Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Luis M Amezcua-Guerra | -- | 3059 | 2023-09-04 18:20:20 | | | |
| 2 | Lindsay Dong | Meta information modification | 3059 | 2023-09-05 02:57:12 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Amezcua-Castillo, E.; González-Pacheco, H.; Sáenz-San Martín, A.; Méndez-Ocampo, P.; Gutierrez-Moctezuma, I.; Massó, F.; Sierra-Lara, D.; Springall, R.; Rodríguez, E.; Arias-Mendoza, A.; et al. C-Reactive Protein as Inflammatory Marker in Cardiovascular Disease. Encyclopedia. Available online: https://encyclopedia.pub/entry/48794 (accessed on 25 July 2026).
Amezcua-Castillo E, González-Pacheco H, Sáenz-San Martín A, Méndez-Ocampo P, Gutierrez-Moctezuma I, Massó F, et al. C-Reactive Protein as Inflammatory Marker in Cardiovascular Disease. Encyclopedia. Available at: https://encyclopedia.pub/entry/48794. Accessed July 25, 2026.
Amezcua-Castillo, Emanuel, Héctor González-Pacheco, Arturo Sáenz-San Martín, Pablo Méndez-Ocampo, Iván Gutierrez-Moctezuma, Felipe Massó, Daniel Sierra-Lara, Rashidi Springall, Emma Rodríguez, Alexandra Arias-Mendoza, et al. "C-Reactive Protein as Inflammatory Marker in Cardiovascular Disease" Encyclopedia, https://encyclopedia.pub/entry/48794 (accessed July 25, 2026).
Amezcua-Castillo, E., González-Pacheco, H., Sáenz-San Martín, A., Méndez-Ocampo, P., Gutierrez-Moctezuma, I., Massó, F., Sierra-Lara, D., Springall, R., Rodríguez, E., Arias-Mendoza, A., & Amezcua-Guerra, L.M. (2023, September 04). C-Reactive Protein as Inflammatory Marker in Cardiovascular Disease. In Encyclopedia. https://encyclopedia.pub/entry/48794
Amezcua-Castillo, Emanuel, et al. "C-Reactive Protein as Inflammatory Marker in Cardiovascular Disease." Encyclopedia. Web. 04 September, 2023.
Copy Citation
C-reactive protein (CRP) is an inflammatory molecule that has demonstrated value as a predictive marker for cardiovascular risk assessment, both independently and in conjunction with other parameters. It has been incorporated into risk assessment algorithms, enhancing risk prediction and guiding therapeutic decisions. Pharmacological interventions with anti-inflammatory properties, such as statins, glucagon-like peptide-1 agonists, and interleukin-1 inhibitors, have shown promising effects in reducing both cardiovascular risks and CRP levels.
C-reactive protein
coronary artery disease
atherosclerotic cardiovascular disease
inflammation
1. Introduction
Atherosclerotic cardiovascular disease (CVD) remains the leading cause of mortality worldwide. While significant progress has been made in understanding and managing conventional risk factors such as hypertension, diabetes, dyslipidemia, and smoking, CVD continues to pose a significant global health challenge [1]. Risk scoring systems incorporating these conventional risk factors have been developed to predict acute coronary syndromes (ACS) and guide therapeutic interventions. Moreover, dietary and pharmacological interventions targeting cardiovascular risk factors have demonstrated substantial benefits in the prevention and progression of coronary artery disease (CAD) [2]. In addition, public policies addressing tobacco use have contributed to reducing the incidence of ACS and the progression of atherosclerotic CVD [3]. However, it is increasingly recognized that traditional risk algorithms may not fully capture the complexities of individual patients. In recent years, inflammation has emerged as a crucial component in the pathogenesis of CVD, with numerous studies elucidating the intricate relationship between inflammation and CAD [4].
Chronic low-grade inflammation, in particular, has been acknowledged as a contributing factor in the initiation, progression, and complications of various cardiovascular conditions, including atherosclerosis, ACS, and heart failure. Interestingly, a reciprocal causality has been unveiled wherein cardiovascular risk factors exhibit the ability to incite inflammatory responses. Indeed, hypertension, dyslipidemia, smoking, diabetes, and obesity have been attributed to the ability to trigger and sustain inflammatory responses. The secretion of proinflammatory molecules may trigger a cascade of events that culminate in the destabilization of atherosclerotic lesions. This reciprocal interplay between inflammation and the pathogenesis of CAD elucidates a compelling rationale for the comprehensive management of cardiovascular risk factors with interventions that improve cardiometabolic status and decrease hypercoagulability while exerting anti-inflammatory effects [4][5].
To effectively combat CVD, it is imperative to understand the molecular and cellular processes driving the inflammatory response. This understanding is paving the way for the development of targeted anti-inflammatory interventions and bridging the gap between basic research and clinical cardiology. The shift toward translational cardiology enables the transfer of knowledge from the laboratory bench to the patient’s bedside, with the ultimate goal of achieving precision cardiology. The realization of personalized cardiology, wherein interventions are tailored to individual patients based on their unique clinical, thrombotic, and inflammatory profiles, holds great promise. By incorporating insights from the inflammatory milieu underlying each patient, we can enhance risk prediction and refine therapeutic strategies and patient outcomes [6].
2. Inflammation as a Novel Pathogenic Paradigm in Myocardial Infarction
Acute myocardial infarction (MI) triage relies on the electrocardiographic assessment of ST-segment changes, a venerable technology in use for more than a century. In the same way, confirmation of myocardial necrosis is achieved through the measurement of molecules that result from the lysis of cardiomyocytes, such as creatine kinase (CK) and cardiac troponins. Although this strategy has shown to be useful when developing evidence-based medicine, the advent of precision medicine has brought with it the need to integrate data at the individual level, encompassing genomics, novel biomarkers, lifestyle factors, and environmental influences [7][8].
Early postmortem studies proposed that plaque rupture was the main cause of fatal MI. This led to the concept of vulnerable plaques, characterized by a large central lipid core, inflammatory cell abundance, and a thin fibrous cap. It was believed that the weakening of the collagen structure in thin-capped fibroatheroma, caused by inflammatory mechanisms, resulted in coronary atheromata instability. Consequently, efforts were made to develop methods for detecting vulnerable plaques. However, identifying high-risk plaques was proved challenging due to their low predictive value [7].
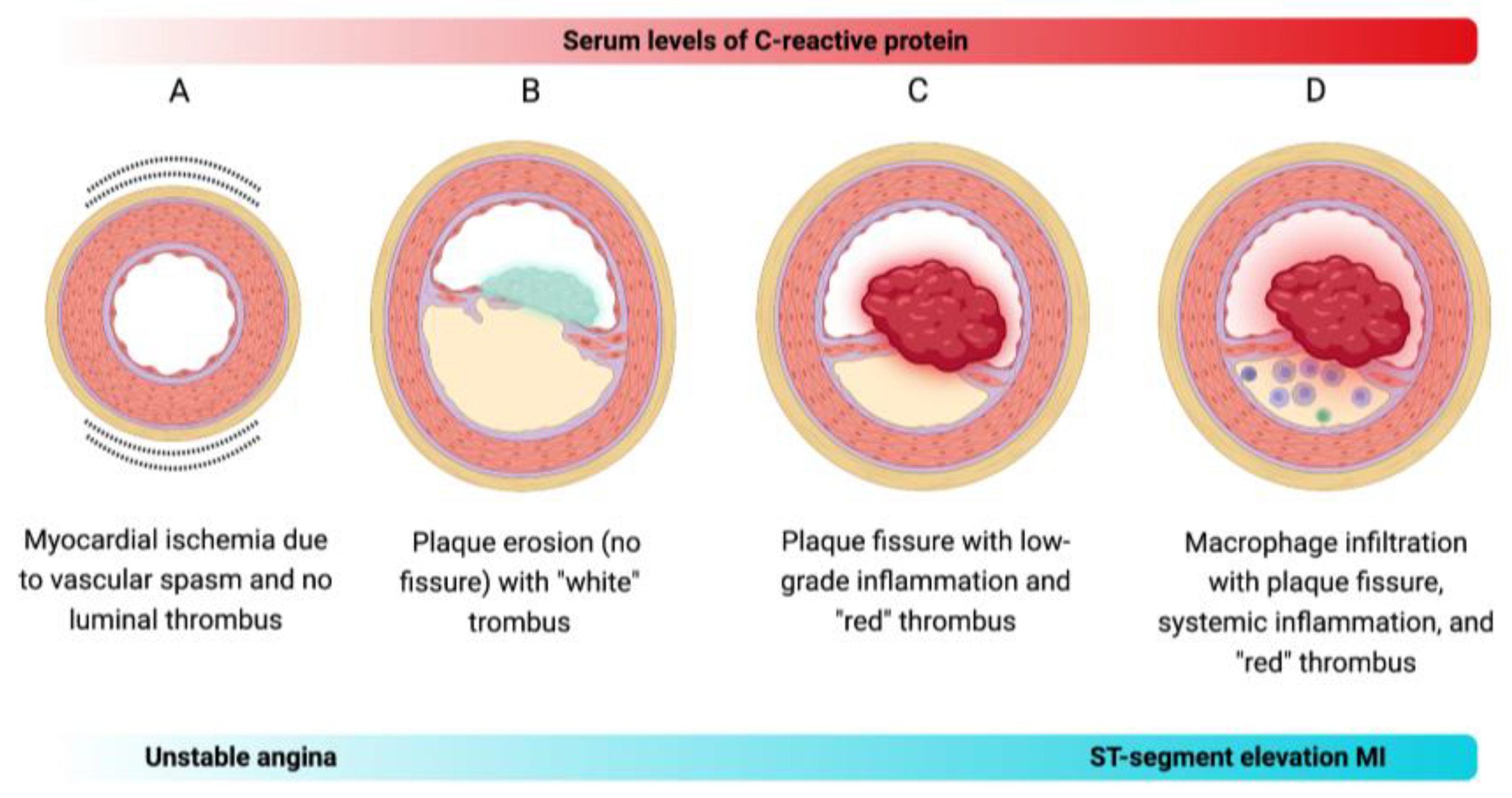
Although inflammation is a major contributor to atherosclerosis development, it may not be the sole driver of the transition from stable atherosclerosis to acute thrombosis. Evidence shows that approximately half of ACS may occur even when CRP levels are normal [9]. Moreover, up to one-third of ACS cases are caused by plaque erosion, and about one-fifth of ACS events occur without detectable coronary thrombosis, indicating that functional alterations beyond thrombus formation can contribute to the pathogenesis of CAD [10]. Based on the notion that inflammation alone may not account for all transitions to MI, Crea and Libby have contextualized a new pathogenic paradigm on the various mechanisms that may cause ACS [5]. Briefly, there are four distinct mechanisms that can lead to ACS (Figure 1):
Figure 1. Proposed mechanistic models of ACS. (A) Vasospasm-induced ACS: Vasospasm, known to occur in epicardial arteries, can also impact coronary microcirculation, triggering ACS, such as unstable angina, independently of inflammation. (B) Plaque erosion-induced ACS: Plaque erosion is increasingly recognized as a contributor to ACS, particularly the non-ST-segment elevation MI. The thrombi formed over eroded intimal patches exhibit characteristics of platelet-rich structures, termed the “white” thrombus. (C) Non-inflammatory plaque rupture-induced ACS: Some atheromata may experience plaque rupture without exhibiting extensive intimal macrophage collections or elevated circulating CRP levels. This type of plaque rupture leads to the formation of fibrin-rich “red” thrombi. (D) Inflammatory plaque rupture-induced ACS: Plaque rupture has conventionally been considered the primary cause of ACS, especially the ST-segment elevation MI. It often occurs in plaques featuring local inflammation marked by macrophage infiltration and systemic inflammation indicated by elevated CRP levels in the blood.
3. CRP Holds Potential as a Quintessential Marker of Inflammation
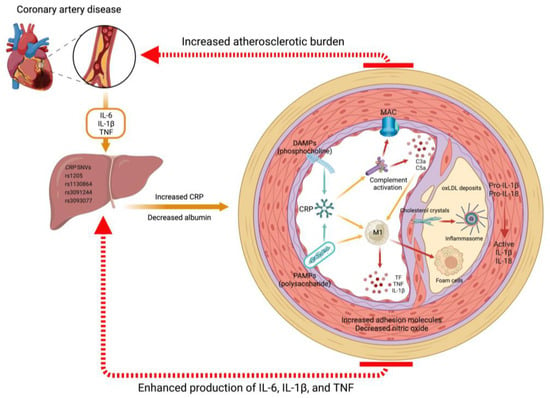
Produced primarily by hepatocytes and endothelial cells under the influence of interleukin (IL)-6, IL-1β, and tumor necrosis factor (TNF), CRP is a pentameric protein that belongs to the pentraxin superfamily. Its name originates from its ability to be bound to pneumococcal somatic C polysaccharide. CRP exhibits dual roles in inflammation, functioning as both pro-inflammatory and anti-inflammatory molecules [11][12]. CRP promotes the recognition and elimination of pathogens, as well as the clearance of necrotic and apoptotic debris. In addition to its high affinity for phosphocholine in the membrane of apoptotic debris, CRP activates the complement system through a pathway parallel to that of lectins, acting as an opsonin for phagocytosis (Figure 2) [13][14].
Figure 2. Mechanisms of CRP in atherosclerotic CVD. CRP, predominantly synthesized in the liver under the influence of proinflammatory cytokines such as IL-6, IL-1β, and TNF, plays a pivotal role in the progression of atherosclerotic CVD. Various single nucleotide variants (SNVs) can modulate CRP production. Once released into circulation, CRP exists in a pentameric form and exhibits recognition and binding capabilities to danger-associated molecular patterns (DAMPs), such as the phosphocholine found in apoptotic debris, as well as pathogen-associated molecular patterns (PAMPs), such as the lipopolysaccharide in the membrane of gram-negative bacteria. Upon activation, CRP undergoes a conformational change into functionally active monomers, leading to the initiation of the complement cascade and activation of inflammatory macrophages (M1 phenotype). In the context of chronic inflammation, these stimuli become detrimental and facilitate the deposition of oxidized low-density lipoproteins (oxLDL) and lipid-containing foam cells within the vascular sub-endothelium. The formation of cholesterol crystals in atheromatous plaques further enhances the activation of inflammasomes, which are PAMP and DAMP recognition receptors. Consequently, this process leads to increased production of IL-1β and IL-18. This inflammatory microenvironment triggers heightened production of chemoattractants and adhesion molecules while concomitantly reducing the production of nitric oxide and other vasodilatory factors. Such disruption of vascular endothelial homeostasis results in an augmented atherosclerotic burden and the development of CAD.
Elevated CRP levels are closely associated with both acute and chronic inflammatory conditions, spanning across a broad spectrum of disorders including infection, trauma, stroke, tissular necrosis, and neoplasms [15]. The conventional measurement techniques for CRP, commonly utilized to evaluate acute or severe inflammatory responses, often lack the requisite sensitivity to detect the subtle inflammatory nuances characterizing chronic conditions, including CVD. Conversely, the implementation of highly sensitive measurement methodologies enables the detection of high-sensitivity CRP, a refined iteration of the CRP assay. In essence, the principal distinction between CRP and high-sensitivity CRP resides in their inherent sensitivity and the expanse of clinical scenarios wherein they find application. In clinical practice, several techniques are used to measure CRP levels. The choice of a particular technique depends on factors such as the level of sensitivity required, the available resources, and the specific goals of the measurement. Immunonephelometry operates on the formation of antigen-antibody complexes and quantifies the intensity of scattered light when a laser passes through the sample. Enzyme-linked immunosorbent assay is a versatile technique that involves the use of antibodies that are bound to CRP, followed by a colorimetric reaction that quantifies the amount of CRP present. Color-flow cytometry employs fluorescently labeled antibodies to detect and quantify CRP levels within the analyzed cells or serum/plasma samples. Latex agglutination involves mixing CRP-specific antibodies with a latex suspension; in the presence of CRP in the sample, the latex particles agglutinate, allowing for visual detection or assessment through turbidity measurements. Point-of-care tests represent rapid diagnostic tools designed for immediate on-site CRP measurement.
4. Ethnic and Gender Differences in CRP Levels
Cardiovascular risk assessment tools are primarily based on studies consisting predominantly of Caucasian men, which may generate inaccuracies when calculating the cardiovascular risk for populations with different genetics or ethnic-racial backgrounds, or for women.
Khera and colleagues investigated the differences in CRP levels based on ethnic-racial background and gender. The study involved 2749 participants, categorized into four groups: Afro-American women, Afro-American men, Caucasian women, and Caucasian men. The findings revealed that Afro-American subjects had higher CRP levels compared to Caucasians (3.0 mg/L vs. 2.3 mg/L; p < 0.001), while women had higher levels than men (3.3 mg/L vs. 1.8 mg/L; p < 0.001). CRP levels > 3 mg/L were found in 31% of Caucasian men, 40% of Afro-American men, 51% of Caucasian women, and 58% of Afro-American women (p < 0.05 for each group vs. Caucasian men). Adjusting for conventional cardiovascular risk factors, estrogen use, statins, and body mass index, the prevalence of CRP levels > 3 mg/L remained significantly higher in Caucasian women (odds ratio [OR], 1.6; 95% confidence interval [CI], 1.1–2.5) and Afro-American women (OR, 1.7; 95% CI, 1.2–2.6), but not in Afro-American men (OR, 1.3; 95% CI, 0.8–1.9) compared to Caucasian men. This highlights the tendency of the populations different from Caucasian men (reference group) to exhibit elevated CRP levels [16].
5. Role of CRP in Predicting Cardiovascular Risk
When examining cardiovascular risk factors, the relationship between atherosclerosis and inflammation becomes evident. Sustained elevation of inflammatory markers is closely linked to the development of adverse cardiovascular events caused by the rupture of atherosclerotic plaques [17].
In 1998, Ridker and colleagues conducted a study to assess the predictive value of CRP measurement in combination with total cholesterol (TC) and high-density lipoprotein-cholesterol (HDL-C). In apparently healthy men who participated in the Physicians’ Health Study, the baseline levels of CRP, TC, and HDL-C were measured in 245 subjects who later experienced the first MI and 372 subjects who remained free of CVD during a 9-year follow-up period. Elevated levels of CRP, TC, and the TC/HDL-C ratio were significantly associated with a higher risk of future MI. Multivariate analysis showed that models incorporating CRP and lipid parameters were superior in predicting risk compared to models using only lipids. Furthermore, baseline CRP levels predicted the risk of MI even in individuals with low TC levels or high TC/HDL-C ratios [18].
Following the identification of the CRP value in predicting the first cardiovascular event in both men and women, its role in elderly populations remained to be studied. Cushman and colleagues measured baseline CRP levels in 3971 men and women aged >65 years without prior CVD. Approximately 26% of the participants had CRP concentrations >3 mg/L. After a 10-year follow-up, 547 participants developed CAD. The incidence of CAD was 33% in men and 17% in women with high CRP levels. Adjusted for age, ethnicity, and sex, the RR for CAD with CRP > 3 mg/L (compared to >1 mg/L) was 1.82 (95% CI, 1.46–2.28).
The predictive role of CRP in assessing stable ischemic cardiopathy has been investigated. Bogaty and colleagues conducted a study to measure CRP levels in 159 patients with established ischemic cardiopathy, utilizing 2 to 8 measurements taken at intervals spanning from 15 days to 6 years. The observed CRP values exhibited significant fluctuations across different ranges, namely, <1 mg/L, 1–3 mg/L, and >3 mg/L. The study revealed that 64 patients (40.3%) experienced a change in risk category between their initial and subsequent measurements. Variability in CRP levels remained consistent in different time points and clinical groups.
6. Impact of CRP Levels on Cardiovascular Risk Assessment Algorithms
The incorporation of CRP into cardiovascular risk evaluation algorithms has gained significant attention due to its role in predicting major cardiovascular events. In particular, the Reynolds risk score was first developed to estimate the risk of adverse cardiovascular events over a 10-year period in women aged 45 and older. This scoring system considers factors such as age, systolic blood pressure, diabetes mellitus, and smoking, as well as levels of TC, HDL-C, and CRP. The Reynolds risk score helps identify individuals who may benefit from statin therapy to reduce their cardiovascular risk. Women with a Reynolds risk score of 10% or lower generally do not require statin therapy.
Recognizing the independent association of CRP with future cardiovascular events and the improved predictive ability of risk calculators in women following its inclusion, Ridker and colleagues conducted a study involving 10,724 non-diabetic men, followed for an average time of 10.8 years. During this period, a total of 1294 cardiovascular events occurred. The study aimed to compare a traditional risk prediction model with one that incorporated CRP levels and family background (known as the Reynolds risk score for men).
Coronary arterial calcium quantification has emerged as a novel approach to assessing cardiovascular risk. In 2018, a study involving 7382 individuals was conducted to validate a new risk scoring system including novel cardiovascular risk factors, such as CRP measurement and coronary calcium quantification. This model, known as the Astronaut Cardiovascular Health and Risk Modification (Astro-CHARM), demonstrated improved net reclassification of individuals with risks of developing significant cardiovascular events.
7. Impact of Therapy on CRP Levels
7.1. Lipid Lowering Drugs
Several studies have demonstrated a significant reduction in serum and plasma CRP levels with the use of statins, independent of changes in lipid levels. The PRINCE study, comprising 1702 individuals in a primary prevention cohort, found that pravastatin significantly reduced the median CRP levels by 16.9% after 24 weeks compared to placebo. Multivariate analysis identified pravastatin and baseline CRP as the only predictors of the changes in CRP levels [19]. Another study evaluated the effects of three statins: simvastatin 20 mg/day, pravastatin 40 mg/day, and atorvastatin 10 mg/day on CRP levels. After 6 weeks of treatment, the CRP levels were significantly reduced with each statin. These reductions were similar between statins, and no relationship between CRP reduction and LDL-C levels was observed [20].
The effect of atorvastatin on CRP levels and its implications for CVD in patients with type 2 diabetes was assessed by Soedamah-Muthu and colleagues. The study included 2322 patients and examined the CRP response after 1 year of atorvastatin treatment compared to placebo. The results revealed a significant net reduction of 32% in CRP levels among the group receiving atorvastatin, although there was considerable variability in individual CRP responses, with 45% of patients not experiencing a reduction in CRP levels. Interestingly, initial CRP levels did not predict the occurrence of CVD during the 3.8-year follow-up period, whereas initial LDL-C levels did. Consequently, the study does not support the use of CRP as an objective marker for statin therapy in patients with diabetes [21].
A randomized controlled trial including 4497 patients diagnosed with ACS was conducted to compare the effectiveness of early intensive (40 mg/day simvastatin for one month followed by 80 mg/day) and a delayed conservative (placebo for four months and then 20 mg/day of simvastatin) therapies using statins. After one month, patients in the early intensive therapy group experienced a significant reduction in LDL-C levels. However, there was no reduction in the primary outcomes, which included cardiovascular death, new ACS, or stroke. Interestingly, a clinical benefit was observed when serum CRP levels decreased, coinciding with the increase in simvastatin dosage from 40 mg/day to 80 mg/day [22].
7.2. Glucagon-like Peptide-1 Receptor Agonists
Investigations focusing on the use of glucagon-like peptide-1 (GLP-1) receptor agonists, such as liraglutide and exenatide, have demonstrated significant improvements in cardiovascular risk factors among diabetic patients [23][24]. These GLP-1 receptor agonists exhibit a broad anti-inflammatory action, which is reflected in their ability to decrease CRP levels [25]. A controlled trial investigating the impact of liraglutide, in combination with metformin, on patients with CAD and recent diagnostic type 2 diabetes mellitus demonstrated a reduction in CRP levels. Notably, this effect was not observed with metformin monotherapy [26]. These findings were further supported by another study, which revealed that adding liraglutide was superior to lifestyle interventions in reducing CRP levels among patients with prediabetes or early diabetes who were treated with metformin [27].
7.3. Anti-Cytokine Agents
Recently, the impact of blocking inflammatory molecules using monoclonal antibodies on CVD has been explored. Canakinumab, an antibody that blocks IL-1β, was administered to 10,061 patients with ACS in the CANTOS study. The results revealed that compared to patients who received a placebo, those treated with canakinumab experienced a significant reduction in MACE such as MI, stroke, or cardiovascular death. Canakinumab had no effect on lipid levels, but it led to a decrease in CRP levels, with the extent of reduction depending on the dosage administered. In addition, patients who achieved a CRP level below 2 mg/L exhibited significant reductions in overall mortality, cardiovascular mortality, and MACE in comparison to patients who received placebo.
7.4. Other Interventions
Several interventions used in the treatment of CAD or its primary risk factors, including thiazolidinediones [28], beta blockers [29], dietary regimens [30], and physical exercise [31], have been associated with a decrease in serum or plasma CRP levels. However, these interventions have not been evaluated in clinical trials to determine whether their cardiovascular benefits depend on the reduction of CRP. Neither acetylsalicylic acid nor colchicine reduces CRP levels [32][33].
8. Conclusions
The advent of highly sensitive assays for measuring CRP has provided us with a valuable biomarker that is cost-effective, easily accessible, and universally standardized, enabling widespread utilization in clinical practice. Over the past two decades, epidemiological studies have shed light on the significant role of CRP in CVD. Its predictive value, when combined with traditional risk factors, has prompted its inclusion in cardiovascular risk calculators. Given these attributes, CRP has become the preferred laboratory biomarker for personalized or precision cardiology, offering the potential to enhance risk assessment and refine therapeutic approaches tailored to individual patients.
References
- Mora-Ramírez, M.; Estevez-Garcia, I.O.; Irigoyen-Camacho, M.E.; Bojalil, R.; Gonzalez-Pacheco, H.; Amezcua-Guerra, L.M. Hyperuricemia on Admission Predicts Short-Term Mortality due to Myocardial Infarction in a Population with High Prevalence of Cardiovascular Risk Factors. Rev. Investig. Clin. 2017, 69, 247–253.
- Rodriguez, F.; Harrington, R.A. Management of Antithrombotic Therapy after Acute Coronary Syndromes. N. Engl. J. Med. 2021, 384, 452–460.
- Wu, A.D.; Lindson, N.; Hartmann-Boyce, J.; Wahedi, A.; Hajizadeh, A.; Theodoulou, A.; Thomas, E.T.; Lee, C.; Aveyard, P. Smoking cessation for secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2022, 8, CD014936.
- Liberale, L.; Badimon, L.; Montecucco, F.; Lüscher, T.F.; Libby, P.; Camici, G.G. Inflammation, Aging, and Cardiovascular Disease: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2022, 79, 837–847.
- Crea, F.; Libby, P. Acute Coronary Syndromes: The Way Forward from Mechanisms to Precision Treatment. Circulation 2017, 136, 1155–1166.
- Shah, S.H.; Arnett, D.; Houser, S.R.; Ginsburg, G.S.; MacRae, C.; Mital, S.; Loscalzo, J.; Hall, J.L. Opportunities for the Cardiovascular Community in the Precision Medicine Initiative. Circulation 2016, 133, 226–231.
- Finn, A.V.; Nakano, M.; Narula, J.; Kolodgie, F.D.; Virmani, R. Concept of vulnerable/unstable plaque. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1282–1292.
- Stone, G.W.; Maehara, A.; Lansky, A.J.; de Bruyne, B.; Cristea, E.; Mintz, G.S.; Mehran, R.; McPherson, J.; Farhat, N.; Marso, S.P.; et al. PROSPECT Investigators. A prospective natural-history study of coronary atherosclerosis. N. Engl. J. Med. 2011, 364, 226–235.
- González-Pacheco, H.; Amezcua-Guerra, L.M.; Sandoval, J.; Martínez-Sánchez, C.; Ortiz-León, X.A.; Peña-Cabral, M.A.; Bojalil, R. Prognostic Implications of Serum Albumin Levels in Patients with Acute Coronary Syndromes. Am. J. Cardiol. 2017, 119, 951–958.
- Bentzon, J.F.; Otsuka, F.; Virmani, R.; Falk, E. Mechanisms of plaque formation and rupture. Circ. Res. 2014, 114, 1852–1866.
- Amezcua-Guerra, L.M.; Springall del Villar, R.; Bojalil Parra, R. Proteína C reactiva: Aspectos cardiovasculares de una proteína de fase aguda . Arch. Cardiol. Mex. 2007, 77, 58–66.
- Boncler, M.; Wu, Y.; Watala, C. The Multiple Faces of C-Reactive Protein-Physiological and Pathophysiological Implications in Cardiovascular Disease. Molecules 2019, 24, 2062.
- Volanakis, J.E. Human C-reactive protein: Expression, structure, and function. Mol. Immunol. 2001, 38, 189–197.
- Springall, R.; Amezcua-Guerra, L.M.; Gonzalez-Pacheco, H.; Furuzawa-Carballeda, J.; Gomez-Garcia, L.; Marquez-Velasco, R.; Mejía-Domínguez, A.M.; Cossío-Aranda, J.; Martínez-Sánchez, C.; Bojalil, R. Interferon-gamma increases the ratio of matrix metalloproteinase-9/tissue inhibitor of metalloproteinase-1 in peripheral monocytes from patients with coronary artery disease. PLoS ONE 2013, 8, e72291.
- Kushner, I.; Rzewnicki, D.; Samols, D. What does minor elevation of C-reactive protein signify? Am. J. Med. 2006, 119, e17–e28.
- Khera, A.; McGuire, D.K.; Murphy, S.A.; Stanek, H.G.; Das, S.R.; Vongpatanasin, W.; Wians, F.H., Jr.; Grundy, S.M.; de Lemos, J.A. Race and gender differences in C-reactive protein levels. J. Am. Coll. Cardiol. 2005, 46, 464–469.
- González-Pacheco, H.; Amezcua-Guerra, L.M.; Vazquez-Rangel, A.; Martínez-Sánchez, C.; Pérez-Méndez, O.; Verdejo, J.; Bojalil, R. Levels of High-Density Lipoprotein Cholesterol are Associated with Biomarkers of Inflammation in Patients with Acute Coronary Syndrome. Am. J. Cardiol. 2015, 116, 1651–1657.
- Ridker, P.M.; Glynn, R.J.; Hennekens, C.H. C-reactive protein adds to the predictive value of total and HDL cholesterol in determining risk of first myocardial infarction. Circulation 1998, 97, 2007–2011.
- Albert, M.A.; Danielson, E.; Rifai, N.; Ridker, P.M. PRINCE Investigators. Effect of statin therapy on C-reactive protein levels: The pravastatin inflammation/CRP evaluation (PRINCE): A randomized trial and cohort study. JAMA 2001, 286, 64–70.
- Jialal, I.; Stein, D.; Balis, D.; Grundy, S.M.; Adams-Huet, B.; Devaraj, S. Effect of hydroxymethyl glutaryl coenzyme a reductase inhibitor therapy on high sensitive C-reactive protein levels. Circulation 2001, 103, 1933–1935.
- Soedamah-Muthu, S.S.; Livingstone, S.J.; Charlton-Menys, V.; Betteridge, D.J.; Hitman, G.A.; Neil, H.A.; Bao, W.; DeMicco, D.A.; Preston, G.M.; Fuller, J.H.; et al. CARDS Investigators. Effect of atorvastatin on C-reactive protein and benefits for cardiovascular disease in patients with type 2 diabetes: Analyses from the Collaborative Atorvastatin Diabetes Trial. Diabetologia 2015, 58, 1494–1502.
- de Lemos, J.A.; Blazing, M.A.; Wiviott, S.D.; Lewis, E.F.; Fox, K.A.; White, H.D.; Rouleau, J.L.; Pedersen, T.R.; Gardner, L.H.; Mukherjee, R.; et al. Investigators. Early intensive vs a delayed conservative simvastatin strategy in patients with acute coronary syndromes: Phase Z of the A to Z trial. JAMA 2004, 292, 1307–1316.
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. LEADER Steering Committee; LEADER Trial Investigators. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 311–322.
- Bunck, M.C.; Diamant, M.; Eliasson, B.; Cornér, A.; Shaginian, R.M.; Heine, R.J.; Taskinen, M.R.; Yki-Järvinen, H.; Smith, U. Exenatide affects circulating cardiovascular risk biomarkers independently of changes in body composition. Diabetes Care 2010, 33, 1734–1737.
- Varanasi, A.; Patel, P.; Makdissi, A.; Dhindsa, S.; Chaudhuri, A.; Dandona, P. Clinical use of liraglutide in type 2 diabetes and its effects on cardiovascular risk factors. Endocr. Pract. 2012, 18, 140–145.
- Anholm, C.; Kumarathurai, P.; Pedersen, L.R.; Samkani, A.; Walzem, R.L.; Nielsen, O.W.; Kristiansen, O.P.; Fenger, M.; Madsbad, S.; Sajadieh, A.; et al. Liraglutide in combination with metformin may improve the atherogenic lipid profile and decrease C-reactive protein level in statin treated obese patients with coronary artery disease and newly diagnosed type 2 diabetes: A randomized trial. Atherosclerosis 2019, 288, 60–66.
- Santilli, F.; Simeone, P.G.; Guagnano, M.T.; Leo, M.; Maccarone, M.T.; Di Castelnuovo, A.; Sborgia, C.; Bonadonna, R.C.; Angelucci, E.; Federico, V.; et al. Effects of Liraglutide on Weight Loss, Fat Distribution, and β-Cell Function in Obese Subjects with Prediabetes or Early Type 2 Diabetes. Diabetes Care 2017, 40, 1556–1564.
- Pfützner, A.; Marx, N.; Lübben, G.; Langenfeld, M.; Walcher, D.; Konrad, T.; Forst, T. Improvement of cardiovascular risk markers by pioglitazone is independent from glycemic control: Results from the pioneer study. J. Am. Coll. Cardiol. 2005, 45, 1925–1931.
- Jenkins, N.P.; Keevil, B.G.; Hutchinson, I.V.; Brooks, N.H. Beta-blockers are associated with lower C-reactive protein concentrations in patients with coronary artery disease. Am. J. Med. 2002, 112, 269–274.
- King, D.E.; Egan, B.M.; Woolson, R.F.; Mainous, A.G., 3rd; Al-Solaiman, Y.; Jesri, A. Effect of a high-fiber diet vs a fiber-supplemented diet on C-reactive protein level. Arch. Intern. Med. 2007, 167, 502–506.
- Balducci, S.; Zanuso, S.; Nicolucci, A.; Fernando, F.; Cavallo, S.; Cardelli, P.; Fallucca, S.; Alessi, E.; Letizia, C.; Jimenez, A.; et al. Anti-inflammatory effect of exercise training in subjects with type 2 diabetes and the metabolic syndrome is dependent on exercise modalities and independent of weight loss. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 608–617.
- Feldman, M.; Jialal, I.; Devaraj, S.; Cryer, B. Effects of low-dose aspirin on serum C-reactive protein and thromboxane B2 concentrations: A placebo-controlled study using a highly sensitive C-reactive protein assay. J. Am. Coll. Cardiol. 2001, 37, 2036–2041.
- Tardif, J.C.; Kouz, S.; Waters, D.D.; Bertrand, O.F.; Diaz, R.; Maggioni, A.P.; Pinto, F.J.; Ibrahim, R.; Gamra, H.; Kiwan, G.S.; et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N. Engl. J. Med. 2019, 381, 2497–2505.
More
Information
Subjects:
Cardiac & Cardiovascular Systems
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
577
Revisions:
2 times
(View History)
Update Date:
05 Sep 2023
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No