058.
- Olegário, I.C.; Malagrana, A.P.V.F.P.; Kim, S.S.H.; Hesse, D.; Tedesco, T.K.; Calvo, A.F.B.; Camargo, L.B.; Raggio, D.P. Mechanical properties of high-viscosity glass ionomer cement and nanoparticle glass carbomer. J. Nanomater. 2015, 16, 37.
- Hasan, A.M.H.R.; Sidhu, S.K.; Nicholson, J.W. Fluoride release and uptake in enhanced bioactivity glass ionomer cement (“glass carbomer™”) compared with conventional and resin-modified glass ionomer cements. J. Appl. Oral Sci. 2019, 27.
- Mahmoud, R.; Ibrahim, A.; Elzoghby, A.; Shaalan, O. Clinical evaluation of Carbomer compared with high viscosity glass ionomer in restoration of root caries in geriatric patients: A randomized controlled trial. J. Int. Oral Health 2022, 14, 118–127.
- Dhummarungrong, S.; Moore, B.K.; Avery, D.R. Properties related to strength and resistance to abrasion of VariGlass VLC, Fuji II L.C. Ketac-Silver, and Z-100 composite resin. ASDC J. Dent. Child. 1994, 61, 17–20.
- Mallow, P.K.; Durward, C.S.; Klaipo, M. Restoration of permanent teeth in young rural children in Cambodia using the atraumatic restorative treatment (ART) technique and Fuji II glass ionomer cement. Int. J. Paediatr. Dent. 1998, 8, 35–40.
- Ghashami, M.; Nouri, F.; Heidari, S.; Mohammadpour, M.; Mirzadeh, M.; Asgari, N. Comparative evaluation of net setting time and radiopacity in Fuji II (GC-Japan) restorative glass ionomer and Iranian glass ionomer. Dent. Res. J. 2022, 19, 109.
- Croll, T.P.; Cavanaugh, R.R. Vitremer cement for Class I restoration of permanent teeth. Pract. Periodontics Aesthetic Dent. PPAD 1994, 6, 25–32; quiz 33.
- Pereira, A.C.; Basting, R.T.; Pinelli, C.; Meneghim, M.D.C.; Werner, C.W. Retention and caries prevention of Vitremer and Ketac-Bond used as occlusal sealants. Am. J. Dent. 1999, 12, 62–64.
- Donly, K.J.; Liu, J.A. Dentin and enamel demineralization inhibition at restoration margins of Vitremer, Z 100 and Cention N. Am. J. Dent. 2018, 31, 166–168.
- Best, S.M.; Porter, A.E.; Thian, E.S.; Huang, J. Bioceramics: Past, present and for the future. J. Eur. Ceram. Soc. 2008, 28, 1319–1327.
- Dorozhkin, S.V. Calcium phosphates and human beings. J. Chem. Educ. 2006, 83, 713–719.
- Dorozhkin, S.V. Calcium orthophosphates in dentistry. J. Mater. Sci. Mater. Med. 2013, 24, 1335–1363.
- Habraken, W.; Habibovic, P.; Epple, M.; Bohner, M. Calcium phosphates in biomedical applications: Materials for the future? Mater. Today 2016, 19, 69–87.
- Cheah, C.W.; Al-Namnam, N.M.; Lau, M.N.; Lim, G.S.; Raman, R.; Fairbairn, P.; Ngeow, W.C. Synthetic material for bone, periodontal, and dental tissue regeneration: Where are we now, and where are we heading next? Materials 2021, 14, 6123.
- Braly, T.E., Jr. The use of Synthograft in periodontal bony defects. J. Oral Implantol. 1983, 10, 611–618.
- Hoexter, D.L. The use of tricalcium (Synthograft). Part I: Its use in extensive periodontal defects. J. Oral Implantol. 1983, 10, 599–610.
- Louise, F.; Fourel, J.; Roig, R. Bioceramics in periodontal bone surgery. Clinical trial of Synthograft. J. Parodontol. 1985, 4, 277–285.
- Shen, T.C. Tricalcium phosphate (Synthograft) in a vital homogeneous tooth transplant. Gen. Dent. 1985, 33, 518–519.
- Rothstein, S.S.; Paris, D.; Sage, B. Use of durapatite for the rehabilitation of resorbed alveolar ridges. J. Am. Dent. Assoc. (1939) 1984, 109, 571–574.
- Greenstein, G.; Jaffin, R.A.; Hilsen, K.L.; Berman, C.L. Repair of anterior gingival deformity with durapatite. A case report. J. Periodontol. 1985, 56, 200–203.
- Koslen, R.H. Two-stage maxillary ridge augmentation using durapatite. J. Oral Implantol. 1987, 13, 428–441.
- Yukna, R.A.; Mayer, E.T.; Amos, S.M. 5-year evaluation of durapatite ceramic alloplastic implants in periodontal osseous defects. J. Periodontol. 1989, 60, 544–551.
- Yukna, R.A.; Cassingham, R.J.; Caudill, R.F.; Evans, G.H.; Miller, S.; Mayer, E.T.; Simon, J.F. Six month evaluation of Calcitite (hydroxyapatite ceramic) in periodontal osseous defects. Int. J. Periodontics Restor. Dent. 1986, 6, 34–45.
- Shepard, W.K.; Bohat, O.; Joseph, C.E.; LoPiccolo, P.; Bernick, S. Human clinical and histological responses to a Calcitite implant in intraosseous lesions. Int. J. Periodontics Restor. Dent. 1986, 6, 46–63.
- Kwon, H.J. Ridge augmentation with hydroxylapatite (Alveograf). CDS Rev. 1984, 77, 29–33.
- Zijderveld, S.A.; Zerbo, I.R.; Van Den Bergh, J.P.A.; Schulten, E.A.J.M.; Ten Bruggenkate, C.M. Maxillary sinus floor augmentation using a β-tricalcium phosphate (Cerasorb) alone compared to autogenous bone grafts. Int. J. Oral Maxillofac. Implant. 2005, 20, 432–440.
- Bokan, I.; Bill, J.S.; Schlagenhauf, U. Primary flap closure combined with Emdogain® alone or Emdogain® and Cerasorb® in the treatment of intra-bony defects. J. Clin. Periodontol. 2006, 33, 885–893.
- Plenk, H., Jr.; Chyplyk, L.; Lederer, J. Unique bone substitution of TCP-granulates (Cerasorb®) during degradation in human sinus floor elevations. Eur. Cells Mater. 2007, 14 (Suppl. 1), 24.
- Ogose, A.; Kondo, N.; Umezu, H.; Hotta, T.; Kawashima, H.; Tokunaga, K.; Ito, T.; Kudo, N.; Hoshino, M.; Gu, W.; et al. Histological assessment in grafts of highly purified beta-tricalcium phosphate (OSferion®) in human bones. Biomaterials 2006, 27, 1542–1549.
- Licina, P.; Coughlan, M.; Johnston, E.; Pearcy, M. Comparison of Silicate-Substituted Calcium Phosphate (Actifuse) with Recombinant Human Bone Morphogenetic Protein-2 (Infuse) in Posterolateral Instrumented Lumbar Fusion. Glob. Spine J. 2015, 5, 471–478.
- Wähnert, D.; Koettnitz, J.; Merten, M.; Kronenberg, D.; Stange, R.; Greiner, J.F.W.; Kaltschmidt, C.; Vordemvenne, T.; Kaltschmidt, B. Spongostan™ leads to increased regeneration of a rat calvarial critical size defect compared to nanobone® and actifuse. Materials 2021, 14, 1961.
- Koduru, S.; Aghanashini, S.; Nadiger, S.; Apoorva, S.; Bhat, D.; Puvvalla, B. A clinical and radiographic evaluation of the efficacy of nanohydroxyapatite (Sybograf™) versus bioactive calcium phosphosilicate putty (Novabone®) in the treatment of human periodontal infrabony defects: A randomized clinical trial. Contemp. Clin. Dent. 2019, 10, 16–23.
- Gerike, W.; Bienengräber, V.; Henkel, K.O.; Bayerlein, T.; Proff, P.; Gedrange, T.; Gerber, T. The manufacture of synthetic non-sintered and degradable bone grafting substitutes. Folia Morphol. 2006, 65, 54–55.
- Götz, W.; Gerber, T.; Michel, B.; Lossdörfer, S.; Henkel, K.O.; Heinemann, F. Immunohistochemical characterization of nanocrystalline hydroxyapatite silica gel (NanoBone®) osteogenesis: A study on biopsies from human jaws. Clin. Oral Implant. Res. 2008, 19, 1016–1026.
- Meier, J.; Wolf, E.; Bienengräber, V. Application of the synthetic nanostructured bone grafting material NanoBone in sinus floor elevation. Implantologie 2008, 16, 301–314.
- Jasrasaria, N.; Tikku, A.P.; Bharti, R. Analysis of porosity, sealer dissolution and apical extrusion of endodontic sealers: A micro computed tomography study. J. Oral Biol. Craniofacial Res. 2023, 13, 495–499.
- Jiménez-Sánchez, M.D.C.; Segura-Egea, J.J.; Díaz-Cuenca, A. Higher hydration performance and bioactive response of the new endodontic bioactive cement MTA HP repair compared with ProRoot MTA white and NeoMTA plus. J. Biomed. Mater. Res.-Part B Appl. Biomater. 2019, 107, 2109–2120.
- Parirokh, M.; Torabinejad, M.; Dummer, P.M.H. Mineral trioxide aggregate and other bioactive endodontic cements: An updated overview—Part I: Vital pulp therapy. Int. Endod. J. 2018, 51, 177–205.
- Torabinejad, M.; Parirokh, M.; Dummer, P.M.H. Mineral trioxide aggregate and other bioactive endodontic cements: An updated overview—Part II: Other clinical applications and complications. Int. Endod. J. 2018, 51, 284–317.
- Primus, C.M.; Tay, F.R.; Niu, L.N. Bioactive tri/dicalcium silicate cements for treatment of pulpal and periapical tissues. Acta Biomater. 2019, 96, 35–54.
- Lee, S.J.; Monsef, M.; Torabinejad, M. Sealing ability of a mineral trioxide aggregate for repair of lateral root perforations. J. Endod. 1993, 19, 541–544.
- Camilleri, J.; Pitt Ford, T.R. Mineral trioxide aggregate: A review of the constituents and biological properties of the material. Int. Endod. J. 2006, 39, 747–754.
- Dammaschke, T.; Gerth, H.U.V.; Züchner, H.; Schäfer, E. Chemical and physical surface and bulk material characterization of white ProRoot MTA and two Portland cements. Dent. Mater. 2005, 21, 731–738.
- Song, J.S.; Mante, F.K.; Romanow, W.J.; Kim, S. Chemical analysis of powder and set forms of Portland cement, gray ProRoot MTA, white ProRoot MTA, and gray MTA-Angelus. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 102, 809–815.
- Camilleri, J.; Sorrentino, F.; Damidot, D. Investigation of the hydration and bioactivity of radiopacified tricalcium silicate cement, Biodentine and MTA Angelus. Dent. Mater. 2013, 29, 580–593.
- Camilleri, J. Investigation of Biodentine as dentine replacement material. J. Dent. 2013, 41, 600–610.
- Nowicka, A.; Lipski, M.; Parafiniuk, M.; Sporniak-Tutak, K.; Lichota, D.; Kosierkiewicz, A.; Kaczmarek, W.; Buczkowska-Radlińska, J. Response of human dental pulp capped with biodentine and mineral trioxide aggregate. J. Endod. 2013, 39, 743–747.
- Luo, Z.; Kohli, M.R.; Yu, Q.; Kim, S.; Qu, T.; He, W.X. Biodentine induces human dental pulp stem cell differentiation through mitogen-activated protein kinase and calcium-/calmodulin-dependent protein kinase II pathways. J. Endod. 2014, 40, 937–942.
- Martens, L.; Rajasekharan, S.; Cauwels, R. Pulp management after traumatic injuries with a tricalcium silicate-based cement (Biodentine™): A report of two cases, up to 48 months follow-up. Eur. Arch. Paediatr. Dent. 2015, 16, 491–496.
- Bani, M.; Aktaş, N.; Çinar, Ç.; Odabaş, M.E. The clinical and radiographic success of primary molar pulpotomy using biodentine" and mineral trioxide aggregate: A 24-month randomized clinical trial. Pediatr. Dent. 2017, 39, 284–288.
- Patel, S.; Vincer, L. Case report: Single visit indirect pulp cap using biodentine. Dent. Update 2017, 44, 141–145.
- Caruso, S.; Dinoi, T.; Marzo, G.; Campanella, V.; Giuca, M.R.; Gatto, R.; Pasini, M. Clinical and radiographic evaluation of biodentine versus calcium hydroxide in primary teeth pulpotomies: A retrospective study. BMC Oral Health 2018, 18, 54.
- Nasrallah, H.; Noueiri, B.E. Biodentine™ Pulpotomy in Stage I Primary Molars: A 12-month Follow-up. Int. J. Clin. Pediatr. Dent. 2022, 15, 660–666.
- Kim, M.; Yang, W.; Kim, H.; Ko, H. Comparison of the biological properties of ProRoot MTA, OrthoMTA, and endocem MTA cements. J. Endod. 2014, 40, 1649–1653.
- Silva, E.J.N.L.; Carvalho, N.K.; Guberman, M.R.D.C.L.; Prado, M.; Senna, P.M.; Souza, E.M.; De-Deus, G. Push-out Bond Strength of Fast-setting Mineral Trioxide Aggregate and Pozzolan-based Cements: ENDOCEM MTA and ENDOCEM Zr. J. Endod. 2017, 43, 801–804.
- Rodríguez-Lozano, F.J.; Collado-González, M.; López-García, S.; García-Bernal, D.; Moraleda, J.M.; Lozano, A.; Forner, L.; Murcia, L.; Oñate-Sánchez, R.E. Evaluation of changes in ion release and biological properties of NeoMTA-Plus and Endocem-MTA exposed to an acidic environment. Int. Endod. J. 2019, 52, 1196–1209.
- Sharma, V.; Nawal, R.R.; Augustine, J.; Urs, A.B.; Talwar, S. Evaluation of Endosequence Root Repair Material and Endocem MTA as direct pulp capping agents: An in vivo study. Aust. Endod. J. 2022, 48, 251–257.
- De-Deus, G.; Reis, C.; Brandão, C.; Fidel, S.; Fidel, R.A.S. The Ability of Portland Cement, MTA, and MTA Bio to Prevent Through-and-Through Fluid Movement in Repaired Furcal Perforations. J. Endod. 2007, 33, 1374–1377.
- De-Deus, G.; Audi, C.; Murad, C.; Fidel, S.; Fidel, R. Similar expression of through-and-through fluid movement along orthograde apical plugs of MTA Bio™ and white Portland cement. Int. Endod. J. 2008, 41, 1047–1053.
- Adl, A.; Shojaee, N.S.; Pourhatami, N. Evaluation of the dislodgement resistance of a new pozzolan-based cement (endoseal MTA) compared to proroot MTA and biodentine in the presence and absence of blood. Scanning 2019, 2019, 3863069.
- Mak, S.T.; Leong, X.F.; Tew, I.M.; Kumolosasi, E.; Wong, L. In Vitro Evaluation of the Antibacterial Activity of EndoSeal MTA, iRoot SP, and AH Plus against Planktonic Bacteria. Materials 2022, 15, 2012.
- Vitti, R.P.; Prati, C.; Silva, E.J.N.L.; Sinhoreti, M.A.C.; Zanchi, C.H.; De Souza E Silva, M.G.; Ogliari, F.A.; Piva, E.; Gandolfi, M.G. Physical properties of MTA fillapex sealer. J. Endod. 2013, 39, 915–918.
- Yavari, H.; Ghasemi, N.; Divband, B.; Rezaei, Y.; Jabbari, G.; Payahoo, S. The effect of photodynamic therapy and polymer solution containing nano-particles of Ag /ZnO on push-out bond strength of the sealers AH-Plus and MTA Fillapex. J. Clin. Exp. Dent. 2017, 9, e1109–e1114.
- Saraiva, J.A.; Da Fonseca, T.S.; Da Silva, G.F.; Sasso-Cerri, E.; Guerreiro-Tanomaru, J.M.; Tanomaru-Filho, M.; Cerri, P.S. Reduced interleukin-6 immunoexpression and birefringent collagen formation indicate that MTA Plus and MTA Fillapex are biocompatible. Biomed. Mater. 2018, 13, 035002.
- Delfino, M.M.; Guerreiro-Tanomaru, J.M.; Tanomaru-Filho, M.; Sasso-Cerri, E.; Cerri, P.S. Immunoinflammatory response and bioactive potential of GuttaFlow bioseal and MTA Fillapex in the rat subcutaneous tissue. Sci. Rep. 2020, 10, 7173.
- Elsayed, M.A.; Hassanien, E.E.; Elgendy, A.A.E. Ageing of TotalFill BC Sealer and MTA Fillapex in Simulated Body Fluid. Eur. Endod. J. 2021, 6, 183–188.
- Kumar, A.; Kour, S.; Kaul, S.; Malik, A.; Dhani, R.; Kaul, R. Cytotoxicity evaluation of Bio-C, CeraSeal, MTA-Fillapex, and AH Plus root canal sealers by microscopic and 3-(4, 5 dimethythiazol-2yl)-2, 5-diphenyltetrazolium bromide (MTT) assay. J. Conserv. Dent. 2023, 26, 73–78.
- Camilleri, J.; Laurent, P.; About, I. Hydration of biodentine, theracal LC, and a prototype tricalcium silicate-based dentin replacement material after pulp capping in entire tooth cultures. J. Endod. 2014, 40, 1846–1854.
- Arandi, N.Z.; Rabi, T. TheraCal LC: From Biochemical and Bioactive Properties to Clinical Applications. Int. J. Dent. 2018, 2018, 3484653.
- Alazrag, M.A.; Abu-Seida, A.M.; El-Batouty, K.M.; El Ashry, S.H. Marginal adaptation, solubility and biocompatibility of TheraCal LC compared with MTA-angelus and biodentine as a furcation perforation repair material. BMC Oral Health 2020, 20, 298.
- Bala Anusha, D.; Prathima, G.; Sanguida, A.; Nandakumar, S.; Kavitha, M. Role of TheraCal LC in pediatric dentistry: A narrative review. J. Int. Oral Health 2022, 14, 111–117.
- Kayad, M.; Koura, A.; El-Nozahy, A. A comparative histological study of the effect of TheraCal LC and biodentine on direct pulp capping in rabbits: An experimental study. Clin. Oral Investig. 2023, 27, 1013–1022.
- Gandolfi, M.G.; Ciapetti, G.; Taddei, P.; Perut, F.; Tinti, A.; Cardoso, M.V.; Van Meerbeek, B.; Prati, C. Apatite formation on bioactive calcium-silicate cements for dentistry affects surface topography and human marrow stromal cells proliferation. Dent. Mater. 2010, 26, 974–992.
- Zhang, H.; Pappen, F.G.; Haapasalo, M. Dentin Enhances the Antibacterial Effect of Mineral Trioxide Aggregate and Bioaggregate. J. Endod. 2009, 35, 221–224.
- Tuna, E.B.; Dinçol, M.E.; Gençay, K.; Aktören, O. Fracture resistance of immature teeth filled with BioAggregate, mineral trioxide aggregate and calcium hydroxide. Dent. Traumatol. 2011, 27, 174–178.
- Kum, K.Y.; Kim, E.C.; Yoo, Y.J.; Zhu, Q.; Safavi, K.; Bae, K.S.; Chang, S.W. Trace metal contents of three tricalcium silicate materials: MTA Angelus, Micro Mega MTA and Bioaggregate. Int. Endod. J. 2014, 47, 704–710.
- Bayram, E.; Bayram, H.M. Fracture resistance of immature teeth filled with mineral trioxide aggregate, bioaggregate, and biodentine. Eur. J. Dent. 2016, 10, 220–224.
- Eram, A.; Zuber, M.; Keni, L.G.; Kalburgi, S.; Naik, R.; Bhandary, S.; Amin, S.; Badruddin, I.A. Finite element analysis of immature teeth filled with MTA, Biodentine and Bioaggregate. Comput. Methods Programs Biomed. 2020, 190, 105356.
- Siboni, F.; Taddei, P.; Prati, C.; Gandolfi, M.G. Properties of NeoMTA plus and MTA plus cements for endodontics. Int. Endod. J. 2017, 50, e83–e94.
- Tomás-Catalá, C.J.; Collado-González, M.; García-Bernal, D.; Oñate-Sánchez, R.E.; Forner, L.; Llena, C.; Lozano, A.; Moraleda, J.M.; Rodríguez-Lozano, F.J. Biocompatibility of New Pulp-capping Materials NeoMTA Plus, MTA Repair HP, and Biodentine on Human Dental Pulp Stem Cells. J. Endod. 2018, 44, 126–132.
- Lozano-Guillén, A.; López-García, S.; Rodríguez-Lozano, F.J.; Sanz, J.L.; Lozano, A.; Llena, C.; Forner, L. Comparative cytocompatibility of the new calcium silicate-based cement NeoPutty versus NeoMTA Plus and MTA on human dental pulp cells: An in vitro study. Clin. Oral Investig. 2022, 26, 7219–7228.
- Sharma, A.; Thomas, M.; Shetty, N.; Srikant, N. Evaluation of indirect pulp capping using pozzolan-based cement (ENDOCEM-Zr®) and mineral trioxide aggregate—A randomized controlled trial. J. Conserv. Dent. 2020, 23, 152–157.
- Rodríguez-Lozano, F.J.; López-García, S.; García-Bernal, D.; Tomás-Catalá, C.J.; Santos, J.M.; Llena, C.; Lozano, A.; Murcia, L.; Forner, L. Chemical composition and bioactivity potential of the new Endosequence BC Sealer formulation HiFlow. Int. Endod. J. 2020, 53, 1216–1228.
- Mann, A.; Zeng, Y.; Kirkpatrick, T.; van der Hoeven, R.; Silva, R.; Letra, A.; Chaves de Souza, L. Evaluation of the Physicochemical and Biological Properties of EndoSequence BC Sealer HiFlow. J. Endod. 2022, 48, 123–131.
- Ersahan, S.; Aydin, C. Dislocation resistance of iRoot SP, a calcium silicate-based sealer, from radicular dentine. J. Endod. 2010, 36, 2000–2002.
- Forghani, M.; Gharechahi, M.; Karimpour, S. In vitro evaluation of tooth discolouration induced by mineral trioxide aggregate Fillapex and iRoot SP endodontic sealers. Aust. Endod. J. 2016, 42, 99–103.
- Atav Ates, A.; Dumani, A.; Yoldas, O.; Unal, I. Post-obturation pain following the use of carrier-based system with AH Plus or iRoot SP sealers: A randomized controlled clinical trial. Clin. Oral Investig. 2019, 23, 3053–3061.
- Bhor, S.; Rao, A.S.; Shah, U.; Mathur, M.; Reda, R.; Pagnoni, F.; Testarelli, L.; Luke, A.M.; Pawar, A.M. Comparative Evaluation of the Sealing Ability of a BioCeramic Sealer (iRoot SP) with AH Plus Sealer with Root Canal Dentin Using Three Different Techniques of Sealer Application: A Combined Dye Extraction and Scanning Electron Microscope Study. J. Compos. Sci. 2023, 7, 106.
- Guneser, M.B.; Akman, M.; Kolcu, İ.B.; Eldeniz, A.U. Fracture resistance of roots obturated with a novel calcium silicate-based endodontic sealer (BioRoot RCS). J. Adhes. Sci. Technol. 2016, 30, 2420–2428.
- Jeanneau, C.; Giraud, T.; Laurent, P.; About, I. BioRoot RCS Extracts Modulate the Early Mechanisms of Periodontal Inflammation and Regeneration. J. Endod. 2019, 45, 1016–1023.
- Bianco, E.; Calvelli, C.; Citterio, C.L.; Pellegatta, A.; Venino, P.M.; Maddalone, M. Evaluation with micro-CT of the canal seal made with two different bioceramic cements: Guttaflow bioseal and bioroot RCS. J. Contemp. Dent. Pract. 2020, 21, 359–366.
- Alsubait, S.; Alhathlool, N.; Alqedairi, A.; Alfawaz, H. A micro-computed tomographic evaluation of retreatability of BioRoot RCS in comparison with AH Plus. Aust. Endod. J. 2022, 47, 222–227.
- Jiménez-Sánchez, M.C.; Segura-Egea, J.J.; Díaz-Cuenca, A. MTA HP Repair stimulates in vitro an homogeneous calcium phosphate phase coating deposition. J. Clin. Exp. Dent. 2019, 11, e322–e326.
- Jiménez-Sánchez, M.C.; Segura-Egea, J.J.; Díaz-Cuenca, A. Physicochemical parameters-hydration performance relationship of the new endodontic cement MTA Repair HP. J. Clin. Exp. Dent. 2019, 11, e739–e744.
- Jiménez-Sánchez, M.C.; Segura-Egea, J.J.; Díaz-Cuenca, A. A microstructure insight of MTA repair HP of rapid setting capacity and bioactive response. Materials 2020, 13, 1641.
More
Information
Subjects:
Materials Science, Biomaterials
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
1.1K
Revisions:
2 times
(View History)
Update Date:
24 Oct 2023
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No