Ibrexafungerp, an orally bioavailable glucan synthase inhibitor, is the first in a new class of triterpenoid antifungals and shares a similar target to the well-established echinocandins. Ibrexafungerp has a very favorable pharmacokinetic profile for the treatment of fungal infections with excellent tissue penetration in organs targeted by molds, such as the lungs, liver, and skin. Ibrexafungerp has demonstrated in vitro activity against Aspergillus spp. as well as efficacy alone and in combination with other antifungals in in animal models of invasive aspergillosis and mucormycosis. Furthermore, ibrexafungerp is approved for use in the USA for the treatment of women with vulvovaginal candidiasis and for the reduction in the incidence of recurrent vulvovaginal candidiasis.
1. Ibrexafungerp Mechanism of Action
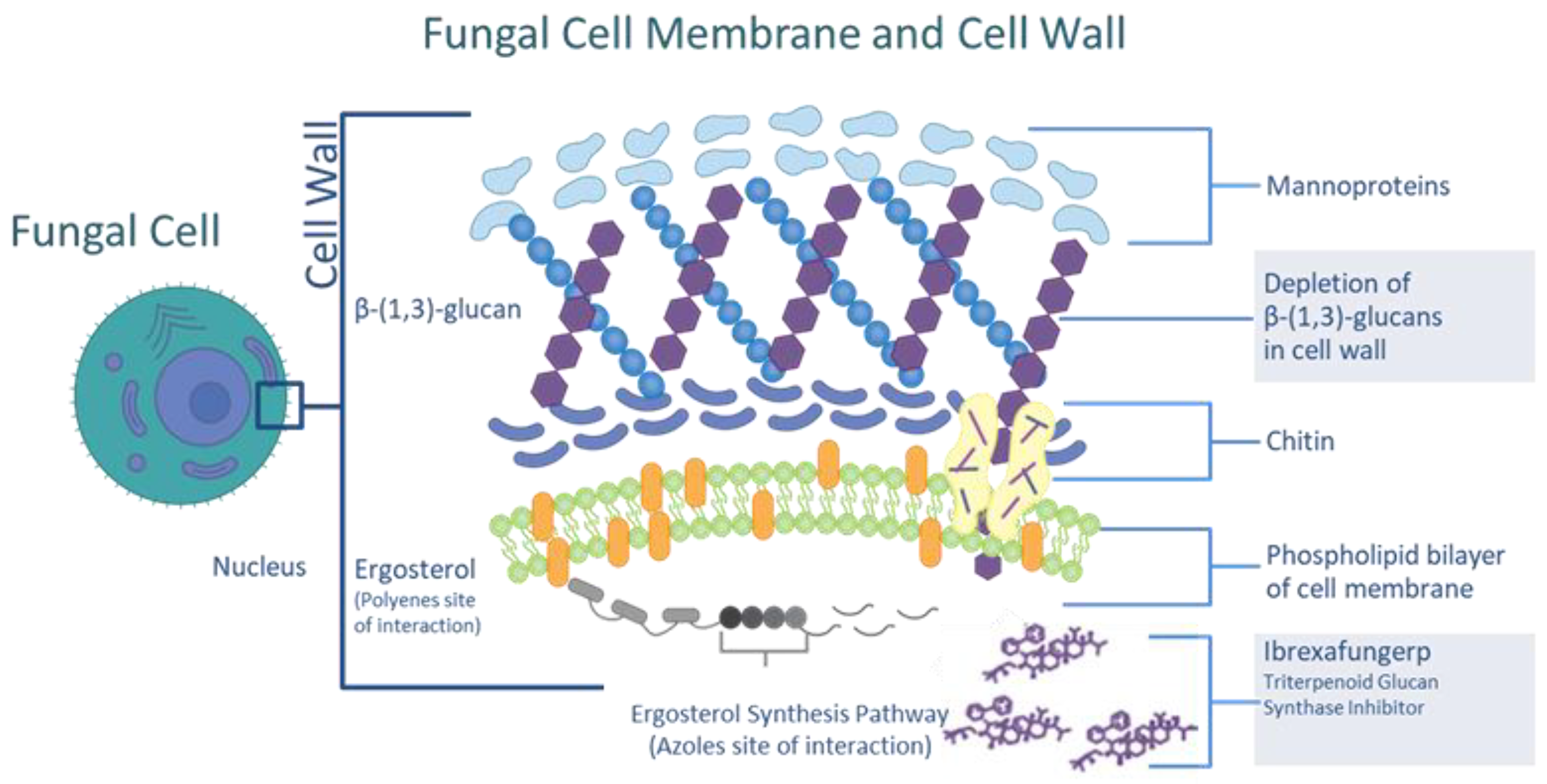
Ibrexafungerp (previously MK-3118 and SCY-078; SCYNEXIS, Inc.; Jersey City, NJ, USA) disrupts fungal cell wall synthesis through the inhibition of (1,3)-β-D-glucan synthase
[1]. Glucan synthase inhibition is also the mechanism of action of the echinocandins and has been demonstrated to result in a clinically meaningful effect in the treatment of yeast and mold infections. Because ibrexafungerp targets an enzymatic pathway that is not found in human cells, it has a low risk of off-target effects (
Figure 1).
Figure 1. The site and mechanism of action of ibrexafungerp.
Ibrexafungerp, a triterpenoid antifungal, is structurally distinct from the echniocandins (
Figure 2) and is a semisynthetic derivative of the naturally occurring hemiacetal triterpene glycoside enfumafungin that incorporates a pyridine triazole at position 15 of the core phenanthropyran carboxylic acid ring system and a 2-amino- 2,3,3-trimethyl-butyl ether at position 14 to improve antifungal potency and pharmacokinetic properties
[2]. Compared with echinocandins, ibrexafungerp has the advantages of oral bioavailability, a larger volume of distribution, and its binding to the glucan synthase appears distinct from that of echinocandins, leading to retention of activity against most echinocandin-resistant isolates of
Candida spp., including those of
C. auris [3].
Figure 2. Molecular structures of caspofungin (left) and ibrexafungerp (right). Red structures indicate core structural components.
2. Pharmacokinetics
In animals, ibrexafungerp is absorbed by the gastrointestinal tract after oral administration with a bioavailability of approximately 35–50%. Importantly, ibrexafungerp is widely distributed in tissues and demonstrates excellent tissue penetration in sites commonly associated with invasive fungal infection, including (but not limited to) the lung, liver, kidney, spleen, and skin. Ibrexafungerp has poor penetration into the central nervous system in uninfected animals
[4] (
Table 1).
Ibrexafungerp is eliminated mainly via metabolism and biliary excretion with <2% of a dose recovered in urine. In vitro studies show that ibrexafungerp is metabolized via hydroxylation by CYP3A4 isoenzymes, followed by glucuronidation and sulfation of a hydroxylated inactive metabolite. Following oral administration of radio-labeled ibrexafungerp to healthy volunteers, a mean of 90% of the radioactive dose (51% as unchanged ibrexafungerp) was recovered in feces, and 1% was recovered in urine. The mean steady-state volume of distribution (V
ss) of ibrexafungerp in humans is approximately 600 L. Ibrexafungerp is highly protein-bound (greater than 99%), predominantly to albumin
[5][6]. A dose-proportional increase in the mean area under the concentration–time curve (AUC
0–∞) and peak concentration (C
max) occurred with single doses of 10 mg to 1600 mg within 4 to 6 h, and the mean terminal half-life was 20 to 30 h
[1]. The oral bioavailability of ibrexafungerp was increased with a high-fat meal, but absorption was delayed by administration with food
[1]. No clinically meaningful effect was observed on the corrected QT interval (QTcF), heart rate, PR, or QRS intervals at plasma ibrexafungerp concentrations up to 4000 ng/mL
[7]. Ibrexafungerp concentrations may be increased when administered with strong CYP3A4 inhibitors and dose adjustment may be needed. The coadministration of ibrexafungerp with CYP3A4 inducers is not recommended since it will decrease ibrexafungerp exposure
[6].
3. In Vitro Activity against Aspergillus species
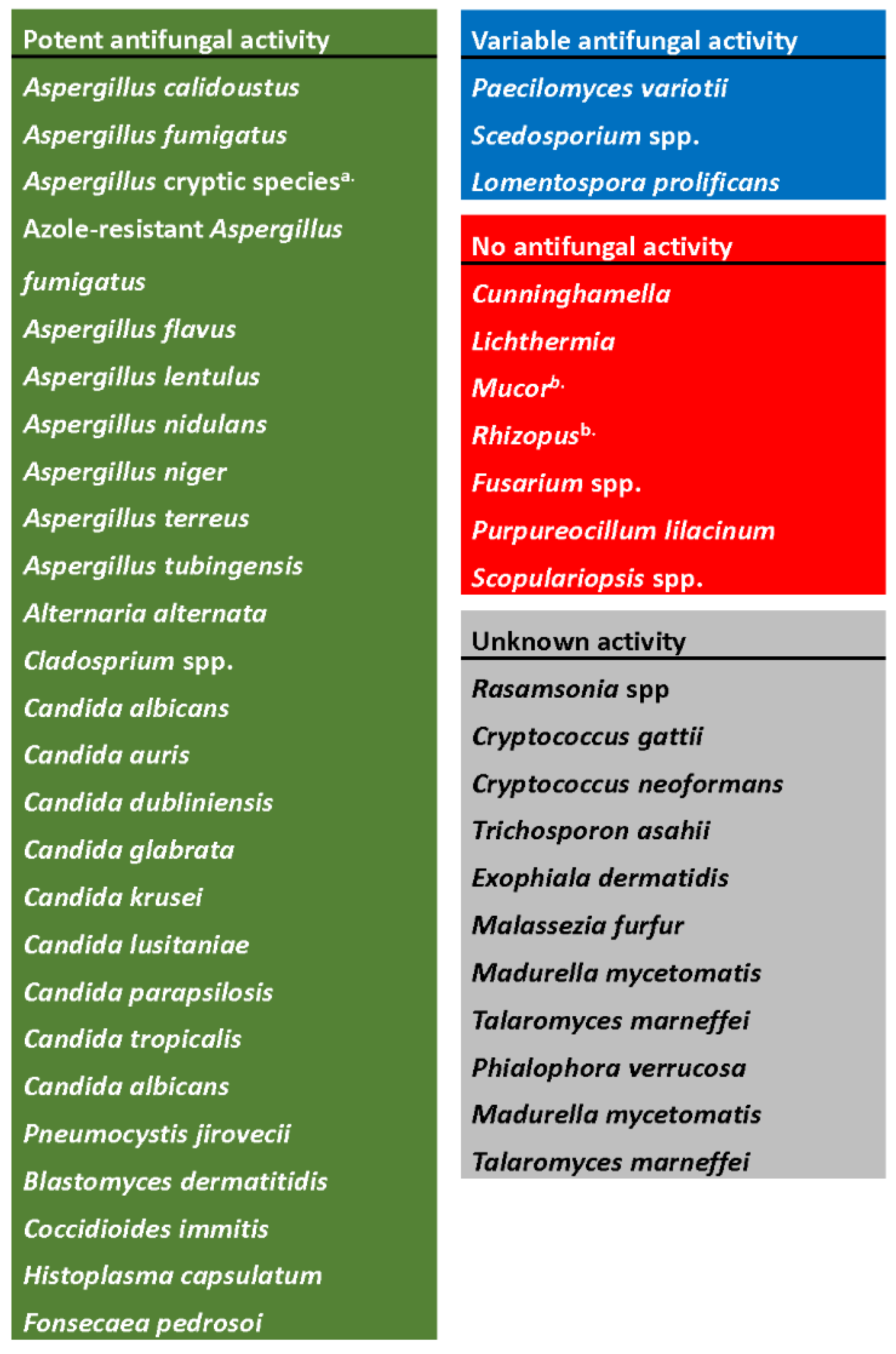
Ibrexafungerp has been extensively tested in vitro against a broad variety of fungal pathogens and has demonstrated potent activity against several isolates, with variable to weak activity against others (Figure 3).
Figure 3. In vitro spectrum of activity of ibrexafungerp. Figure adapted from Hoenigl, 2021
[8].
- a.
-
Includes A. fumigatiaffinis, A. thermomutatus, A. udagawae, A. hiratsukae, A. felis, A. citrinoterreus, A. carneus, A. aureoterreus, A. hortai, A. kevei, A. insuetus, A. ochraceus, and A. sclerotiorum.
- b.
-
No in vitro activity, although in vivo activity has been reported in animal models.
Glucan synthase inhibitors exhibit a fungistatic effect against many molds
[9][10], such as
Aspergillus spp., despite a high proportion of β-(1,3)-D-glucan in the Aspergillus cell wall
[9]. Because glucan synthase inhibitors exhibit a fungistatic effect against
Aspergillus, MIC values are not accurate; thus, minimum effective concentrations (MEC; the lowest concentration at which abnormal hyphal growth occurs) are used for antifungal susceptibility testing in both CLSI and EUCAST methods
[10].
In studies of in vitro susceptibility, ibrexafungerp demonstrated potent in vitro activity against
Aspergillus spp. Complexes including azole-resistant strains
[11][12][13][14]. The MEC of ibrexafungerp against a collection of
Aspergillus spp. (n = 311) ranged from <0.06 µg/mL to 4 µg/mL
[11]. The combinations of ibrexafungerp with voriconazole, amphotericin B, or isavuconazole were tested using a checkerboard combination test method against four strains of wild-type (WT) and two strains of azole-resistant
Aspergillus strains. The combination of ibrexafungerp with voriconazole or isavuconazole showed in vitro synergy against WT
Aspergillus spp. and was additive against azole-resistant strains. The combination of ibrexafungerp and amphotericin B were synergistic against both WT
Aspergillus spp. and azole-resistant strains
[11]. Similar results were observed in another study reporting that the combination of ibrexafungerp with isavuconazole resulted in a synergistic interaction in
A. fumigatus, measured by Bliss independence drug interaction analysis
[15].
The in vitro activity of ibrexafungerp combined with azole antifungals was evaluated against
Aspergillus spp. isolates from patients undergoing lung transplantation
[16]. The median MIC for azoles against all isolates was reduced by ≥4-fold when combined with ibrexafungerp, and the median MIC for ibrexafungerp also was reduced by ≥4-fold when combined with azoles against all isolated other than
A. calidoustus. A synergistic effect was observed for ibrexafungerp combined with isavuconazole (62%), posaconazole (54%), and voriconazole (53%). Among isolates with an ibrexafungerp or azole MIC < 0.06 µg/mL, combinations remained beneficial with ≥4-fold reduction in MIC for 75%, 50%, and 75% of isolates for isavuconazole, posaconazole, and voriconazole, respectively.
The in vitro activity of ibrexafungerp and other antifungal comparators was evaluated against
Aspergillus spp. clinical isolates that included both azole-susceptible and azole-resistant
A. fumigatus sensu stricto (s.s.) and cryptic species with varying degrees of antifungal resistance
[17]. The geometric mean MECs against
A. fumigatus s.s. with ibrexafungerp were 0.040 µg/mL for azole-susceptible strains versus 1.231 µg/mL and 0.660 µg/mL (EUCAST and CLSI) for voriconazole, respectively
[18][19]. Against azole-resistant strains, MECs were 0.092 µg/mL and 0.056 µg/mL (EUCAST and CLSI) with ibrexafungerp vs. 2.144 µg/mL and 2.000 µg/mL with voriconazole
[18][19]. Ibrexafungerp was also active against most cryptic species of
Aspergillus [18][19]. Ibrexafungerp exhibited moderate activity against the
A. ustus species complex, including
A. calidoustus,
A. insuetus, and
A. keveii, but was inactive against
A. alliaceus (MEC
90 ≥ 16 µg/mL). Overall, ibrexafungerp demonstrated in vitro activity against many
Aspergillus spp., including azole-susceptible and azole-resistant strains of
A. fumigatus.
Additionally, the in vitro activity of ibrexafungerp was examined against a selection of clinical isolates obtained from patients failing azole therapy for chronic pulmonary aspergillosis
[20]. The MEC was determined for 22
A. fumigatus complex, 3
A. flavus complex, and 1
A. niger complex isolates with resistance to at least 1 azole antifungal. The MEC range for ibrexafungerp was from 0.008 to 0.25 µg/mL. The ibrexafungerp MEC among isolates considered resistant to all azoles ranged from 0.015 to 0.25 µg/L. One isolate that was resistant to all azoles and amphotericin B was susceptible to ibrexafungerp (MEC 0.125 µg/mL).
4. In Vivo Activity against Aspergillus spp. in Animal Models of Infection
In neutropenic mice, ibrexafungerp demonstrated potent in vivo efficacy against wild-type (WT) and azole-resistant strains of
A. fumigatus when studied in a murine model of invasive aspergillosis
[21]. Treatment with oral ibrexafungerp at 7.5 mg/kg/day and 10 mg/kg/day BID significantly increased the mean survival in all strains (
p ≤ 0.003) and resulted in significant reductions in fungal kidney burden (
p < 0.05) and serum galactomannan levels (
p < 0.005). The exposure needed to achieve efficacy was similar to exposures reported in invasive candidiasis models.
The in vivo efficacy of ibrexafungerp combined with isavuconazole was examined in an experimental neutropenic rabbit model of invasive
A. fumigatus pneumonia
[15]. Ibrexafungerp 2.5 or 7.5 mg/kg/d IV or oral isavuconazole 40 mg/kg/d or their combination were administered. Ibrexafungerp and isavuconazole in combination demonstrated prolonged survival, decreased pulmonary injury, reduced residual fungal burden, and lower GMI and (1,3)-β-D-glucan levels in comparison to those of single therapy for the treatment of invasive pulmonary aspergillosis
 +1 credit
+1 credit