Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Jacinto Colan | -- | 1316 | 2022-12-08 15:20:07 | | | |
| 2 | Dean Liu | -4 word(s) | 1312 | 2022-12-09 09:20:56 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Colan, J.; Davila, A.; Hasegawa, Y. Tactile Displays for Conventional Laparoscopic Surgery. Encyclopedia. Available online: https://encyclopedia.pub/entry/38349 (accessed on 26 July 2026).
Colan J, Davila A, Hasegawa Y. Tactile Displays for Conventional Laparoscopic Surgery. Encyclopedia. Available at: https://encyclopedia.pub/entry/38349. Accessed July 26, 2026.
Colan, Jacinto, Ana Davila, Yasuhisa Hasegawa. "Tactile Displays for Conventional Laparoscopic Surgery" Encyclopedia, https://encyclopedia.pub/entry/38349 (accessed July 26, 2026).
Colan, J., Davila, A., & Hasegawa, Y. (2022, December 08). Tactile Displays for Conventional Laparoscopic Surgery. In Encyclopedia. https://encyclopedia.pub/entry/38349
Colan, Jacinto, et al. "Tactile Displays for Conventional Laparoscopic Surgery." Encyclopedia. Web. 08 December, 2022.
Copy Citation
Laparoscopic surgery (LS) is a minimally invasive technique that offers many advantages over traditional open surgery: it reduces trauma, scarring, and shortens recovery time. Researchers review the applications and challenges in the development of tactile feedback technologies that can be implemented with conventional laparoscopic instruments
tactile display
haptic feedback
laparoscopic surgery
1. Introduction
Laparoscopic surgery (LS) is a minimally invasive technique that offers many advantages over traditional open surgery: reduces trauma, scarring, and shortens recovery time. In LS, surgeons use an endoscope camera and long surgical instruments to access the anatomy of the patient through natural openings or keyhole incisions (5–12 cm in diameter) [1]. However, laparoscopic techniques have several drawbacks [2]. The images obtained from the endoscope camera are in most cases 2D, with loss of depth perception. Instruments pivot around the incision point, creating a mirror effect that requires the surgeon to move the instruments in the opposite direction, restricting range of motion, and contributing to poorer hand-eye coordination. Recent advances in the development of robotic-assisted surgery technologies have been shown to be effective in addressing these problems. Robotic systems can improve surgeon capabilities by providing magnified 3D vision with depth perception, highly dexterous surgical tools, and intuitive human–robot interfaces with improved ergonomics and high-precision tool motion control [3]. Robot-assisted surgery platforms have been developed for a wide range of surgical applications, including laparoscopic [4], endonasal [5][6], and ophthalmic [7] surgeries. The benefits of robot-assisted minimally invasive surgery (RMIS) come at the cost of being expensive, bulky, and time-consuming to set up [8]. Moreover, RMIS systems show a longer and steeper learning curve, as they are not widely available as compared to conventional laparoscopic instruments.
Despite the benefits obtained from RMIS techniques, an important limitation in LS remains: the loss of haptic sensation (force and tactile). Haptic information is important for the surgeon to discriminate between healthy and abnormal tissues, manipulate delicate tissues, and identify organs. Several studies have found a strong correlation between lack of haptic feedback and operational injuries. This limitation is acknowledged by the increasing number of studies on the development of tactile and force sensors. However, less interest has been found in the development of tactile feedback displays. Most of the proposed devices have been developed for RMIS, in which critical constraints, such as size, weight, or sterilibility, can be omitted because the surgeon is physically decoupled from the patient. Since RMIS is still far from being generally accessible, this survey focuses on recent progress in the development of tactile feedback technologies that can be implemented with conventional laparoscopic instruments.
2. Haptic Feedback in Minimally Invasive Surgery
Haptic feedback systems are commonly divided into two main types: kinesthetic or force feedback, and tactile or cutaneous feedback [9]. The difference lies in the feedback signal they provide [10]. Kinesthetic feedback provides the surgeon with information about the position, velocity, and force of objects. It relies on mechanoreceptors found within the joints and muscles. Traditional LS provides kinesthetic feedback to some extent through the transmission of forces along the shaft of the surgical tool. Tactile feedback provides information on a range of properties of surface tissues, such as temperature, pressure distribution, and texture, and is commonly termed the sense of touch. Humans obtained tactile information through stimulation (e.g., deep pressure, stretching, and vibrations) of mechanoreceptors located on the skin. Unlike kinesthetic feedback, in LS, the tactile feedback is completely lost. Compared to kinesthetic feedback, the display of tactile information is a significantly more difficult task due to the large number of tactile sensations available in human hands. Figure 1 shows the workflow of a tactile feedback system for laparoscopic surgery.
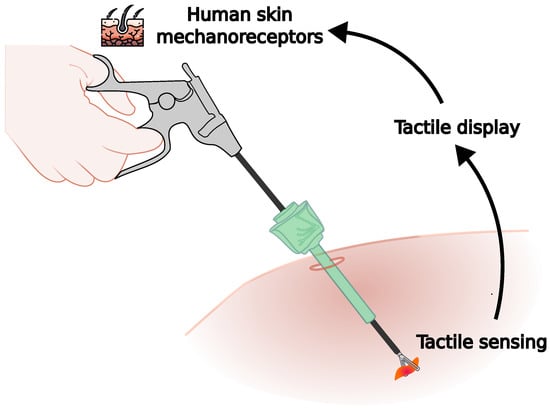
Figure 1. Tactile feedback in minimally invasive surgery. Tactile sensors convert the tactile stimuli into data sent to the tactile display, which recreate the same feedback sensation into the human skin mechanoreceptors.
In LS, it is important for the surgeon to recognize the consistencies, shapes, and structures of the tissue, and the lack of tactile feedback information represents an important challenge. Despite efforts to provide reliable tactile feedback in the surgical room, there is still no system ready for clinical applications [8].
2. Applications in Laparoscopic Surgery
Experimental results have shown that the addition of tactile feedback increases overall performance in common surgical tasks, with applications in palpation, tissue manipulation, suturing, and guidance tasks.
2.1. Palpation
Tumors are generally more rigid than surrounded tissues, and therefore a higher pressure intensity could be used for tumor detection. Most of the works included have focused on the palpation task to discriminate tissue stiffness. Rigid tactors have been proposed to reproduce stiffness as a normal force applied over the user’s finger, arm, or foot. The need to mount the actuators on the surgeon’s body, skin exposure, and minimal tactile information transmission could limit its applicability in real scenarios. In the case of vibrotactile feedback, specific vibration patterns appear to be more effective than others for the palpation task [11]. The benefits of using different patterns in other LS tasks remain unexplored. Furthermore, feedback gain is also an important parameter that should be adjusted according to the level of user perception [12]. Comparison studies between tactile feedback on the skin and visual tactile feedback showed a preference for visual display of tactile information. However, multimodal display, in which both forms of feedback are presented simultaneously, appears to be more effective [13][14].
2.2. Tissue manipulation
Manipulation of tissues and organs is based on a good estimation of their dynamic characteristics, such as stiffness and elasticity. Surgeons generally use grip force feedback to estimate these characteristics. Amplification of grip forces has been proposed [15] by innovative designs of compliant mechanisms without the need for a sensor. The reliability and robustness of the proposed design in real surgical scenarios still require further studies.
2.3. Suturing
Control of tension forces in suturing and knot tying tasks is required to avoid damaging delicate tissues. Stochastic resonance (SR) has been explored for this application [16]. The use of SR improved the participant’s assessment scores in terms of total score and needle position due to improvements in tactile sensitivity when holding a needle. However, experiments ex vivo did not show improvement in tissue damage and large-scale experiments are still required.
2.4. Guidance
Vibrotactile cues have also been explored to guide the movement of surgical tools along predefined constraints, for example, in the case of resection paths [13]. Well-tuned vibration patterns significantly improve performance in a guidance task. Only corrections are provided as vibrotactile information, and ways of including directional information have not yet been studied.
2.5. Challenges in the Development of Tactile Displays
In contrast to kinesthetic feedback, the complexity and various forms of tactile sensations make the development of tactile displays for LS quite challenging. To be implemented on conventional laparoscopic tools, tactile displays must overcome challenges similar to those for tactile sensing:
-
Transparency: The tactile display should provide tactile information to the surgeon in a natural and seamless way to avoid increasing the surgeon’s cognitive workload.
-
Compactability: Size of the tactile display must be able to be included in the surgical workspace without constraining the surgeon’s movement.
-
Weight: The weight of the display should not affect the manipulation of the surgical tool and should not increase the surgeon’s effort. The selection of external actuators and its location are critical to reduce the overall weight of the device.
-
Time delay: The time delay between tactile sensing and tactile feedback rendering reduces its effectiveness.
-
Safety: Forces generated must be kept within a safe range to avoid injuring the surgeon.
-
Adjustable: Each user requires different levels of stimulation, and adjustable perception is desirable.
-
Sterilizable: Tactile displays mounted close to the surgical workspace (e.g., surgical tool or surgeon’s hands) must be sterilized.
-
Reusability: To reduce costs, surgical instruments are commonly reused multiple times before being discarded. In the same way, tactile displays should be designed to last for many uses. Single-use devices could eliminate the need for cleaning or sterilization but increase costs and have a high environmental impact.
References
- Sieber, A.; Houston, K.; Woegerer, C.; Enoksson, P.; Menciassi, A.; Dario, P. Sensorized Tools for Haptic Force Feedback in Computer Assisted Surgery. In Haptics Rendering and Applications; Saddik, A.E., Ed.; IntechOpen: Rijeka, Croatia, 2012; Chapter 7.
- Xin, H.; Zelek, J.; Carnahan, H. Laparoscopic surgery, perceptual limitations and force: A review. In Proceedings of the First Canadian Student Conference on Biomedical Computing, Waterloo, ON, Canada, 2006; Volume 144.
- Freschi, C.; Ferrari, V.; Melfi, F.; Ferrari, M.; Mosca, F.; Cuschieri, A. Technical review of the da Vinci surgical telemanipulator. Int. J. Med. Robot. Comput. Assist. Surg. 2013, 9, 396–406.
- DiMaio, S.; Hanuschik, M.; Kreaden, U. The da Vinci surgical system. In Surgical Robotics; Springer: Berlin/Heidelberg, Germany, 2011; pp. 199–217.
- Colan, J.; Nakanishi, J.; Aoyama, T.; Hasegawa, Y. A Cooperative Human-Robot Interface for Constrained Manipulation in Robot-Assisted Endonasal Surgery. Appl. Sci. 2020, 10, 4809.
- Colan, J.; Nakanishi, J.; Aoyama, T.; Hasegawa, Y. Optimization-Based Constrained Trajectory Generation for Robot-Assisted Stitching in Endonasal Surgery. Robotics 2021, 10, 27.
- Koyama, Y.; Marinho, M.M.; Mitsuishi, M.; Harada, K. Autonomous Coordinated Control of the Light Guide for Positioning in Vitreoretinal Surgery. IEEE Trans. Med. Robot. Bionics 2022, 4, 156–171.
- Okamura, A.M. Haptics in robot-assisted minimally invasive surgery. In The Encyclopedia of Medical Robotics; Chapter 11; World Scientific: Singapore, 2019; pp. 317–339.
- See, A.R.; Choco, J.A.G.; Chandramohan, K. Touch, Texture and Haptic Feedback: A Review on How We Feel the World around Us. Appl. Sci. 2022, 12, 4686.
- Schostek, S.; Schurr, M.O.; Buess, G.F. Review on aspects of artificial tactile feedback in laparoscopic surgery. Med. Eng. Phys. 2009, 31, 887–898.
- Howard, T.; Szewczyk, J. Assisting control of forces in laparoscopy using tactile and visual sensory substitution. In New Trends in Medical and Service Robots; Springer: Berlin/Heidelberg, Germany, 2016; pp. 151–164.
- Tanaka, Y.; Nagai, T.; Fujiwara, M.; Sano, A. Lump detection with tactile sensing system including haptic bidirectionality. In Proceedings of the 2014 World Automation Congress (WAC), Waikoloa, HI, USA, 3–7 August 2014; pp. 77–82.
- Howard, T.; Szewczyk, J. Visuo-haptic feedback for 1D Guidance in laparoscopic surgery. In Proceedings of the 5th IEEE RAS/EMBS International Conference on Biomedical Robotics and Biomechatronics, Sao Paulo, Brazil, 12–15 August 2014; pp. 58–65.
- Howard, T.; Szewczyk, J. Improving precision in navigating laparoscopic surgery instruments toward a planar target using haptic and visual feedback. Front. Robot. AI 2016, 3, 37.
- Aguirre, M.E.; Kommuri, K.D.; Isbister, D.J.; Gallego, J.A. Multi-Modal Mechanism for Enhancing Haptics and Safety in Handheld Surgical Grasping. In Proceedings of the 2022 IEEE Haptics Symposium (HAPTICS), Santa Barbara, CA, USA, 21–24 March 2022; pp. 1–6.
- Sawada, H.; Egi, H.; Hattori, M.; Suzuki, T.; Mukai, S.; Kurita, Y.; Yasui, W.; Ohdan, H. Stochastic resonance enhanced tactile feedback in laparoscopic surgery. Surg. Endosc. 2015, 29, 3811–3818.
More
Information
Subjects:
Surgery
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
993
Revisions:
2 times
(View History)
Update Date:
09 Dec 2022
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No