Myofascial pain syndrome (MPS) is thought to stem from masticatory muscle hypersensitivity. Masticatory myofascial pain syndrome (MMPS) is characterized by multiple trigger points (MTrPs), also known as hyperirritable points, in taut bands of affected muscles, regional muscle pain, or referred pain to nearby maxillofacial areas like teeth, masticatory muscles or the temporomandibular joint (TMJ). Muscle stiffness, reduced range of motion, muscle weakening without atrophy, and autonomic symptoms may accompany regional discomfort. Multiple treatments have been utilized to reduce trigger points and mandibular function restrictions. As a result of these incapacitating symptoms, MMPS can significantly impair many elements of quality of life. The application of Kinesio tape (KT) is a non-invasive method of treating dormant myofascial trigger points. Utilizing the body’s innate capacity for self-repair, this technique entails taping specific regions of the skin. KT alleviates discomfort, decreases swelling and inflammation, enhances or suppresses motor function in the muscles, stimulates proprioception, promotes lymphatic drainage, stimulates blood flow, and expedites tissue recovery.
1. Introduction
Myofascial pain syndrome is a multifactorial musculoskeletal disorder with a wide range of possible regionalized manifestations in terms of symptoms and severity. Masticatory myofascial pain syndrome (MMPS) is characterized by multiple trigger points (MTrPs), also known as hyperirritable points, in taut bands of affected muscles, regional muscle pain, or referred pain to nearby maxillofacial areas like teeth, masticatory muscles or the temporomandibular joint (TMJ). MMPS is frequently diagnosed in clinical practice, with a prevalence as high as 30% and a ratio of up to 85%
[1]. Despite their limitations, the Revised Diagnostic Criteria for Temporomandibular Disorders are the most widely used diagnostic guidelines for masticatory myofascial pain syndrome
[2][3][4][5].
A physical examination can quickly identify myofascial trigger points (MTrPs) inside a tight band of the afflicted muscle, probing which may elicit referral pain and a local twitch reaction. Muscle stiffness, reduced range of motion, muscle weakening without atrophy, and autonomic symptoms may accompany regional discomfort
[6][7][8]. As a result of these incapacitating symptoms, MMPS can significantly impair many elements of quality of life. Although the specific cause of MMPS is unknown, various risk factors for the disease’s development have been proposed, including acute muscle overload, trauma, poor posture, and psychological stress
[9][10]. As a result, a single therapy approach rarely entirely resolves the symptoms. Each patient needs individualized and multisectoral care to restore muscle strength and flexibility, deactivate MTrPs, and sustain pain management
[11][12]. MMPS treatment strategies are primarily divided into invasive and non-invasive techniques. Pharmacotherapy, acupuncture, electrotherapy, cold spray, manual therapies, stretching, ischemic compression, intraoral appliance therapy, and massage are non-invasive treatment techniques. Although invasive procedures such as trigger point injections and dry needling are preferred, they are not without risk
[13][14][15]. Predisposing variables must be eliminated, and structured exercise programs must be implemented for optimal MMPS management
[16][17]. Even with numerous therapies, the pain syndrome may not be alleviated.
The Kinesio Taping is a therapeutic tool that is used by rehabilitation specialists in all programs, including pediatric, geriatric, orthopedic, neurological, oncology, and others, as well as levels of acute care, inpatient rehabilitation, outpatient rehabilitation, home care, and Day Rehab
[18][19][20]. Among the many possible applications of Kinesio tape (KT) are the following: repairing damaged or weak muscles; accelerating recovery from musculoskeletal injuries; facilitating or inhibiting muscle activity; an increasing pain-free range of motion (ROM); boosting proprioception; providing soft tissue support; alleviating headaches and sinus pain; improving joint alignment; reducing swelling and edema; minimizing pain; managing lymphedema;
[21][22][23][24][25][26][27]. By microscopically lifting the skin, the KT therapeutic taping technique alleviates pain and facilitates lymphatic drainage. This lifting effect creates convolutions in the skin, expanding the interstitial space and reducing inflammation in the affected area. The Kinesio Taping (KT) technique has recently gained popularity for the treatment of sprains and strains sustained during athletic activities, postoperative complications, and various types of musculoskeletal injuries, including the management of pain. KT is a non-invasive procedure for releasing dormant MTrPs. This technique involves taping specific areas of the skin to stimulate the body’s natural ability to repair itself
[28][29]. Kinesiology taping’s effectiveness in alleviating the symptoms of musculoskeletal disorders has been widely documented and lauded, making it a go-to treatment option for both professional athletes and the public. KT as a therapeutic approach was initially published in the literature in 1969 as a valuable measure for elbow joint rehabilitation
[30][31][32]. KT has now acquired acceptance as a beneficial method in the treatment of acute and chronic musculoskeletal issues, such as pain, paresthesia, joint instability, and edema in many regions of the musculoskeletal system
[33]. The tape’s tension gradually elevates the skin, perhaps increasing lymphatic flow and diverting it to less congested routes
[34][35]. The significant effects of this technique are the restoration of muscular tension and improvements in small vessel blood circulation and lymph flow
[28][36]. Kinesio Taping (KT) has gained popularity for treating MTrPs because of its non-invasiveness, painlessness, and decreased time commitment
[37].
2. Kinesio Taping
2.1. Background of Kinesio Taping
Dr. Kenzo Kase, a Japanese chiropractor and acupuncturist, created Kinesio taping (KT) in 1973 to support the musculoskeletal system without excessive immobilization
[38][39]. Initially, the objective was to minimize swelling by regulating edema, supporting soft tissues, protecting joints, and reducing inflammation-caused heat
[21][40]. The main objective was to extend the benefits of manual therapy from the clinic to daily life at home and in other settings. After the Japanese athletics team used KT in the 1988 Olympics in Seoul, it attracted worldwide recognition and was imported to the US, where it gained popularity
[29]. MMPS, subacromial syndrome, hemiplegic shoulder, lymphedema, tendinitis, lateral epicondylitis, patellofemoral pain syndrome, and knee osteoarthritis are treated by KT
[30][34][35]. Previous research demonstrated post mandibular fracture surgery; KT reduced post-surgery swelling in the first two days
[41]. Despite its novelty as a tape method, few studies have examined it. Effectiveness in treating myofascial pain syndrome (MPS). The lack of data makes it hard to tell how different types of KT work on MMPS.
2.2. Characters of Kinesio Taping
Kinesio is woven cotton and elastic tape used to manage movement and accomplish functional goals. Kinesio Tape’s elastic fibers might be cotton or polyester. Tape is applied to the paper backing using an acrylic adhesive and 10–15% stretching
[42][43]. In Kinesio Taping, this strain is called “paper off tension”. This tape’s heat-sensitive acrylic adhesive and cotton-wrapped elastic core lessen the risk of latex allergy in children. The non-medicinal tape is water-resistant and may remain effective for 3 to 5 days. Waved designs may alternate proprioception and somatosensory inputs. The elastic tape may be easily trimmed to fit any body alignment
[29]. Kinesio Tape may stretch to 120–150% of its original length without stretching.
2.3. Types of Kinesio Taping
For humans, there are four Kinesio Tape varieties and two for animals. Clinicians pick tape based on the patient’s purpose and skin condition. Classic or Performance+ Tape is suggested for beginners. KT varies in size and form
[21][23][40].
Types of KT and its features and tape selection based on types of applications are mentioned in Table 1.
3. Mechanism of Action of Kinesio Taping
The skin is the body’s largest sensory organ and a key conduit for eliciting the appropriate motor responses. The required therapeutic motor impact can be achieved by applying the KT to certain skin sensory receptors
[29][30]. So, it alleviates discomfort, decreases swelling and inflammation, enhances or suppresses motor function in the muscles, stimulates proprioception, and promotes lymphatic drainage. When placed on the skin with minimal strain, KT raises the region under the skin and soft tissue to increase subcutaneous space, stimulate blood and lymph fluid circulation, expedite tissue recovery and channel fluid flow away from and into the damaged area to speed the recovery of wounded tissue. Varying the application and tension of the tape influence the body’s natural healing processes
[29][42].
Pain and abnormal sensations are minimized, muscles are supported, subcutaneous lymphatic fluid and blood are emptied, and joint derangement is repaired. This product lifts skin, improves space between muscles and skin, and reduces pressure. Reduced pressure diminishes subcutaneous pain receptor activation, allowing pain-free movement
[29][44]. Previous research showed the effect of tape on blood circulation to confirm that regular compression and decompression of the lymphatic system boosted flow and circulation
[29]. Negative-pressure pumping directs fluid from the superficial to deeper levels of the one-way lymphatic system beneath the skin
[29][41]. Muscle contraction and relaxation help create negative pressure. Intercellular junction shutters close as edema increases the interstitial pressure in the lymphatic system. Muscular contraction and relaxation, massage, and compression clothing may vary the pressure in each area. Lymph and interstitial fluid recirculation reduce swelling and pain. Lymph edema drains lesions and promotes tissue repair, improving circulation
[45][46].
Taping may affect proprioception, placebo effect, and biomechanics. Patients with patellofemoral pain syndrome may benefit from further KT
[47]. Gate control theory may explain KT’s pain-management benefits. Touch A-fiber diameter and conduction velocity are higher than pain A- and C-fibers. Mildly touching afferent skin receptors may activate glial spinal cells. The spinal cord blocks pain conduction to the brain
[11]. Although KT does not replace the need for exercise, it is recommended as an adjunctive strategy for the short term in the treatment of pain
[43]. Therefore, the KT tape is not to be used as the sole form of treatment, but rather as an alternative or complementary treatment when an immediate and short-duration effect by application is desired. Pairing with other methods and tools is recommended including manual therapy, muscle strengthening, electrothermal, and phototherapy
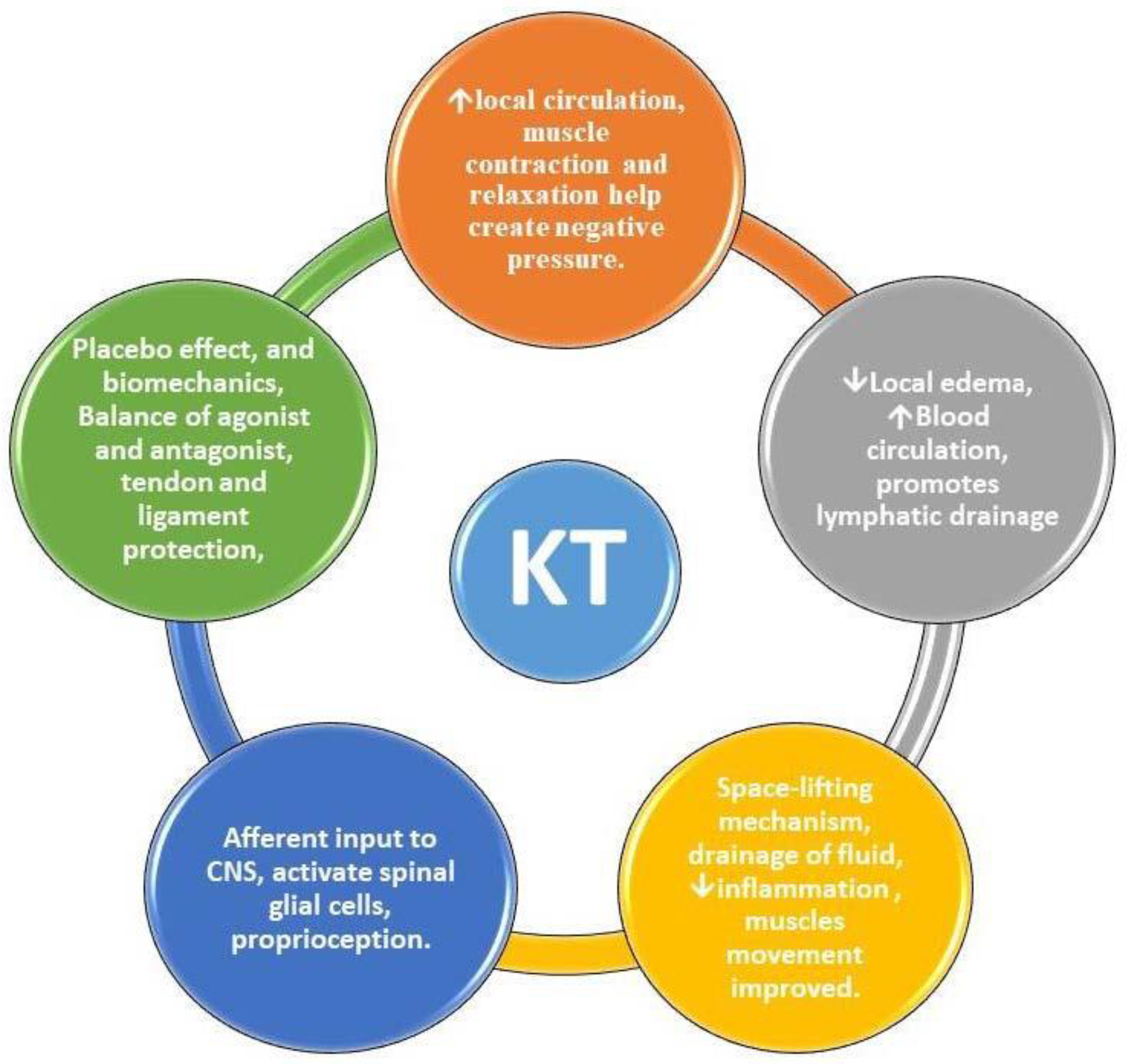
[48]. Kinesio taping may be the best treatment option for patients with myofascial pain syndrome, but more high-quality RCTs are needed to determine this at post-intervention and follow-up stages. Schematic diagrams represent the effects of KT application for MMPS in
Figure 1.
Figure 1. Effects of Kinesio taping on masticatory myofascial pain syndrome. CNS—central nervous system; KT—Kinesio taping.
 +1 credit
+1 credit