Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Tadashi Nishimura | -- | 1624 | 2023-07-24 11:59:06 | | | |
| 2 | Conner Chen | Meta information modification | 1624 | 2023-07-27 05:02:02 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Nishimura, T.; Hosoi, H.; Shimokura, R.; Kitahara, T. Cartilage Conduction Hearing Aids. Encyclopedia. Available online: https://encyclopedia.pub/entry/47180 (accessed on 26 July 2026).
Nishimura T, Hosoi H, Shimokura R, Kitahara T. Cartilage Conduction Hearing Aids. Encyclopedia. Available at: https://encyclopedia.pub/entry/47180. Accessed July 26, 2026.
Nishimura, Tadashi, Hiroshi Hosoi, Ryota Shimokura, Tadashi Kitahara. "Cartilage Conduction Hearing Aids" Encyclopedia, https://encyclopedia.pub/entry/47180 (accessed July 26, 2026).
Nishimura, T., Hosoi, H., Shimokura, R., & Kitahara, T. (2023, July 24). Cartilage Conduction Hearing Aids. In Encyclopedia. https://encyclopedia.pub/entry/47180
Nishimura, Tadashi, et al. "Cartilage Conduction Hearing Aids." Encyclopedia. Web. 24 July, 2023.
Copy Citation
A relatively loud sound is audible when a vibrator is attached to the aural cartilage. This form of conduction is referred to as cartilage conduction (CC). In Japan, a new type of hearing aid has been developed using CC and has been available in clinical practice since 2017. A clinical study conducted prior to its launch demonstrated its benefits, particularly in patients with aural atresia who were unable to use air conduction hearing aids.
bone conduction
cartilage conduction
hearing device
aural atresia
1. Introduction
Sound is generally delivered to the ear via air conduction (AC) in conventional hearing aids. AC hearing aids amplify signals to help patients with various hearing losses. Unfortunately, some patients are unable to receive adequate benefits from AC hearing aids. For instance, in patients with aural atresia, hearing aids cannot be worn owing to anatomical issues or they receive inadequate benefits even if they can be worn [1]. In addition, continuous otorrhea prevents the use of hearing aids because they can prolong the inflammation, damage hearing aids, and obstruct the bore, thereby deteriorating the signal [2]. Bone conduction (BC) hearing aids have been considered as an alternative. In conventional BC hearing aids, a vibrator with static force is placed on the mastoid using a headband. BC hearing aids are effective in amplifying sound in the above-mentioned cases because sound is transmitted via BC [3][4][5]. In contrast, the fixed form of BC causes various problems, such as skin induration, long-continued depressions in the skin, and discomfort [3][4]. Furthermore, fixation with a headband is considered an esthetic disadvantage. Therefore, BC hearing aids are not preferred in patients who can use AC hearing aids without serious complications, and are rarely used in patients with unilateral aural atresia.
When a vibrator is attached to the aural cartilage, hearing is significantly improved compared with that in the unattached condition. This phenomenon was confirmed by using a probe microphone [6]. Previous studies have demonstrated this improvement to be significant, particularly at low to middle frequencies [6][7][8][9]. This unique form of transmission is called cartilage conduction (CC) [10]. Figure 1A shows the predominant pathways theoretically assumed in CC [11][12]. The first pathway is direct AC. The vibrator radiates sound around it, which cannot be completely eliminated. This airborne sound travels through the ear canal to drive the eardrum and the ossicles. This pathway is considered an AC pathway. The second pathway is the cartilage–BC. Vibrations are delivered to the skull bone via the aural cartilage, and the vibrations of the skull bone are transmitted to the cochlea in the same manner as in BC. Mediation by the aural cartilage could deteriorate these signals. This pathway is considered the BC pathway. The third pathway is the cartilage–AC. The delivered vibrations of the cartilaginous portion of the ear canal generate airborne sounds in the ear canal. The cartilaginous portion of the ear canal functions as a movable plate during this process [13]. This third pathway is not the predominant signaling route in either AC or BC. However, the airborne sound level in the cartilage AC is considered to be larger than that in direct AC in CC. The differences in the elevations of the thresholds with the insertion of an earplug and the injection of water into the ear canal demonstrated a significant cartilage AC function [11][12][14][15]. Previous studies have concluded that CC varies in the transduction method from AC and BC.
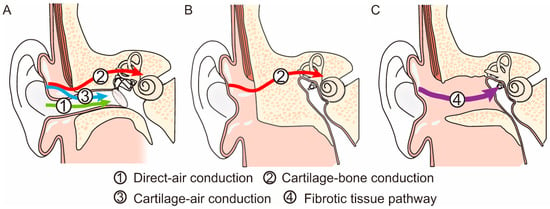
Figure 1. Difference in signal transmission in the normal ear (A), a bony atretic ear (B), and a fibrotic atretic ear with a fibrotic tissue pathway (FTP) (C).
2. Development of CC Hearing Aids
CC hearing aids are new hearing devices utilizing CC [16][17][18]. CC hearing aids were first developed in 2010 [16]. The characteristics of CC hearing aids are more similar to those of AC hearing aids than BC hearing aids because sound is finally transmitted to the cochlea via the eardrum and ossicles. In contrast to AC hearing aids, CC hearing aids deliver sounds to the aural cartilage as vibrations. In patients with aural atresia, skull vibrations are required to transmit sounds to the cochlea using any hearing device. Sound deterioration in CC is considerably lower than that in AC because it avoids the boundary between the air and the body during sound transmission. The vibrator of a CC hearing aid is placed on the aural cartilage without contact force, which is different from that of BC hearing aids. To fix it, the vibrator is inserted into the cavity or attached with double-sided tape. This fixation style can resolve the problems experienced in BC hearing aid use. In patients with continuous otorrhea, ear canal opening contributes to the continuous use of hearing devices. The vibrator of the CC hearing aid can be placed to keep the ear canal open, thereby contributing to ventilation; moreover, it is completely waterproof, which reduces the risk of damage to the vibrator. The audiological benefits of the prototype CC hearing aids were evaluated in a previous study to demonstrate their benefits, particularly in patients with aural atresia [19].
The initial prototype CC hearing aid was a box type, and the transducer was not compact [16][17]. Furthermore, a piezoelectric transducer was employed, which required a high-voltage battery for proper function. Therefore, using this prototype in clinical practice is challenging. A new electromagnetic transducer was developed as a CC hearing aid for clinical practice. It functions using the same battery used in commercially available AC hearing aids. This new transducer contributed to the miniaturization and production of a behind the ear (BTE)-style hearing aid. A clinical study was performed using the devised BTE CC hearing aids, mainly in patients with aural atresia [19]. Forty-one patients (21, 15, and 5 with bilateral aural atresia, unilateral aural atresia, and other conductive hearing loss, respectively) participated in the study. Most patients with bilateral aural atresia had used BC hearing aids before the trial. No significant differences were observed in the aided thresholds and speech recognition between the CC and BC hearing aids. After the trial, 20 patients with bilateral aural atresia continued to use the CC hearing aids. Nearly none of the patients with unilateral aural atresia used any hearing device. The functional gains obtained using the CC hearing aid were similar to those observed in patients with bilateral aural atresia. After the trial, 14 patients continued to use the CC hearing aids. A clinical study has demonstrated the effectiveness of CC hearing aids [19]; moreover, CC hearing aids were approved as new medical devices by the Ministry of Health, Labor, and Welfare in Japan and have been used in clinical practice in Japan since 2017.
3. Performance of CC Hearing Aids
Commercially available CC hearing aids are small BTE hearing aids, which were developed based on those used in clinical studies. The main body was designed based on that used in commercially available receiver-in-canal (RIC)-style AC hearing aids. The vibrator is connected to the main body with a wire that encapsulates the electrode within. Three types of vibrator units (ear-chip embedded, ear-chip attachment, and simple) are employed (Figure 2). The size and mass of the assembled transducer are 11.9 × 7.8 × 4.7 mm and 1.4 g, respectively. This type was chosen based on the ear condition. The ear chips are custom fitted, made based on ear impressions. Instead of taking an impression of the ear, computed tomography (CT) images can also be utilized for designing the vibrator [20]. Compared to the conventional process, the merits of the design using CT images are as follows: no risks related to taking the ear impression, advantage of understanding the shape of the ear in 3D, no physical transport or shipment of an ear impression, and CT images can be sent instantly via the internet. Therefore, CC hearing aids can be created without visiting the hospital. If a CT scan is performed for diagnosis or other purposes, the images can be used without additional risk. A previous study reported that the performance of a CT-based vibrator is not significantly inferior to that of an impression-based vibrator [20]. In contrast, the simple type is available for all ear conditions and can be prepared in advance; patients can try it quickly and unnecessary ear chip costs are also reduced. However, the simple type requires double-sided tape for fixation. Among the three types, the custom-fitted type is recommended for improved stability when the cavity of the fixation placement is sufficient to hold the transducer. A previous study [21] that investigated the differences in the purchase rates demonstrated a decreased purchase rate particularly in canal-open ears when a simple vibrator was used for the trial of the CC hearing aid.
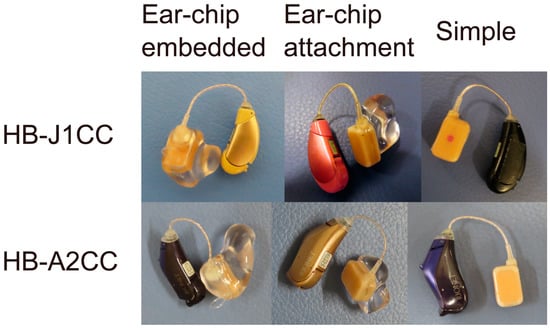
Figure 2. Two models of cartilage conduction hearing aids used in clinical practice: HB-J1CC (upper) and HB-A2CC (lower). Both models have three transducer types: ear-chip embedded (left), ear-chip attachment (middle), and simple vibrator (right).
Two CC hearing aid (HB-J1CC and HB-A2CC; Rion Co Ltd., Kokubunji, Japan) models are commercially available (Figure 2). The transducers used in the vibrator are identical. The functions of the two devices vary slightly. HB-A2CC is a later model that has been modified to reflect the feedback obtained from HB-J1CC users. Both devices were adjusted using fitting software. The gains, compression rates, and maximum output levels can be controlled. Linear amplification is utilized in patients with conduction hearing loss, such as those with aural atresia. The fitting software depicts the frequency responses on the screen; however, these simulated gains are not always equal to the actual values. Therefore, the real gains must be confirmed by measuring the unaided and aided thresholds. Both devices can manage feedback problems and directional modes. While only one program can be memorized for HB-J1CC, three programs can be used to switch memories for HB-A2CC. Furthermore, HB-A2CC can be connected via Bluetooth with an Android smartphone using an application and equipped with a child safety lock for the battery locker.
References
- Mylanus, E.A.; van der Pouw, K.C.; Snik, A.F.; Cremers, C.W. Intraindividual comparison of the bone-anchored hearing aid and air-conduction hearing aids. Arch. Otolaryngol. Head Neck Surg. 1998, 124, 271–276.
- Snik, A.F.; Mylanus, E.A.; Cremers, C.W. The bone-anchored hearing aid: A solution for previously unresolved otologic problems. Otolaryngol. Clin. N. Am. 2001, 34, 365–372.
- Dillon, H. CROS, bone-conduction, and implanted hearing aids. In Hearing Aids; Dillon, H., Ed.; Thieme: Stuttgart, Germany, 2001; pp. 434–450.
- Lo, J.F.W.; Tsang, W.S.S.; Yu, J.Y.K.; Ho, O.Y.M.; Ku, P.K.M.; Tong, M.C.F. Contemporary hearing rehabilitation options in patients with aural atresia. Biomed. Res. Int. 2014, 2014, 761579.
- Ellsperman, S.E.; Nairn, E.M.; Stucken, E.Z. Review of bone conduction hearing devices. Audiol. Res. 2021, 11, 207–219.
- Shimokura, R.; Hosoi, H.; Nishimura, T.; Yamanaka, T.; Levitt, H. Cartilage conduction hearing. J. Acoust. Soc. Am. 2014, 135, 1959–1966.
- Miyamae, R.; Nishimura, T.; Hosoi, H.; Saito, O.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Perception of speech in cartilage conduction. Auris Nasus Larynx 2017, 44, 26–32.
- Nishimura, T.; Miyamae, R.; Hosoi, H.; Saito, O.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Frequency characteristics and speech recognition in cartilage conduction. Auris Nasus Larynx 2019, 46, 709–715.
- Blondé-Weinmann, C.; Joubaud, T.; Zimpfer, V.; Hamery, P.; Roth, S. Characterization of cartilage implication in protected hearing perception during direct vibro-acoustic stimulation at various locations. Appl. Acoust. 2021, 179, 108074.
- Hosoi, H.; Nishimura, T.; Shimokura, R.; Kitahara, T. Cartilage conduction as the third pathway for sound transmission. Auris Nasus Larynx 2019, 46, 151–159.
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Matsui, T.; Yamanaka, T.; Levitt, H. Is cartilage conduction classified into air or bone conduction? Laryngoscope 2014, 124, 1214–1219.
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Yamanaka, T.; Kitahara, T.; Levitt, H. Cartilage conduction is characterized by vibrations of the cartilaginous portion of the ear canal. PLoS ONE 2015, 10, e0120135.
- Nishimura, T.; Hosoi, H.; Shimokura, R.; Morimoto, C.; Kitahara, T. Cartilage Conduction Hearing and Its Clinical Application. Audiol. Res. 2021, 11, 254–262.
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Matsui, T.; Yamanaka, T.; Kitahara, T.; Levitt, H. Cartilage conduction efficiently generates airborne sound in the ear canal. Auris Nasus Larynx 2015, 42, 15–19.
- Nishimura, T.; Hosoi, H.; Saito, O.; Akasaka, S.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Effect of fixation place on airborne sound in cartilage conduction. J. Acoust. Soc. Am. 2020, 148, 469.
- Hosoi, H.; Yanai, S.; Nishimura, T.; Sakaguchi, T.; Iwakura, T.; Yoshino, K. Development of cartilage conduction hearing aid. Arch. Mater. Sci. Eng. 2010, 42, 104–110.
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Matsui, T.; Iwakura, T. Benefit of a new hearing device utilizing cartilage conduction. Auris Nasus Larynx 2013, 40, 440–446.
- Shimokura, R.; Hosoi, H.; Iwakura, T.; Nishimura, T.; Matsui, T. Development of monaural and binaural behind-the-ear cartilage conduction hearing aids. Appl. Acoust. 2013, 74, 1234–1240.
- Nishimura, T.; Hosoi, H.; Saito, O.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Cartilage Conduction Hearing Aids for Severe Conduction Hearing Loss. Otol. Neurotol. 2018, 39, 65–72.
- Nishimura, T.; Hosoi, H.; Morimoto, C.; Okayasu, T.; Shimokura, R.; Kitahara, T. Comparison of Cartilage Conduction Hearing Devices Designed by Ear Impression and Computed Tomography. Appl. Sci. 2023, 13, 6152.
- Nishimura, T.; Hosoi, H.; Sugiuchi, T.; Matsumoto, N.; Nishiyama, T.; Kenichi, T.; Sugimoto, S.; Yazama, H.; Sato, T.; Komori, M. Factors Influencing the Purchase Rate of Cartilage Conduction Hearing Aids. J. Am. Acad. Audiol. 2022, 33, 14–22.
More
Information
Subjects:
Audiology & Speech-language Pathology
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
963
Revisions:
2 times
(View History)
Update Date:
27 Jul 2023
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No