Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Mustapha Benkhalifa | -- | 1751 | 2022-11-02 09:53:27 | | | |
| 2 | Vivi Li | -1 word(s) | 1750 | 2022-11-03 02:28:47 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Benkhalifa, M.; Joao, F.; Duval, C.; Montjean, D.; Bouricha, M.; Cabry, R.; Bélanger, M.; Bahri, H.; Miron, P.; Benkhalifa, M. Endometrium Immunomodulation in Assisted Reproductive Technology. Encyclopedia. Available online: https://encyclopedia.pub/entry/32488 (accessed on 27 July 2026).
Benkhalifa M, Joao F, Duval C, Montjean D, Bouricha M, Cabry R, et al. Endometrium Immunomodulation in Assisted Reproductive Technology. Encyclopedia. Available at: https://encyclopedia.pub/entry/32488. Accessed July 27, 2026.
Benkhalifa, Mustapha, Fabien Joao, Cynthia Duval, Debbie Montjean, Molka Bouricha, Rosalie Cabry, Marie-Claire Bélanger, Hatem Bahri, Pierre Miron, Moncef Benkhalifa. "Endometrium Immunomodulation in Assisted Reproductive Technology" Encyclopedia, https://encyclopedia.pub/entry/32488 (accessed July 27, 2026).
Benkhalifa, M., Joao, F., Duval, C., Montjean, D., Bouricha, M., Cabry, R., Bélanger, M., Bahri, H., Miron, P., & Benkhalifa, M. (2022, November 02). Endometrium Immunomodulation in Assisted Reproductive Technology. In Encyclopedia. https://encyclopedia.pub/entry/32488
Benkhalifa, Mustapha, et al. "Endometrium Immunomodulation in Assisted Reproductive Technology." Encyclopedia. Web. 02 November, 2022.
Copy Citation
After more than four decades of assisted reproductive technology (ART) practice worldwide, more than 60% of women undergoing in vitro fertilization (IVF) treatments fail to become pregnant after the first embryo transfer and nearly 20% of patients are suffering from unexplained recurrent implantation failures (RIFs) and repeated pregnancy loss (RPL). The literature reported different causes of RIF–RPL, mainly multifactorial, endometrial and idiopathic. RIF remains a black box because of the complicated categorization and causes of this physio-pathological dysregulation of implantation and pregnancy process after ovarian stimulation. Many options were suggested as solutions to treat RIF–RPL with controversial results on their usefulness.
infertility
assisted reproductive technology
implantation failure
endometrium immunomodulation
1. Introduction
In assisted reproductive technology (ART) programs, 60–70% of women fail to become pregnant after embryo transfer. Repeated implantation failure (RIF) remains a black box in daily practice due to the complicated categorization and causes of this physio-pathological dysregulation [1]. Different causes of RIF were reported, mainly multifactorial, endometrial and idiopathic. Multifactorial RIF can be caused by maternal and paternal factors, gamete and embryo quality, infections and lifestyle changes in combination with psychological status and oxidative stress [1][2]. Impaired endometrium function such as abnormal growth or loss of vascularization can account for endometrial RIF, but idiopathic RIF, caused mainly by abnormal cross-talk between the embryo and endometrium, remains the principal question and needs to be elucidated [1].
RIF may be defined as a failure to obtain a pregnancy after multiple viable embryo transfers during IVF treatment [3], but its definition is inconsistent between studies. The most common definition was portrayed by Bashiri and colleagues [4] who describe RIF as three or more pregnancy failures following the transfer of at least three good-quality embryos [4]. However, other authors such as Coughlan and colleagues [5] suggest including maternal age, number of embryos transferred and number of previous cycles to the definition of RIF [5]. Interestingly, a consensus is emerging thanks to a recent extensive survey. It was proposed to define RIF as the failure to achieve a clinical pregnancy after 2–3 IVF cycles with 1–4 good-quality embryos [6]. RIF is a challenge for clinicians as its etiology includes various possible causes [2].
The causes of RIF can be divided into two categories: maternal (uterine anatomic abnormalities, chronic endometritis, non-receptive endometrium, antiphospholipid antibody syndrome and immunological factors) and embryonic (genetic defects and other factors specific to embryonic development) causes [3]. In the absence of male factors, oxidative stress, bad-quality embryos and anatomical abnormalities such as hydro-salpinx and thrombophilia, RIF seems to be caused by impaired endometrial function such as abnormal endometrial growth or loss of vascularization [4]. However, RIF caused by immunological factors could be manageable using several innovative therapeutic options. Among them, intrauterine administration of human chorionic gonadotropin (HCG), granulocyte colony-stimulating factor (G-CSF) or autologous peripheral blood mononuclear cells (PBMCs) has been suggested as a treatment for patients suffering from RIF [4][7][8][9][10][11][12][13][14][15][16].
2. Endometrium Immunomodulation via Intrauterine Insemination of Activated Autologous Peripheral Blood Mononuclear Cells (PBMCs)
PBMCs from patients with RIF are usually isolated during the ovulation period using a lymphocyte separation medium composed of an iso-osmotic poly-sucrose and sodium diatrizoate solution to separate mononuclear cells (including B-lymphocytes, T-lymphocytes and monocytes) from the other blood cells. After separation, PBMCs are generally activated with hCG or corticotropin-releasing hormone (CRH) and cultured in vitro for 24–72 h in a humidified incubator with 5% CO2 at 37 °C (Figure 1).
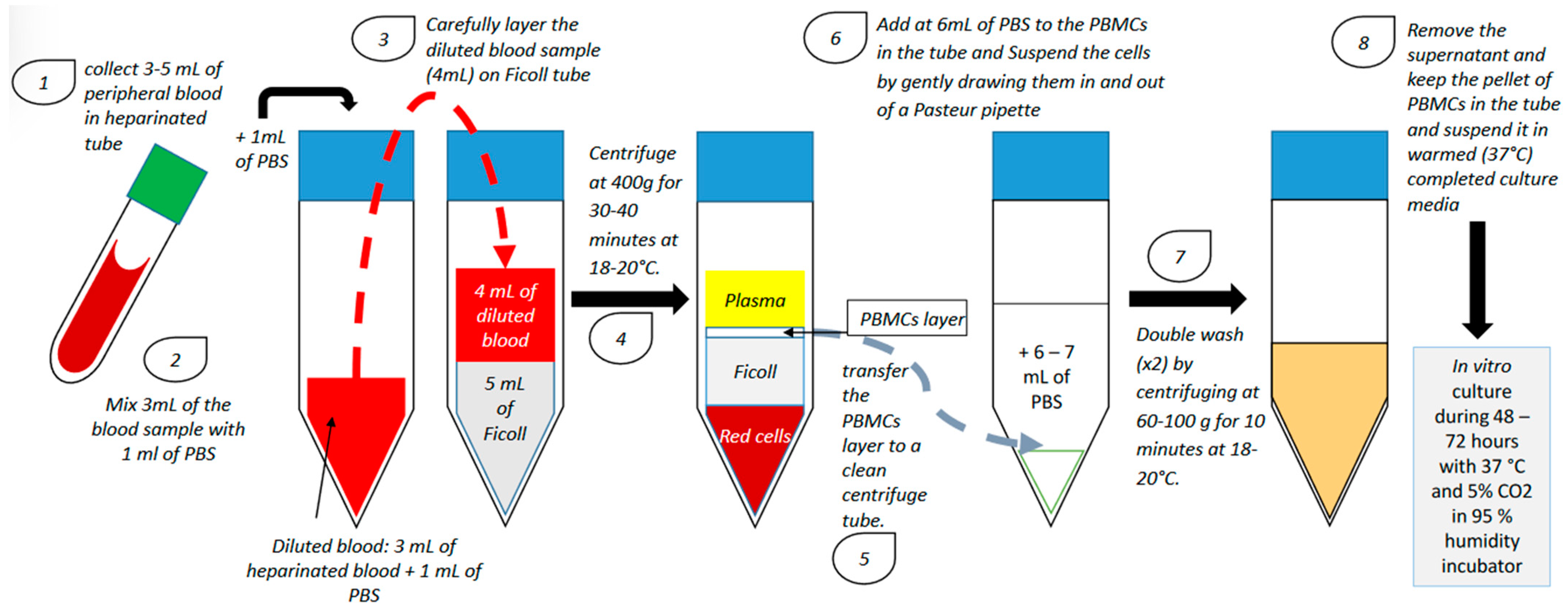
Figure 1. PBMC isolation technique and in vitro culture (PBS: phosphate-buffered saline; PBMC: peripheral blood mononuclear cell).
After culture, PBMCs are administered in utero using a catheter [4][7][8][9][10][11][12][13][14][15]. However, the number of cells administered in utero is not homogeneous among all studies investigating the use of PBMC in the treatment of RIF (Table 1). Although there were some methodological variations between studies in terms of the number of previous cycles, cycle type, and number and quality of transferred embryos, patients were generally administered with 10 to 30 million PBMCs [7][8][9][10][11][12][13][14][15][16]. Madkour and colleagues showed a significant increase in clinical pregnancy rate (CPR) with only 1 million cells [10]. Furthermore, in a recent meta-analysis, Qin and colleagues have demonstrated that CPR was higher when less than 100 million PBMCs/mL were administered in utero, suggesting that although the quantity of cells inseminated is not homogeneous, intrauterine administration of PBMC does appear to be an effective treatment for patients suffering from RIF [17].
Table 1. Main studies using PBMCs to treat RIF.
| Study | Number of Previous Failed IVF Cycles | Sample Size | Day of Blood Collection | PBMCs Co-cultured with | Duration of PBMC Culture | Number of PBMCs Administered In Utero | Transfer Type | Stage of Embryo | Implantation Rate (Control vs. Case) | Clinical Pregnancy Rate (Control vs. Case) | Miscarriage Rate (Control vs. Case) | Live Birth Rate (Control vs. Case) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control | Case | ||||||||||||
| Yoshioka et al., 2006 [7] | ≥4 | 18 | 17 | On the day of oocyte retrieval | hCG: 5 IU/mL | 48 h | 20 × 106 | Fresh | 1, 2 or 3 blastocysts | 4.1% vs. 23.4% (p = 0.0034) | 11.1% vs. 41.2% (p = 0.042) | Not specified | 7.6% vs. 55.6% (p = 0.013) |
| Okitsu et al., 2011 [16] | ≥1 | 170 | 83 | On the day following ovulation or the day after | Not activated | No culture | 30 × 106 | Frozen/ thawed |
early cleavage embryo or blastocyst | ≥1 RIF: 21.1% vs. 21.6% (ns); 3 RIF: 9.38% vs. 25.0% (p = 0.041) | ≥1 RIF: 32.9% vs. 34.9% (ns); ≥3 RIF: 16.7% vs. 42.1% (p = 0.039) | Not specified | ≥ 1 RIF: 21.8% vs. 21.7% (ns); ≥3 RIF: 11.1% vs. 21.2% (ns) |
| Makrigiannakis et al., 2015 [9] | ≥3 | 45 | 45 | On the day of oocyte retrieval | CRH: 107 M/1.106 cells/mL | 48 h | 20 × 106 + 107 CRH | Fresh | 2 or 3 blastocysts (grade 3BB and above) | Not specified | 0% vs. 44.44% (p < 0.001) | Not specified | Not specified |
| Madkour et al., 2016 [10] | ≥2 | 27 | 27 | On the day of ovulation induction | Complete culture medium + 75 IU of hMG | 72 h | 1 × 106 | Fresh | 1, 2 or 3 early cleavage embryos | ≥2 RIF: 9% vs. 22% (p = 0.02); 2 RIF vs. ≥ 3 RIF: 15% vs. 35% (p = 0.09) | ≥2 RIF: 15% vs. 44% (p = 0.045); 2 RIF vs. ≥ 3 RIF: 29% vs. 70% (p = 0.04) | ≥2 RIF: 17% vs. 75% (p = 0.08) 2 RIF vs. ≥ 3 RIF: 20% vs. 14% (p = 0.8) | Not specified |
| Yu et al., 2016 [11] | ≥3 | 105 | 93 | On the day following ovulation | hCG: 10 IU/mL | 24 h | 10–20 × 106 | Frozen/ thawed |
early cleavage embryo | 11.43% vs. 23.66% (p < 0.05) | 20.95% vs. 46.24% (p < 0.05) | 31.8% vs. 20.9% (ns) | 14.28% vs. 34.41% (p < 0.05) |
| Li et al., 2017 [12] | ≥1 | 339 | 294 | Two days before embryo transfer | hCG: 10 IU/mL | 24 h | 10–20 × 106 | Fresh and frozen/ thawed |
2 or 3 early cleavage embryos or 2 or 3 grade 2 blastocysts at day 5 and 3BB and above at day 6 | 1 RIF: 32.33% vs. 29.35% (ns); 2 RIF: 27.74% vs. 35.98% (p = 0.048); 3 RIF: 26.23% vs. 23.20% (ns); ≥4 RIF: 4.88% vs. 22.00% (p = 0.014) | 1 RIF: 41.23% vs. 43.75% (ns); 2 RIF: 42.18% vs. 48.15% (p = 0.016); 3 RIF: 36.84% vs. 42.22% (ns); ≥4 RIF: 14.29% vs. 39.58% (p = 0.038) | Not specified | 1 RIF: 36.84% vs. 37.5% (ns); 2 RIF: 33.33% vs. 34.26% (ns); 3 RIF: 24.56% vs. 28.89% (ns); ≥4 RIF: 9.58% vs. 33.33% (p = 0.038) |
| Makrigiannakis et al., 2019 [13] | ≥3 | 26 | 26 | On the day of oocyte retrieval | CRH: 107 M/1.106 cells/mL | 48 h | 20 × 106 + 107 M CRH | Fresh | 2 or 3 grade 1 or 2 early cleavage embryos | Not specified | 0% vs. 57,69% (p < 0.01) | Not specified | Not specified |
| Nobijari et al., 2019 [15] | ≥1 | 128 | 122 | 5 days before the frozen/thawed embryo transfer | CRH (concentration not specified) | 48–72 h | 20 × 106 + 107 M CRH | Frozen/ thawed |
early cleavage embryo or blastocyst | Not specified | <3 RIF: 30.4% vs. 30.8% (p = 0.91); ≥3 RIF: 19,7% vs. 38,6% (p = 0.01) | Not specified | Not specified |
| Pourmoghadam et al., 2020 [14] | ≥3 | 50 | 50 | On the day of ovulation induction | hCG: 10 IU/mL daily | 48 h | 15–20 × 106 | Frozen/ thawed |
early cleavage embryo or blastocyst | Not specified | 22% vs. 42% (p = 0.032) | 24% vs. 8% (p = 0.029) | 20% vs. 38% (p = 0.047) |
CRH: corticotropin-releasing hormone; hCG: human chorionic gonadotropin; RIF: recurrent implantation failure.
3. Immunoregulation of the Endometrium during Embryo Implantation: Biological Function and Molecular Pathway
To achieve successful embryo implantation and pregnancy, an appropriate dialogue between the embryo and the endometrium must take place [18].
In the uterine environment, a particular form of natural killer (NK) cells with a unique transcriptional profile, the uterine NK (uNK) cells, represents the most abundant lymphocyte population, especially in the endometrium [19][20][21]. In fact, most of the immune cells present in the uterus usually display a unique phenotype [18]. Peripheral blood NK cells express CD56+CD16+ at their membrane surface and are characterized by a highly cytotoxic profile [22]. However, uNK cells are less toxic since they do not express CD16 on their membrane surface [23]. During the menstrual cycle, levels of uNK cells start to increase in the mid-secretory phase, which could explain their importance in embryo implantation [24][25][26][27].
Dendritic cells (DCs), another type of innate immune cells, have a crucial role in the site of embryo implantation and maternal–fetal interface. DCs act as antigen-presenting cells to T cells and have the unique ability to induce a primary immune response, a phenomenon crucial for successful pregnancy [28]. In addition, DCs can influence trophoblast invasion by regulating the secretion of cytokines and the production of endometrial cell-surface proteins. Through the regulation of immune cell functions and actions, DCs have a major role in the establishment of a special local immune environment essential for embryo implantation and placental development [29]. Human decidual DCs, however, seem to have an immature phenotype characterized by a low expression of CD40, CD80, CD86 and CD205 [30][31]. DCs seem to be involved in the immune tolerance of the implantation site through the regulation of T-cell proliferation and the elimination of antigen-specific T cells. In the decidua, uterine dendritic cells (uDCs) are also crucial in maintaining pregnancy [32]. Since the 1990s, it has been known that maternal T cells are essential to the complex mechanisms of immune tolerance, a phenomenon critical to the invasion of the endometrium by the blastocyst [33].
T-cell interactions can be performed directly by cell–cell contact or indirectly through the secretion of pro-inflammatory or anti-inflammatory cytokines [34]. Pro-inflammatory cytokines such as interleukin (IL)-1β, -6, -12, -2 and -18; tumor necrosis factor alpha (TNF-α) and interferon gamma (IFN-γ) are mainly produced by T helper (Th) 1 cells, while anti-inflammatory cytokines such as IL-4, IL-10, IL-13 and TGF-β1 are mostly secreted by Th2 cells [35]. The pro-inflammatory Th1 profile was shown to be associated with successful and normal pregnancy at early and late pregnancy stages. In the midgestation stage, however, a shift to an anti-inflammatory Th2 profile must take place to establish tolerance to the foreign fetal antigens [36]. An imbalance in these cytokine profiles has been associated with spontaneous abortion and common complications of pregnancy [37][38][39]. Moreover, it has been shown that levels of pro-inflammatory cytokines (such as IL-2 and IFN-γ) decreased while levels of anti-inflammatory cytokines (such as IL-4 and IL-10) increased in the induction of immune tolerance to allografts [40][41]. The implication of T cells, especially CD4+ CD25+ Foxp3+ Treg cells, in the initial stages of pregnancy is therefore needed for the prevention of an alloreactivity action by the endometrium against the fetus through cascades of immunoregulation actions [42][43].
Treg, Th1 and Th2 cells are, however, not the only T-cell subtypes known to be crucial for successful embryo implantation. Th17 cells, a subset of T cells showing remarkable plasticity, are also indispensable in the immunoregulation of embryo implantation as well as in maintaining normal pregnancy [44].
Monocytes and macrophages also play an important role during the menstrual cycle and pregnancy [14][45][46]. Macrophages regulate trophoblast activity by promoting endometrial tissue remodeling and angiogenesis [47]. Pregnancy hormones directly and indirectly modulate the recruitment of monocytes in the uterus and participate in their differentiation and stimulation into functional macrophages [48]. Intrauterine administration of PBMCs could also be a source of hCG-activated macrophages and regulate the uterine environment at the embryo implantation site [14].
References
- Benkhalifa, M.; Zayani, Y.; Bach, V.; Copin, H.; Feki, M.; Benkhalifa, M.; Allal-Elasmi, M. Does the dysregulation of matrix metalloproteinases contribute to recurrent implantation failure? Expert Rev. Proteom. 2018, 15, 311–323.
- Busnelli, A.; Somigliana, E.; Cirillo, F.; Baggiani, A.; Levi-Setti, P.E. Efficacy of therapies and interventions for repeated embryo implantation failure: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 1747.
- Simon, A.; Laufer, N. Repeated implantation failure: Clinical approach. Fertil. Steril. 2012, 97, 1039–1043.
- Bashiri, A.; Halper, K.I.; Orvieto, R. Recurrent Implantation Failure-update overview on etiology, diagnosis, treatment and future directions. Reprod. Biol. Endocrinol. 2018, 16, 121.
- Coughlan, C.; Ledger, W.; Wang, Q.; Liu, F.; Demirol, A.; Gurgan, T.; Cutting, R.; Ong, K.; Sallam, H.; Li, T.C. Recurrent implantation failure: Definition and management. Reprod. Biomed. Online 2014, 28, 14–38.
- Cimadomo, D.; Craciunas, L.; Vermeulen, N.; Vomstein, K.; Toth, B. Definition, diagnostic and therapeutic options in recurrent implantation failure: An international survey of clinicians and embryologists. Hum. Reprod. 2021, 36, 305–317.
- Yoshioka, S.; Fujiwara, H.; Nakayama, T.; Kosaka, K.; Mori, T.; Fujii, S. Intrauterine administration of autologous peripheral blood mononuclear cells promotes implantation rates in patients with repeated failure of IVF-embryo transfer. Hum. Reprod. 2006, 21, 3290–3294.
- Bielfeld, A.P.; Pour, S.J.; Poschmann, G.; Stühler, K.; Krüssel, J.S.; Baston-Büst, D.M. A Proteome Approach Reveals Differences between Fertile Women and Patients with Repeated Implantation Failure on Endometrial Level⁻Does hCG Render the Endometrium of RIF Patients? Int J. Mol. Sci. 2019, 2, 425.
- Makrigiannakis, A.; BenKhalifa, M.; Vrekoussis, T.; Mahjub, S.; Kalantaridou, S.N.; Gurgan, T. Repeated implantation failure: A new potential treatment option. Eur. J. Clin. Investig. 2015, 45, 380–384.
- Madkour, A.; Bouamoud, N.; Louanjli, N.; Kaarouch, I.; Copin, H.; Benkhalifa, M.; Sefrioui, O.; Madkour, L. Intrauterine insemination of cultured peripheral blood mononuclear cells prior to embryo transfer improves clinical outcome for patients with repeated implantation failures. Zygote 2016, 24, 58–69.
- Yu, N.; Zhang, B.; Xu, M.; Wang, S.; Liu, R.; Wu, J.; Yang, J.; Feng, L. Intrauterine administration of autologous peripheral blood mononuclear cells (PBMCs) activated by HCG improves the implantation and pregnancy rates in patients with repeated implantation failure: A prospective randomized study. Am. J. Reprod. Immunol. 2016, 76, 212–216.
- Li, S.; Wang, J.; Cheng, Y.; Zhou, D.; Yin, T.; Xu, W.; Yu, N.; Yang, J. Intrauterine administration of hCG-activated autologous human peripheral blood mononuclear cells (PBMC) promotes live birth rates in frozen/thawed embryo transfer cycles of patients with repeated implantation failure. J. Reprod. Immunol. 2017, 119, 15–22.
- Makrigiannakis, A.; Vrekoussis, T.; Makrygiannakis, F.; Ruso, H.; Kalantaridou, S.N.; Gurgan, T. Intrauterine CRH-treated PBMC in repeated implantation failure. Eur. J. Clin. Investig. 2019, 49, e13084.
- Pourmoghadam, Z.; Soltani-Zangbar, M.S.; Sheikhansari, G.; Azizi, R.; Eghbal-Fard, S.; Mohammadi, H.; Siahmansouri, H.; Aghebati-Maleki, L.; Danaii, S.; Mehdizadeh, A.; et al. Intrauterine administration of autologous hCG- activated peripheral blood mononuclear cells improves pregnancy outcomes in patients with recurrent implantation failure; A double-blind, randomized control trial study. J. Reprod. Immunol. 2020, 142, 103182.
- Nobijari, F.F.; Arefi, S.S.; Moini, A.; Taheripanah, R.; Fazeli, E.; Kharazi, H.; Hosseini, S.Z.; Hosseini, A.; Valojerdi, M.R.; Copin, H. Endometrium immunomodulation by intrauterine insemination administration of treated peripheral blood mononuclear cell prior frozen/thawed embryos in patients with repeated implantation failure. Zygote 2019, 27, 214–218.
- Okitsu, O.; Kiyokawa, M.; Oda, T.; Miyake, K. Intrauterine administration of autologous blood mononuclear cells increases clinical pregnancy rates in frozen/thawed embryo transfer cycles of patients with repeated implantation failure. J. Reprod. Immunol. 2011, 92, 82–87.
- Qin, Q.; Chang, H.; Zhou, S.; Zhang, S.; Yuan, D.; Yu, L.L.; Qu, T. Intrauterine administration of peripheral blood mononuclear cells activated by human chorionic gonadotropin in patients with repeated implantation failure: A meta-analysis. J. Reprod. Immunol. 2021, 145, 103323.
- Zenclussen, A.C.; Hämmerling, G.J. Cellular regulation of the uterine microenvironment that enables embryo implantation. Front. Immunol. 2015, 6, 321.
- King, A.; Balendran, N.; Wooding, P.; Carter, N.P.; Loke, Y.W. CD3- leukocytes present in the human uterus during early placentation: Phenotypic and morphologic characterization of the CD56++ population. Dev. Immunol. 1991, 1, 169–190.
- Koopman, L.A.; Kopcow, H.D.; Rybalov, B.; Boyson, J.E.; Orange, J.S.; Schatz, F.; Masch, R.; Lockwood, C.J.; Schachter, A.D.; Park, P.J.; et al. Human decidual natural killer cells are a unique NK cell subset with immunomodulatory potential. J. Exp. Med. 2003, 198, 1201–1212.
- Mori, M.; Bogdan, A.; Balassa, T.; Csabai, T.; Szekeres-Bartho, J. The deciduas-the maternal bed embracing the embryo-maintains the pregnancy. Semin. Immunopathol. 2016, 38, 635–649.
- Poli, A.; Michel, T.; Thérésine, M.; Andrès, E.; Hentges, F.; Zimmer, J. CD56bright natural killer (NK) cells: An important NK cell subset. Immunology 2009, 126, 458–465.
- Mandal, A.; Viswanathan, C. Natural killer cells: In health and disease. Hematol. Oncol. Stem Cell Ther. 2015, 8, 47–55.
- Timeva, T.; Shterev, A.; Kyurkchiev, S. Recurrent Implantation Failure: The Role of the Endometrium. J. Reprod. Infertil. 2014, 15, 173–183.
- Helige, C.; Ahammer, H.; Hammer, A.; Huppertz, B.; Frank, H.G.; Dohr, G. Trophoblastic invasion in vitro and in vivo: Similarities and differences. Hum. Reprod. 2008, 23, 2282–2291.
- Wallace, A.E.; Fraser, R.; Cartwright, J.E. Extravillous trophoblast and decidual natural killer cells: A remodelling partnership. Hum. Reprod. Update 2012, 18, 458–471.
- Lee, J.Y.; Lee, M.; Lee, S.K. Role of endometrial immune cells in implantation. Clin. Exp. Reprod. Med. 2011, 38, 119–125.
- Huang, X.; Venet, F.; Chung, C.S.; Lomas-Neira, J.; Ayala, A. Changes in dendritic cell function in the immune response to sepsis: Cell- & tissue-based therapy. Expert Opin. Biol. Ther. 2007, 7, 929–938.
- Gellersen, B.; Brosens, J.J. Cyclic decidualization of the human endometrium in reproductive health and failure. Endocr. Rev. 2014, 35, 851–905.
- Péguet-Navarro, J.; Dalbiez-Gauthier, C.; Rattis, F.M.; Van Kooten, C.; Banchereau, J.; Schmitt, D. Functional expression of CD40 antigen on human epidermal Langerhans cells. J. Immunol. 1995, 155, 4241–4247.
- Rattis, F.M.; Péguet-Navarro, J.; Staquet, M.J.; Dezutter-Dambuyant, C.; Courtellemont, P.; Redziniak, G.; Schmitt, D. Expression and function of B7-1 (CD80) and B7-2 (CD86) on human epidermal Langerhans cells. Eur. J. Immunol. 1996, 26, 449–453.
- Tagliani, E.; Erlebacher, A. Dendritic cell function at the maternal–fetal interface. Expert Rev. Clin. Immunol. 2011, 7, 593–602.
- Tafuri, A.; Alferink, J.; Möller, P.; Hämmerling, G.J.; Arnold, B. T cell awareness of paternal alloantigensduring pregnancy. Science 1995, 270, 630–633.
- Hudic, I.; Fatušic, Z. Progesterone-induced blocking factor (PIBF) and Th1/Th2 cytokine in women with threatened spontaneous abortion. J. Perinat. Med. 2009, 37, 338–342.
- Kaiko, G.E.; Horvat, J.C.; Beagley, K.W.; Hansbro, P.M. Immunological decision-making: How does the immune system decide to mount a helper T-cell response? Immunology 2008, 123, 326–338.
- Mor, G.; Cardenas, I.; Abrahams, V.; Guller, S. Inflammation and pregnancy: The role of the immune system at the implantation site. Ann. N. Y. Acad. Sci. 2011, 1221, 80–87.
- Jena, M.K.; Nayak, N.; Chen, K.; Nayak, N.R. Role of Macrophages in Pregnancy and Related Complications. Arch. Immunol. Ther. Exp. 2019, 67, 295–309.
- Deshmukh, H.; Way, S.S. Immunological Basis for Recurrent Fetal Loss and Pregnancy Complications. Annu. Rev. Pathol. 2019, 14, 185–210.
- Liang, P.Y.; Diao, L.H.; Huang, C.Y.; Lian, R.C.; Chen, X.; Li, G.G.; Zhao, J.; Li, Y.Y.; He, X.B.; Zeng, Y. The pro-inflammatory and anti-inflammatory cytokine profile in peripheral blood of women with recurrent implantation failure. Reprod. Biomed. Online 2015, 31, 823–826.
- Robertson, S.A.; Care, A.S.; Moldenhauer, L.M. Regulatory T cells in embryo implantation and the immune response to pregnancy. J. Clin. Investig. 2018, 128, 4224–4235.
- Von Wolff, M.; Thaler, C.J.; Strowitzki, T.; Broome, J.; Stolz, W.; Tabibzadeh, S. Regulated expression of cytokines in human endometrium throughout the menstrual cycle: Dysregulation in habitual abortion. Mol. Hum. Reprod. 2000, 6, 627–634.
- Ahmadi, M.; Abdolmohammadi-Vahid, S.; Ghaebi, M.; Aghebati-Maleki, L.; Dolati, S.; Farzadi, L.; Ghasemzadeh, A.; Hamdi, K.; Younesi, V.; Nouri, M.; et al. Regulatory T cells improve pregnancy rate in RIF patients after additional IVIG treatment. Syst. Biol. Reprod. Med. 2017, 63, 350–359.
- Teles, A.; Schumacher, A.; Kühnle, M.C.; Linzke, N.; Thuere, C.; Reichardt, P.; Tadokoro, C.E.; Hämmerling, G.J.; Zenclussen, A.C. Control of uterine microenvironment by foxp3 (+) cells facilitates embryo implantation. Front. Immunol. 2013, 4, 158.
- Saito, S.; Nakashima, A.; Shima, T.; Ito, M. Th1⁄Th ⁄Th17 and regulatory T-cell paradigm in pregnancy. Am. J. Reprod. Immunol. 2010, 63, 601–610.
- Tedesco, S.; Adorni, M.P.; Ronda, N.; Cappellari, R.; Mioni, R.; Barbot, M.; Pinelli, S.; Plebani, M.; Bolego, C.; Scaroni, C.; et al. Activation profiles of monocyte-macrophages and HDL function in healthy women in relation to menstrual cycle and in polycystic ovary syndrome patients. Endocrine 2019, 66, 360–369.
- Faas, M.M.; Spaans, F.; De Vos, P. Monocytes and macrophages in pregnancy and pre-eclampsia. Front. Immunol. 2014, 5, 298.
- Cervar, M.; Blaschitz, A.; Dohr, G.; Desoye, G. Paracrine regulation of distinct trophoblast functions in vitro by placental macrophages. Cell Tissue Res. 1999, 295, 297–305.
- Tonello, A.; Poli, G. Tubal ectopic pregnancy: Macrophages under the microscope. Hum. Reprod. 2007, 22, 2577–2584.
More
Information
Subjects:
Reproductive Biology
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
891
Revisions:
2 times
(View History)
Update Date:
08 Nov 2022
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No