 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Dean Liu | -- | 2060 | 2022-11-14 01:31:37 |
Video Upload Options
Abiraterone, also known as abiraterone acetate and sold under the brand name Zytiga among others, is a medication used to treat prostate cancer. Specifically it is used together with corticosteroid for metastatic castration-resistant prostate cancer (mCRPC) and metastatic high-risk castration-sensitive prostate cancer (mCSPC). It should either be used following removal of the testicles or along with a gonadotropin-releasing hormone (GnRH) analog. It is taken by mouth. Common side effects include tiredness, vomiting, headache, joint pain, high blood pressure, swelling, low blood potassium, high blood sugar, hot flashes, diarrhea, and cough. Other severe side effects may include liver failure and adrenocortical insufficiency. In males who partners can become pregnant, birth control is recommended. Supplied as abiraterone acetate it is converted in the body to abiraterone. Abiraterone works by suppressing the production of androgens – specifically it inhibits CYP17A1 – and thereby decreases the production of testosterone. In doing so, it prevents the effects of these hormones in prostate cancer. Abiraterone was described in 1995, and approved for medical use in the United States and Europe in 2011. It is on the World Health Organization's List of Essential Medicines, the safest and most effective medicines needed in a health system. In the United Kingdom it costs the NHS £2,735 a month as of 2018. In the United States this amount costs US$3,276 as of 2019. The medication is marketed widely throughout the world.
1. Medical Uses
1.1. Prostate Cancer
Abiraterone is used in combination with prednisone, a corticosteroid, as a treatment for mCRPC (previously called hormone-resistant or hormone-refractory prostate cancer).[1][2][3][4] This is a form of prostate cancer that is not responding to first-line androgen deprivation therapy or treatment with androgen receptor antagonists. Abiraterone has received Food and Drug Administration (FDA) (28 April 2011), European Medicines Agency (EMA) (23 September 2011), Medicines and Healthcare Products Regulatory Agency (MHRA) (5 September 2011) and Therapeutic Goods Administration (TGA) (1 March 2012) approval for this indication.[1][2][3][4] In Australia it is covered by the Pharmaceutical Benefits Scheme when being used to treat castration-resistant prostate cancer and given in combination with prednisone/prednisolone (subject to the conditions that the patient is not currently receiving chemotherapy, is either resistant or intolerant of docetaxel, has a WHO performance status of <2, and his disease has not since become progressive since treatment with PBS-subsidised abiraterone has commenced).[5]
Abiraterone may be useful for prevention of the testosterone flare at the initiation of GnRH agonist therapy in men with prostate cancer.[6]
In people previously treated with docetaxel survival is increased by 3.9 months (14.8 months versus 10.9 months for placebo).[7]
In people with castration-refractory prostate cancer but who had not received chemotherapy those who received abiraterone had a progression-free survival of 16.5 months rather than 8.3 months with placebo. After a median follow-up period of 22.2 months, overall survival was better with abiraterone.[8]
2. Contraindications
Contraindications include hypersensitivity to abiraterone. Although documents state that it should not be taken by women who are or who may become pregnant,[2][9] there is no medical reason that any woman should take it. Women who are pregnant should not even touch the pills unless they are wearing gloves.[9] Other cautions include severe baseline hepatic impairment, mineralocorticoid excess, cardiovascular disease including heart failure and hypertension, uncorrected hypokalemia, and adrenocorticoid insufficiency.[10]
3. Side Effects
Side effects by frequency:[1][2][3][4][10]
Very common (>10% frequency):
- Urinary tract infection
- Hypokalemia
- Hypertension
- Diarrhea
- Peripheral edema
Common (1-10% frequency):
- Hypertriglyceridaemia
- Sepsis
- Cardiac failure
- Angina pectoris
- Arrhythmia
- Atrial fibrillation
- Tachycardia
- Dyspepsia (indigestion)
- Rash
- Alanine aminotransferase increased
- Aspartate aminotransferase increased
- Fractures
- Hematuria
Uncommon (0.1-1% frequency):
- Adrenal insufficiency
- Myopathy
- Rhabdomyolysis
Rare (<0.1% frequency):
- Allergic alveolitis
4. Overdose
Experience with overdose of abiraterone is limited.[1] There is no specific antidote for abiraterone overdose, and treatment should consist of general supportive measures, including monitoring of cardiac and liver function.[1]
5. Interactions
Abiraterone is a CYP3A4 substrate and hence should not be administered concurrently with strong CYP3A4 inhibitors such as ketoconazole, itraconazole, clarithromycin, atazanavir, nefazodone, saquinavir, telithromycin, ritonavir, indinavir, nelfinavir, voriconazole) or inducers such as phenytoin, carbamazepine, rifampin, rifabutin, rifapentine, phenobarbital.[9][10] It also inhibits CYP1A2, CYP2C9, and CYP3A4 and likewise should not be taken concurrently with substrates of any of these enzymes that have a narrow therapeutic index.[9][10]
Spironolactone generally exerts anti-androgenic effects, but experimental evidence exists that it acts as an androgen receptor agonist in an androgen-depleted environment, capable of inducing prostate cancer proliferation.[11] This is supported by the observations described in several case reports.[12] Therefore, spironolactone should be avoided in prostate cancer people with treatment-associated mineralocorticoid side effects of abiraterone.
6. Pharmacology
6.1. Pharmacodynamics
Antiandrogenic activity
Abiraterone, the active metabolite of abiraterone acetate, inhibits CYP17A1, which manifests as two enzymes, 17α-hydroxylase (IC50 = 2.5 nM) and 17,20-lyase (IC50 = 15 nM) (approximately 6-fold more selective for inhibition of 17α-hydroxylase over 17,20-lyase)[13][14] that are expressed in testicular, adrenal, and prostatic tumor tissues. CYP17A1 catalyzes two sequential reactions: (a) the conversion of pregnenolone and progesterone to their 17α-hydroxy derivatives by its 17α-hydroxylase activity, and (b) the subsequent formation of dehydroepiandrosterone (DHEA) and androstenedione, respectively, by its 17,20-lyase activity.[15] DHEA and androstenedione are androgens and precursors of testosterone. Inhibition of CYP17A1 activity by abiraterone thus decreases circulating levels of androgens such as DHEA, testosterone, and dihydrotestosterone (DHT). Abiraterone acetate, via its metabolite abiraterone, has the capacity to lower circulating testosterone levels to less than 1 ng/dL (i.e., undetectable) when added to castration.[13][16] These concentrations are considerably lower than those achieved by castration alone (~20 ng/dL).[16] The addition of abiraterone to castration was found to reduce levels of DHT by 85%, DHEA by 97 to 98%, and androstenedione by 77 to 78% relative to castration alone.[16] In accordance with its antiandrogenic action, abiraterone decreases the weights of the prostate gland, seminal vesicles, and testes.[17]
Abiraterone also acts as a partial antagonist of the androgen receptor (AR), and as an inhibitor of the enzymes 3β-hydroxysteroid dehydrogenase (3β-HSD), CYP11B1 (steroid 11β-hydroxylase), CYP21A2 (Steroid 21-hydroxylase), and other CYP450s (e.g., CYP1A2, CYP2C9, and CYP3A4).[10][18][19][20] In addition to abiraterone itself, part of the activity of the drug has been found to be due to a more potent active metabolite, δ4-abiraterone (D4A), which is formed from abiraterone by 3β-HSD.[21] D4A is an inhibitor of CYP17A1, 3β-hydroxysteroid dehydrogenase/Δ5-4 isomerase, and 5α-reductase, and has also been found to act as a competitive antagonist of the AR reportedly comparable to the potent antagonist enzalutamide.[21] However, the initial 5α-reduced metabolite of D4A, 3-keto-5α-abiraterone, is an agonist of the AR, and promotes prostate cancer progression.[22] Its formation can be blocked by the coadministration of dutasteride, a potent and selective 5α-reductase inhibitor.[22]
Estrogenic activity
There has been interest in the use of abiraterone for the treatment of breast cancer due to its ability to lower estrogen levels.[23] However, abiraterone has been found to act as a direct agonist of the estrogen receptor, and induces proliferation of human breast cancer cells in vitro.[23] If abiraterone is used in the treatment of breast cancer, it should be combined with an estrogen receptor antagonist like fulvestrant.[23] In spite of its antiandrogenic and estrogenic properties, abiraterone does not appear to produce gynecomastia as a side effect.[24]
Other activities
Due to inhibition of glucocorticoid biosynthesis, abiraterone can cause glucocorticoid deficiency, mineralocorticoid excess, and associated adverse effects.[25] This is why the medication is combined with prednisone, a corticosteroid, which serves as a means of glucocorticoid replacement and prevents mineralocorticoid excess.[26]
Abiraterone, along with galeterone, has been identified as an inhibitor of sulfotransferases (SULT2A1, SULT2B1b, SULT1E1), which are involved in the sulfation of DHEA and other endogenous steroids and compounds, with Ki values in the sub-micromolar range.[27]
6.2. Pharmacokinetics
After oral administration, abiraterone acetate, the prodrug form in the commercial preparation, is converted into the active form, abiraterone. This conversion is likely to be esterase-mediated and not CYP-mediated. Administration with food increases absorption of the drug and thus has the potential to result in increased and highly variable exposures; the drug should be consumed on an empty stomach at least one hour before or two hours after food. The drug is highly protein bound (>99%), and is metabolised in the liver by CYP3A4 and SULT2A1 to inactive metabolites. The drug is excreted in feces (~88%) and urine (~5%), and has a terminal half-life of 12 ± 5 hours.[9]
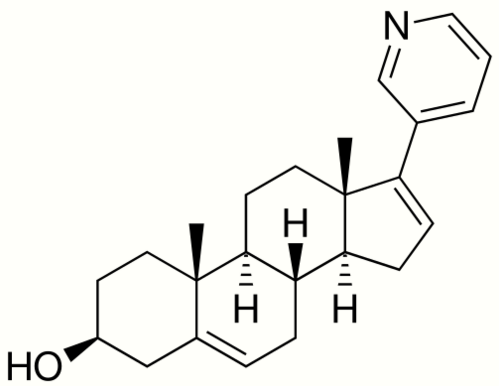
7. Chemistry
Abiraterone acetate, also known as 17-(3-pyridinyl)androsta-5,16-dien-3β-ol acetate, is a synthetic androstane steroid and a derivative of androstadienol (androsta-5,16-dien-3β-ol), an endogenous androstane pheromone. It is specifically a derivative of androstadienol with a pyridine ring attached at the C17 position and an acetate ester attached to the C3β hydroxyl group. Abiraterone acetate is the C3β acetate ester of abiraterone.
8. History
In the early 1990s, Mike Jarman, Elaine Barrie, and Gerry Potter of the Cancer Research UK Centre for Cancer Therapeutics in the Institute of Cancer Research in London set out to develop drug treatments for prostate cancer. With the nonsteroidal androgen synthesis inhibitor ketoconazole as a model, they developed abiraterone, filing a patent in 1993 and publishing the first paper describing it the following year.[28][29] Rights for commercialization of the drug were assigned to BTG, a UK-based specialist healthcare company. BTG then licensed the product to Cougar Biotechnology, which began development of the commercial product.[30] In 2009, Cougar was acquired by Johnson & Johnson, which developed and sells the commercial product, and is conducting ongoing clinical trials to expand its clinical uses.[31]
Abiraterone was approved by the United States Food and Drug Administration on 28 April 2011 for mCRPC.[32][33] The FDA press release made reference to a phase III clinical trial in which abiraterone use was associated with a median survival of 14.8 months versus 10.9 months with placebo; the study was stopped early because of the successful outcome.[34] Abiraterone was also licensed by the European Medicines Agency.[35] Until May 2012 the National Institute for Health and Clinical Excellence (NICE) did not recommend use of the drug within the NHS on cost-effectiveness grounds. This position was reversed when the manufacturer submitted revised costs.[36] The use is currently limited to men who have already received one docetaxel-containing chemotherapy regimen.[37][38] It was subsequently approved for the treatment of mCSPC in 2018.[39]
9. Society and Culture
9.1. Names
Abiraterone is the INN and BAN.[40][41] Abiraterone acetate is its USAN, BANM, and JAN.[40] It is also known by its developmental code names CB-7630 and JNJ-212082, while CB-7598 was the developmental code name of abiraterone.[40][42]
Abiraterone is marketed by Janssen Biotech (a subsidiary of Johnson & Johnson) under the brand name Zytiga,[40] and by Sun Pharmaceutical under the brand name Yonsa.[40]
Generic versions of abiraterone have been approved in the United States.[43] Generic versions of Yonsa are not available (As of November 2019).[44] In May 2019, the United States Court of Appeals for the Federal Circuit upheld a Patent Trial and Appeal Board decision invalidating a patent by Johnson & Johnson's on abiraterone.[45]
Intas Pharmaceuticals markets the drug under the brand name Abiratas, Cadila Pharmaceuticals markets the drug as Abretone, and Glenmark Pharmaceuticals as Abirapro. It is marketed as Yonsa by Sun Pharmaceutical Industries (licensed from Churchill Pharmaceuticals).[46][47]
9.2. Available Forms
Abiraterone is available in the form of 250 mg and 500 mg film-coated oral tablets and 250 mg uncoated oral tablets.[1] It is used at a dosage of 1,000 mg by mouth once per day an empty stomach, in conjunction with castration (via GnRH analogue therapy or orchiectomy) and in combination with 5 mg prednisone orally twice per day.[1]
Abiraterone is also available in the form of micronized 125 mg tablets used once per day at 500 mg in combination with methylprednisolone 4 mg taken twice per day with or without food.[48]
Abiraterone is marketed widely throughout the world, including in the United States, Canada, the United Kingdom, Ireland, elsewhere in Europe, Australia, New Zealand, Latin America, Asia, and Israel.[40]
9.3. Cost
In the United Kingdom it costs the NHS £2,735 a month as of 2018.[49] In the United States this amount costs US$3,276 as of 2019.[50] A generic version is available in India at a price of US$238 a month as of 2019.[51] The National Centre for Pharmacoeconomics initially found abiraterone to be not cost effective based on prices in 2012, however following the agreement to supply at a lower price it was accepted in 2014.[51]
10. Research
Abiraterone is under development for the treatment of breast cancer and ovarian cancer and as of March 2018, is in phase II clinical trials for these indications.[42] It was also under investigation for the treatment of congenital adrenal hyperplasia, but no further development has been reported for this potential use.[42]
References
- "ZYTIGA- abiraterone acetate tablet, film coated". 13 June 2019. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=4e338e89-3cf2-48eb-b6e2-a06c608c6513.
- "Zytiga EPAR". European Medicines Agency. 13 March 2019. https://www.ema.europa.eu/en/medicines/human/EPAR/zytiga.
- "ZYTIGA 500 mg film-coated tablets - Summary of Product Characteristics (SmPC)". electronic medicines compendium (emc). Datapharm. 4 March 2019. https://www.medicines.org.uk/emc/product/2381/smpc.
- "Zytiga abiraterone acetate product information" (PDF). TGA eBusiness Services. Janssen-Cilag Pty Ltd. 1 March 2012. https://www.ebs.tga.gov.au/ebs/picmi/picmirepository.nsf/pdf?OpenAgent&id=CP-2012-PI-01395-3.
- "Pharmaceutical Benefits Scheme - Abiraterone". Pharmaceutical Benefits Scheme. http://www.pbs.gov.au/medicine/item/2698B.
- "Strategies to Circumvent Testosterone Surge and Disease Flare in Advanced Prostate Cancer: Emerging Treatment Paradigms". J Natl Compr Canc Netw 13 (7): e49–55. July 2015. doi:10.6004/jnccn.2015.0109. PMID 26150586. https://dx.doi.org/10.6004%2Fjnccn.2015.0109
- "Abiraterone and increased survival in metastatic prostate cancer". The New England Journal of Medicine 364 (21): 1995–2005. May 2011. doi:10.1056/NEJMoa1014618. PMID 21612468. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=3471149
- "Abiraterone in metastatic prostate cancer without previous chemotherapy". The New England Journal of Medicine 368 (2): 138–48. January 2013. doi:10.1056/NEJMoa1209096. PMID 23228172. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=3683570
- "Zytiga prescribing information". Janssen Biotech. May 2012. http://www.zytigahcp.com/pdf/full_prescribing_info.pdf.
- "Zytiga (abiraterone) dosing, indications, interactions, adverse effects, and more". Medscape Reference. WebMD. http://reference.medscape.com/drug/zytiga-abiraterone-999651.
- "Androgenic activity of synthetic progestins and spironolactone in androgen-sensitive mouse mammary carcinoma (Shionogi) cells in culture". Journal of Steroid Biochemistry 31 (5): 845–52. November 1988. doi:10.1016/0022-4731(88)90295-6. PMID 2462135. https://dx.doi.org/10.1016%2F0022-4731%2888%2990295-6
- "Abiraterone and spironolactone in prostate cancer: a combination to avoid". Acta Clinica Belgica: 1–6. November 2018. doi:10.1080/17843286.2018.1543827. PMID 30477405. https://dx.doi.org/10.1080%2F17843286.2018.1543827
- Neidle, Stephen (30 September 2013). Cancer Drug Design and Discovery. Academic Press. pp. 341–342. ISBN 978-0-12-397228-6. https://books.google.com/books?id=HS6IAAAAQBAJ&pg=PA342.
- "Mechanism of the Dual Activities of Human CYP17A1 and Binding to Anti-Prostate Cancer Drug Abiraterone Revealed by a Novel V366M Mutation Causing 17,20 Lyase Deficiency". Pharmaceuticals 11 (2): 37. April 2018. doi:10.3390/ph11020037. PMID 29710837. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=6027421
- "Selective blockade of androgenic steroid synthesis by novel lyase inhibitors as a therapeutic strategy for treating metastatic prostate cancer". BJU International 96 (9): 1241–6. December 2005. doi:10.1111/j.1464-410X.2005.05821.x. PMID 16287438. https://dx.doi.org/10.1111%2Fj.1464-410X.2005.05821.x
- "Can targeting the androgen receptor in localized prostate cancer provide insights into why men with metastatic castration-resistant prostate cancer die?". Journal of Clinical Oncology 32 (33): 3689–91. November 2014. doi:10.1200/JCO.2014.57.8534. PMID 25311216. "Abiraterone acetate is a prodrug for abiraterone, a CYP17 inhibitor, which has the capacity to lower serum testosterone levels to less than 1 ng/dL (compared with levels closer to 20 ng/dL that are achieved with conventional ADT).19 [...] Relative to LHRHa alone, the addition of abiraterone resulted in an 85% decline in dihydrotestosterone (DHT) levels, a 97% to 98% decline in dehydroepiandrosterone (DHEA) levels, and a 77% to 78% decline in androstenedione levels.". https://dx.doi.org/10.1200%2FJCO.2014.57.8534
- Tindall, Donald J.; James, Mohler (20 April 2009). Androgen Action in Prostate Cancer. Springer Science & Business Media. pp. 748–. ISBN 978-0-387-69179-4. https://books.google.com/books?id=L6NMZizNLMoC&pg=PA748.
- "CYP17 inhibitors--abiraterone, C17,20-lyase inhibitors and multi-targeting agents". Nature Reviews. Urology 11 (1): 32–42. January 2014. doi:10.1038/nrurol.2013.274. PMID 24276076. https://dx.doi.org/10.1038%2Fnrurol.2013.274
- "CYP17A1 inhibitor abiraterone, an anti-prostate cancer drug, also inhibits the 21-hydroxylase activity of CYP21A2". The Journal of Steroid Biochemistry and Molecular Biology 174: 192–200. November 2017. doi:10.1016/j.jsbmb.2017.09.007. PMID 28893623. https://dx.doi.org/10.1016%2Fj.jsbmb.2017.09.007
- "Specificity of anti-prostate cancer CYP17A1 inhibitors on androgen biosynthesis". Biochemical and Biophysical Research Communications 477 (4): 1005–1010. September 2016. doi:10.1016/j.bbrc.2016.07.019. PMID 27395338. https://dx.doi.org/10.1016%2Fj.bbrc.2016.07.019
- "Conversion of abiraterone to D4A drives anti-tumour activity in prostate cancer". Nature 523 (7560): 347–51. July 2015. doi:10.1038/nature14406. PMID 26030522. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=4506215
- "Redirecting abiraterone metabolism to fine-tune prostate cancer anti-androgen therapy". Nature 533 (7604): 547–51. May 2016. doi:10.1038/nature17954. PMID 27225130. PMC 5111629. https://dash.harvard.edu/bitstream/handle/1/29626087/5111629.pdf?sequence=1.
- "The CYP17A1 inhibitor abiraterone exhibits estrogen receptor agonist activity in breast cancer". Breast Cancer Research and Treatment 157 (1): 23–30. May 2016. doi:10.1007/s10549-016-3774-3. PMID 27083183. https://dx.doi.org/10.1007%2Fs10549-016-3774-3
- "Multimodality treatment of gynecomastia in patients receiving antiandrogen therapy for prostate cancer in the era of abiraterone acetate and new antiandrogen molecules". Oncology 84 (2): 92–9. 2013. doi:10.1159/000343821. PMID 23128186. https://dx.doi.org/10.1159%2F000343821
- Figg, William D.; Chau, Cindy H.; Small, Eric J. (14 September 2010). Drug Management of Prostate Cancer. Springer Science & Business Media. p. 97. ISBN 978-1-60327-829-4. https://books.google.com/books?id=4KDrjeWA5-UC&pg=PA97.
- Rosenthal, Laura; Burchum, Jacqueline (17 February 2017). Lehne's Pharmacotherapeutics for Advanced Practice Providers - E-Book. Elsevier Health Sciences. pp. 936. ISBN 978-0-323-44779-9. https://books.google.com/books?id=gfYoDgAAQBAJ&pg=PA936.
- "Identification of Galeterone and Abiraterone as Inhibitors of Dehydroepiandrosterone Sulfonation Catalyzed by Human Hepatic Cytosol, SULT2A1, SULT2B1b, and SULT1E1". Drug Metabolism and Disposition 46 (4): 470–482. April 2018. doi:10.1124/dmd.117.078980. PMID 29436390. https://dx.doi.org/10.1124%2Fdmd.117.078980
- "Where did abiraterone come from?". Cancer Research UK. 2011-09-21. http://scienceblog.cancerresearchuk.org/2011/09/21/where-did-abiraterone-come-from/.
- "A new way to treat prostate cancer: The story of abiraterone". The Institute of Cancer Research. 2012-09-10. http://www.icr.ac.uk/press/recent_featured_articles/Story_Abiraterone/index.shtml.
- "Abiraterone Acetate (CB7630)". Cougar Biotechnology. Archived from the original. Error: If you specify |archiveurl=, you must also specify |archivedate=. https://web.archive.org/web/20080907194739/http://www.cougarbiotechnology.com/cb7630.html.
- "Johnson & Johnson Announces Definitive Agreement to Acquire Cougar Biotechnology, Inc" (Press release). Cougar Biotechnology. 2009-05-11. Archived from the original on 2009-05-29. Retrieved 2009-06-03. https://web.archive.org/web/20090529115329/http://www.cougarbiotechnology.com/pr052109.html
- "Drugs@FDA - FDA Approved Drug Products - Zytiga". https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=202379.
- "FDA approves Zytiga for late-stage prostate cancer" (Press release). Food and Drug Administration (FDA). 2011-04-28. Archived from the original on 2017-01-12. https://wayback.archive-it.org/7993/20170112024032/https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm253055.htm
- "FDA Approval for Abiraterone Acetate". U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute. http://www.cancer.gov/cancertopics/druginfo/fda-abirateroneacetate.
- "EMA assessment of Zytiga (abiraterone)". European Medicines Agency. http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/002321/human_med_001499.jsp&mid=WC0b01ac058001d124.
- "Prostate cancer (metastatic, castration resistant) - abiraterone (following cytoxic therapy): final appraisal determination guidance". NICE guidance. 15 May 2012. http://www.nice.org.uk/nicemedia/live/13484/59217/59217.pdf.
- "NICE technology appraisal guidance [TA259]". NICE guidance. June 2012. http://www.nice.org.uk/guidance/ta259/chapter/1-guidance.
- "NICE appraisal of earlier treatment with abiraterone for prostate cancer". NICE press release. 14 August 2014. http://www.nice.org.uk/nice-appraisal-of-earlier-treatment-with-abiraterone-for-prostate-cancer.
- NCI Staff. "Abiraterone Approved for Earlier Use in Men with Metastatic Prostate Cancer". National Cancer Institute (NCI). https://www.cancer.gov/news-events/cancer-currents-blog/2018/abiraterone-fda-prostate-hormone-sensitive.
- "Abiraterone". Drugs.com. https://www.drugs.com/international/abiraterone.html.
- "abiraterone". https://mednet-communities.net/inn/db/ViewINN.aspx?i=7375.
- "Abiraterone acetate - Johnson & Johnson". Adis Insight. http://adisinsight.springer.com/drugs/800005133.
- "Generic Zytiga Availability". Drugs.com. https://www.drugs.com/availability/generic-zytiga.html.
- "Generic Yonsa Availability". Drugs.com. https://www.drugs.com/availability/generic-yonsa.html.
- "BTG International Limited v. Amneal Pharmaceuticals LLC". United States Court of Appeals for the Federal Circuit. 2019-05-14. http://www.cafc.uscourts.gov/node/24791.
- "Sun Pharma Gets FDA Go-Ahead for Yonsa for Prostate Cancer". https://www.biospace.com/article/sun-pharma-gets-fda-go-ahead-for-yonsa-for-prostate-cancer/.
- "Sun Pharma Announces USFDA Approval of YONSA (abiraterone acetate) To Treat Metastatic Castration-Resistant Prostate Cancer In Combination With Methylprednisolone" (Press release). Sun Pharmaceutical Industries Limited/Churchill Pharmaceuticals. 23 May 2018. Archived from the original on 15 November 2019. Retrieved 14 November 2019 – via Business Wire. https://www.businesswire.com/news/home/20180522006497/en/Sun-Pharma-Announces-USFDA-Approval-YONSA%C2%AE-abiraterone
- "YONSA- abiraterone acetate tablet". 5 June 2018. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=b8967e10-f768-47ce-ac9e-2324c8390132.
- British national formulary : BNF 76 (76 ed.). Pharmaceutical Press. 2018. pp. 921. ISBN 9780857113382.
- "Abiraterone Prices, Coupons & Patient Assistance Programs" (in en). https://www.drugs.com/price-guide/abiraterone.
- "PROPOSAL FOR THE INCLUSION OF ENZALUTAMIDE AND ABIRATERONE ACETATE IN THE WHO MODEL LIST OF ESSENTIAL MEDICINES FOR THE TREATMENT OF METASTATIC CASTRATION RESISTANT PROSTATE CANCER". p. 22, 25. https://www.who.int/selection_medicines/committees/expert/22/applications/8.3_enzalutamide-abiraterone.pdf. Retrieved 26 November 2019.

