Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Roberto Arrigoni | -- | 1384 | 2022-10-31 15:31:48 | | | |
| 2 | Catherine Yang | Meta information modification | 1384 | 2022-11-01 02:07:21 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Arrigoni, R.; Ballini, A.; Topi, S.; Bottalico, L.; Jirillo, E.; Santacroce, L. Overcome Antibiotic Resistance against Mycobacterium tuberculosis. Encyclopedia. Available online: https://encyclopedia.pub/entry/32126 (accessed on 09 June 2026).
Arrigoni R, Ballini A, Topi S, Bottalico L, Jirillo E, Santacroce L. Overcome Antibiotic Resistance against Mycobacterium tuberculosis. Encyclopedia. Available at: https://encyclopedia.pub/entry/32126. Accessed June 09, 2026.
Arrigoni, Roberto, Andrea Ballini, Skender Topi, Lucrezia Bottalico, Emilio Jirillo, Luigi Santacroce. "Overcome Antibiotic Resistance against Mycobacterium tuberculosis" Encyclopedia, https://encyclopedia.pub/entry/32126 (accessed June 09, 2026).
Arrigoni, R., Ballini, A., Topi, S., Bottalico, L., Jirillo, E., & Santacroce, L. (2022, October 31). Overcome Antibiotic Resistance against Mycobacterium tuberculosis. In Encyclopedia. https://encyclopedia.pub/entry/32126
Arrigoni, Roberto, et al. "Overcome Antibiotic Resistance against Mycobacterium tuberculosis." Encyclopedia. Web. 31 October, 2022.
Copy Citation
Tuberculosis (TB) is an infectious disease caused by the bacillus Mycobacterium tuberculosis (Mtb). TB treatment is based on the administration of three major antibiotics: isoniazid, rifampicin, and pyrazinamide. However, multi-drug resistant (MDR) Mtb strains are increasing around the world, thus, allowing TB to spread around the world. The stringent response is demonstrated by Mtb strains in order to survive under hostile circumstances, even including exposure to antibiotics. The stringent response is mediated by alarmones, which regulate bacterial replication, transcription and translation. Moreover, the Mtb cell wall contributes to the mechanism of antibiotic resistance along with efflux pump activation and biofilm formation.
antibiotics
antibiotic resistance
immunity
microbiota
multi-drug resistant Mycobacterium tuberculosis strains
1. Probiotics
There is evidence that antibiotics against TB alter the gut and pulmonary microbiota [1]. Moreover, antibiotic-mediated dysbiosis may affect the microbiota–immune axis, thus, aggravating the clinical course of TB and increasing the risk of reinfection [2][3]. Probiotics have been identified by the WHO as “Living microorganisms that when administered in adequate amounts as a part of food confer a health benefit to the host” [4]. Just recently, the bactericidal activity of probiotics has been demonstrated to suppress a few antibiotic-resistant superbugs and, therefore, attempts have been made to apply them against tuberculosis [5]. In general terms, probiotics are able to increase the protective effect of the intestinal epithelial barrier, also shifting the immune profile towards a tolerogenic pathway with the production of IL-10 by TREG cells [6][7].
Experimentally, the probiotic Nyaditum resae® (Nr), enriched in heat-killed Mycobacterium manresensis, abrogated the development of active murine TB, through increasing the function of memory TREG cells [8]. Furthermore, Nr effects were evaluated in patients with or without latent TB infection and an increase in T effector cells and memory TREG cells was observed [9]. Lacticaseibacillus rhamnosus PMC203, isolated from the vaginal microbiota of healthy women has been shown to exhibit an effective killing of drug-sensitive and drug-resistant Mtb infecting RAW macrophages, also inhibiting Mtb growth under broth culture medium [10]. L. casei supplemented to TB patients for four weeks led to a dramatic reduction of TNF-alpha, IL-6, IL-10, and IL-12, with an up-regulation of metabolites, such as phosphatidylserine, maresin 1, and phosphatidylcholine [11]. L. crispatus, isolated from the vaginal microbiota of healthy women, reduced the growth of MtbH37Rv in broth, and MtbH37Rv and Mtb XDR TBs in macrophages [12].
2. Polyphenols
Polyphenols are natural products largely contained in fruits, vegetables, cereals, red wine, and extra virgin olive oil [13]. They are endowed with antioxidant, anti-inflammatory, and microbicidal activities and, therefore, they are currently used in the prevention or treatment of chronic disease [14]. In fact, polyphenols exert their anti-inflammatory activity either inhibiting the NF-kB pathway with reduced expression of pro-inflammatory cytokines or activating TREG cells with the enhanced expression of the anti-inflammatory cytokine IL-10.
The use of polyphenols in the treatment of TB has been poorly investigated. A mixed flavonoid mixture treatment of TPH-1 infected macrophages and human granuloma reduced the intracellular survival of Mtb and increased granuloma formation, with higher levels of IL-12 and IFN-gamma, and lower levels of IL-10 [15]. Polyphenols, extracted from Areca catechu and enriched in catechin, epicatechin, and epigallocatechin, were able to inhibit Mtb growth [16]. Polyphenols extracted from the roots of Anogeissus (A.) leiocarpa could inhibit Mycobacterium smegmatis growth in view of high concentration of ellagic acid derivatives, ellagitannins, and flavonoids [17]. Clinical data support the use of A. leiocarpa in the treatment of cough related to TB. A saponin-polybrophenol antibiotic (CU1), extracted from Cassia fistula inhibited transcription from Mtb polymerases, and its ethanol extract was very effective against MDR bacteria [18]. Sirtuin (Sirt) 1 is a NAD-dependent deacetylase, that is able to inhibit apoptosis and inflammation in human cells [19]. Resveratrol, a non-flavonoid polyphenol, is a Sirt 1 activator, which abrogated Mtb-induced apoptosis in peritoneal macrophages [20]. Furthermore, Sirt 1 inhibited Mtb growth, enhancing GSK3 beta phosphorylation, thus, inducing its deacylation. Therefore, Sirt 1 can be considered as potential anti-TB agent. The use of natural products as anti-TB agents is described in Figure 1.
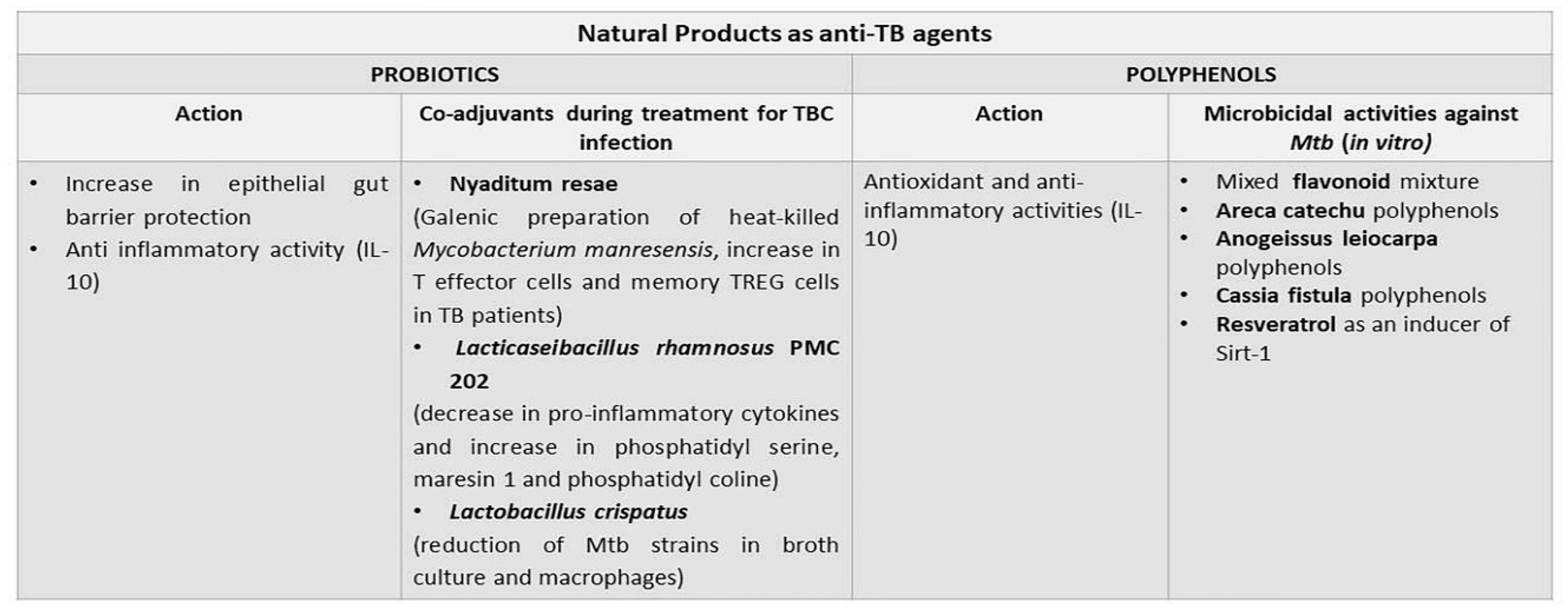
Figure 1. Potential use of natural products as anti-TB agents. Both probiotics and polyphenols have been experimented with as anti-TB pharmaceuticals. Probiotics can modulate the gut–lung axis that is compromised in the course of TB. Polyphenols exert anti-TB microbicidal activity in vitro and their application in human TB needs to be better explored.
3. Antimicrobial Peptides
AMPs have been shown to act as antimicrobial compounds alone or in combination with other drugs [21][22][23][24]. In general terms, they are cationic with less than 50 amino acid residues. Additionally, synthetic analogues are more effective than natural AMPs demonstrating a lower minimum inhibitory concentration [25]. AMPs act through different modalities: i. Disruption of bacterial membrane with formation of pores or via electroporation; ii. Interaction with bacterial components and cell death induction; iii. Inhibition of cell wall biosynthesis; iv. Antimicrobial activity mediated via the activation of the innate immune system [26][27][28]. Cathelicidins, human defensins, and lactoferrin (LF) are the major categories of AMPs. LL-37 is a human cathelicidin, that is able to bind to the negatively charged outer leaflet of the microbial membrane, leading to its disruption [29]. In addition, LL-37 exerts its microbicidal activity against Mtb via modulation of the innate immune response [30]. In the course of Mtb infection, LL-37 was expressed following the up-regulation of the vitamin D receptor, as well as after oral administration of phenylbutyrate and vitamin D3, with reduction of the intracellular burden of Mtb [31][32]. Of note, LL-37 stimulation of infected macrophages led to the production of anti-inflammatory cytokines, IL-10 and TGF-beta, thus, suggesting a modulation of the immune response in the earlier phase of Mtb infection [33]. Among analogues of AMPs, acyl depsipeptides (ADEPs) seem to represent a future generation of antibiotics against tuberculosis [34]. ADEPs exert antibacterial activity on Mtb strains through activation of the caseinolytic protease ClpP1P2. Biotherapeutics for the treatment of TB are indicated in Figure 2.
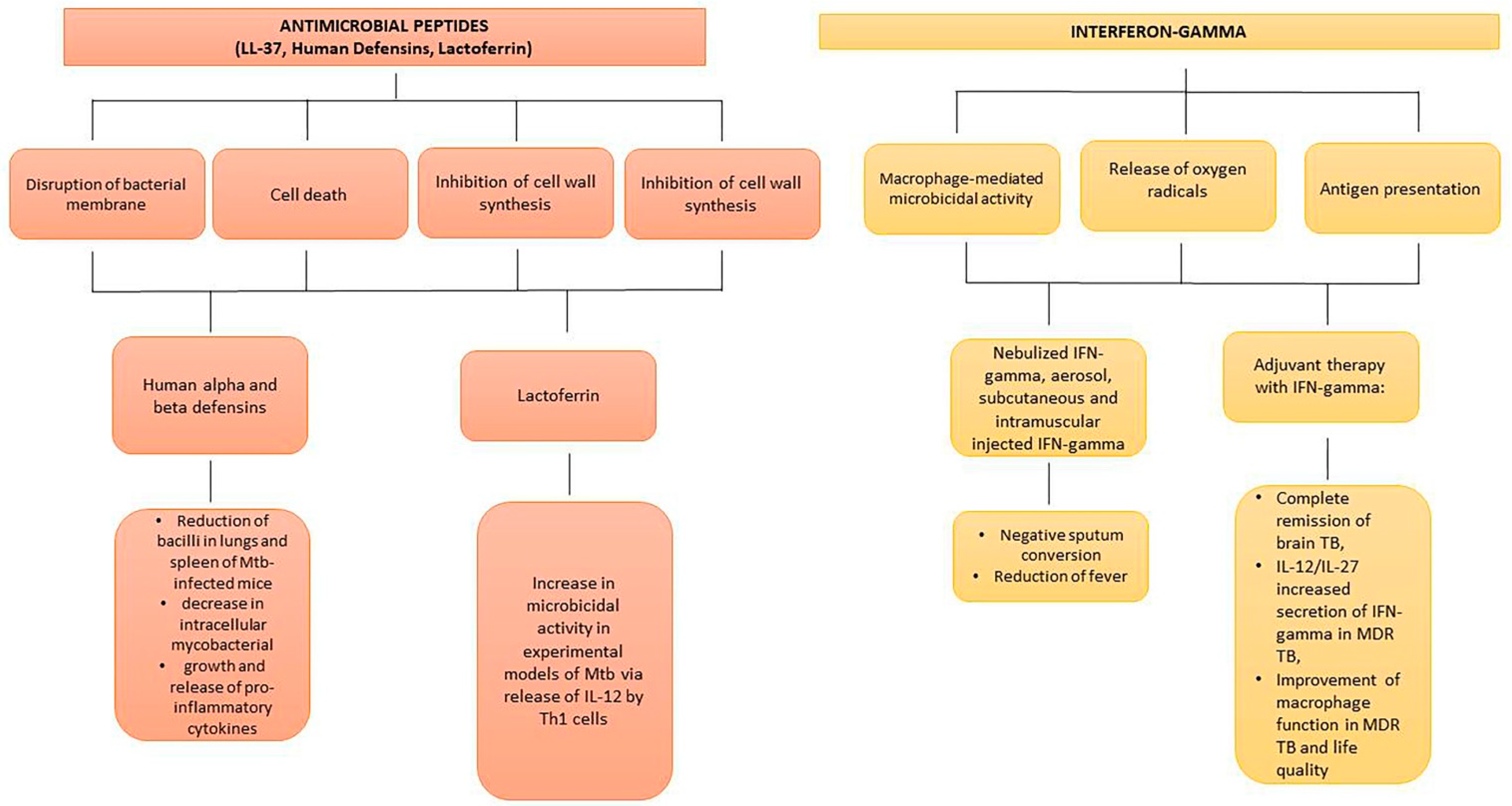
Figure 2. Biotherapeutics for treatment of experimental and human TB. AMPs target Mtb in different ways, inhibiting intracellular mycobacterial growth and reducing pro-inflammatory cytokines and IL-12 release by Th1 cells. Nebulized, aerosol, subcutaneous, and intramuscular IFN-gamma administration leads to sputum conversion, reduction of fever, and improvement of life quality in severe human TB.
4. Interferon-Gamma and Mesenchymal Stem Cells
IFN-gamma represents a protective cytokine against TB progression that is produced by Th1 and T cytotoxic lymphocytes a few days after infection [35][36][37]. Several genes that encode IFN-gamma and its receptors are required for anti-TB response to occur [38]. In particular, IFN-gamma potentiates the microbicidal response of macrophages, with the release of nitric oxide and reactive oxygen species, and the enhancement of antigen presentation [39]. In TB patients infected with a MDR Mtb strain, levels of IFN-gamma were reduced and the same was true in TB patients treated with beta-lactams [40][41]. In a meta-analysis, evidence has been provided that IFN-gamma represents an adjunctive therapy against lung TB [42]. In separate clinical trials, nebulized IFN-gamma, aerosol, subcutaneous injected IFN-gamma, and intramuscularly administered IFN-gamma were very effective in negative sputum conversion and reduction in fever symptoms [43][44]. Remarkably, intramuscular injection of IFN-gamma was very effective in patients with MDR TB [45]. Another three studies in patients with MDR TB demonstrated the efficacy of adjuvant therapy with IFN-gamma: i. A case of brain TB with complete remission following 12 months of treatment [46][47]; ii. Increase in IL-12/IL-27-induced secretion of IFN-gamma in MDR TB [43]; iii. Improvement of macrophage function in MDR TB patients [48]. Finally, adjunct therapy with IFN-gamma was very beneficial in patients with destructive lung TB, also significantly improving life quality [49]. Mesenchymal stem cells (MSCs) are pluripotent stem cells present in the bone marrow, skin, thymus, placenta, and umbilical cord tissue, that can be induced to differentiate into osteoblasts, adipocytes, chondroblasts, and neuron cells [50][51]. Over recent years, a few reports have attributed a role to MSCs in the regulation of tuberculosis granuloma (TG). These cells generate nitric oxide, which can inhibit the growth of Mtb within the granuloma [52]. Conversely, MSCs are niches for Mtb dormancy in the context of TG and may contribute to the development of Tuberculosis [53]. Notably, there is evidence that MSCs can affect lipid homeostasis in macrophages, also reducing the expression of MHC II [54]. These activities, in turn, may decrease the Mtb energy supply, regulating the lipid metabolism in macrophages. As reported by Zhang and associates [54][55], the application of MSCs for the treatment of tuberculosis is at the beginning stages and some issues should be taken into consideration, such as, tissue sources of MSCs, culture conditions in vitro, and possible side effects.
References
- Santacroce, L.; Man, A.; Charitos, I.A.; Haxhirexha, K.; Topi, S. Current knowledge about the connection between health status and gut microbiota from birth to elderly. A narrative review. Front. Biosci. (Landmark Ed.) 2021, 26, 135–148.
- Negatu, D.A.; Liu, J.J.J.; Zimmerman, M.; Kaya, F.; Dartois, V.; Aldrich, C.C.; Gengenbacher, M.; Dick, T. Whole-Cell Screen of Fragment Library Identifies Gut Microbiota Metabolite Indole Propionic Acid as Antitubercular. Antimicrob. Agents Chemother. 2018, 62, e01571-17.
- Genestet, C.; Bernard-Barret, F.; Hodille, E.; Ginevra, C.; Ader, F.; Goutelle, S.; Lina, G.; Dumitrescu, O.; Lyon, T.B.; Lyon TB study group. Antituberculous Drugs Modulate Bacterial Phagolysosome Avoidance and Autophagy in Mycobacterium tuberculosis-Infected Macrophages. Tuberculosis 2018, 111, 67–70.
- Liu, Y.; Tran, D.Q.; Rhoads, J.M. Probiotics in Disease Prevention and Treatment. J. Clin. Pharmacol. 2018, 58, S164–S179.
- Pamer, E.G. Resurrecting the intestinal microbiota to combat antibiotic-resistant pathogens. Science 2016, 352, 535–538.
- Hörmannsperger, G.; Haller, D. Molecular crosstalk of probiotic bacteria with the intestinal immune system: Clinical relevance in the context of inflammatory bowel disease. Int. J. Med. Microbiol. 2010, 300, 63–73.
- Ghadimi, D.; Fölster-Holst, R.; de Vrese, M.; Winkler, P.; Heller, K.J.; Schrezenmeir, J. Effects of Probiotic Bacteria and Their Genomic DNA on TH1/TH2-Cytokine Production by Peripheral Blood Mononuclear Cells (PBMCs) of Healthy and Allergic Subjects. Immunobiology 2008, 213, 677–692.
- Cardona, P.J. The Progress of Therapeutic Vaccination with Regard to Tuberculosis. Front. Microbiol. 2016, 7, 1536.
- Montané, E.; Barriocanal, A.M.; Arellano, A.L.; Valderrama, A.; Sanz, Y.; Perez-Alvarez, N.; Cardona, P.; Vilaplana, C.; Cardona, P.-J. Pilot, Double-Blind, Randomized, Placebo-Controlled Clinical Trial of the Supplement Food Nyaditum Resae® in Adults with or without Latent TB Infection: Safety and Immunogenicity. PLoS ONE 2017, 12, e0171294.
- Rahim, M.A.; Seo, H.; Kim, S.; Tajdozian, H.; Barman, I.; Lee, Y.; Lee, S.; Song, H.-Y. In Vitro Anti-Tuberculosis Effect of Probiotic Lacticaseibacillus rhamnosus PMC203 Isolated from Vaginal Microbiota. Sci. Rep. 2022, 12, 8290.
- Jiang, L.; Wang, J.; Xu, L.; Cai, J.; Zhao, S.; Ma, A. Lactobacillus Casei Modulates Inflammatory Cytokines and Metabolites during Tuberculosis Treatment: A Post Hoc Randomized Controlled Trial. Asia. Pac. J. Clin. Nutr. 2022, 31, 66–77.
- Lee, Y.; Seo, H.; Kim, S.; Rahim, M.D.A.; Yoon, Y.; Jung, J.; Lee, S.; Beom Ryu, C.; Song, H.-Y. Activity of Lactobacillus Crispatus Isolated from Vaginal Microbiota against Mycobacterium tuberculosis. J. Microbiol. 2021, 59, 1019–1030.
- Magrone, T.; Magrone, M.; Russo, M.A.; Jirillo, E. Recent Advances on the Anti-Inflammatory and Antioxidant Properties of Red Grape Polyphenols: In Vitro and In Vivo Studies. Antioxidants 2019, 9, 35.
- Watson, R.R. Polyphenols: Prevention and Treatment of Human Disease, 2nd ed.; Elsevier: San Diego, CA, USA, 2018.
- Cao, R.; Teskey, G.; Islamoglu, H.; Gutierrez, M.; Salaiz, O.; Munjal, S.; Fraix, M.P.; Sathananthan, A.; Nieman, D.C.; Venketaraman, V. Flavonoid Mixture Inhibits Mycobacterium tuberculosis Survival and Infectivity. Molecules 2019, 24, 851.
- Raju, A.; Degani, M.S.; Khambete, M.P.; Ray, M.K.; Rajan, M.G. Antifolate Activity of Plant Polyphenols against Mycobacterium tuberculosis. Phytother. Res. 2015, 29, 1646–1651.
- Salih, E.Y.A.; Julkunen-Tiitto, R.; Luukkanen, O.; Sipi, M.; Fahmi, M.K.M.; Fyhrquist, P.J. Potential Anti-Tuberculosis Activity of the Extracts and Their Active Components of Anogeissus leiocarpa (DC.) Guill. and Perr. with Special Emphasis on Polyphenols. Antibiotics 2020, 9, 364.
- Chakraborty, A.K.; Saha, S.; Poria, K.; Samanta, T.; Gautam, S.; Mukhopadhyay, J. A Saponin-Polybromophenol Antibiotic (CU1) from Cassia Fistula Bark Against Multi-Drug Resistant Bacteria Targeting RNA Polymerase. Curr. Res. Pharm. Drug Discov. 2022, 3, 100090.
- Shinozaki, S.; Chang, K.; Sakai, M.; Shimizu, N.; Yamada, M.; Tanaka, T.; Nakazawa, H.; Ichinose, F.; Yamada, Y.; Ishigami, A.; et al. Inflammatory Stimuli Induce Inhibitory S-Nitrosylation of the Deacetylase SIRT1 to Increase Acetylation and Activation of P53 and P65. Sci. Signal 2014, 7, ra106.
- Yang, H.; Chen, J.; Chen, Y.; Jiang, Y.; Ge, B.; Hong, L. Sirtuin Inhibits, M. Tuberculosis -Induced Apoptosis in Macrophage through Glycogen Synthase Kinase-3β. Arch. Biochem. Biophys. 2020, 694, 108612.
- Magana, M.; Pushpanathan, M.; Santos, A.L.; Leanse, L.; Fernandez, M.; Ioannidis, A.; Giulianotti, M.A.; Apidianakis, Y.; Bradfute, S.; Ferguson, A.L.; et al. The Value of Antimicrobial Peptides in the Age of Resistance. Lancet Infect. Dis. 2020, 20, e216–e230.
- Gaglione, R.; Pizzo, E.; Notomista, E.; de la Fuente-Nunez, C.; Arciello, A. Host Defence Cryptides from Human Apolipoproteins: Applications in Medicinal Chemistry. Curr. Top. Med. Chem. 2020, 20, 1324–1337.
- Mehta, K.; Sharma, P.; Mujawar, S.; Vyas, A. Role of Antimicrobial Peptides in Treatment and Prevention of Mycobacterium tuberculosis: A Review. Int. J. Pept. Res. Ther. 2022, 28, 132.
- Jadhav, K.; Singh, R.; Ray, E.; Singh, A.K.; Verma, R.K. Taming the devil: Antimicrobial peptides for safer TB therapeutics. Curr. Protein Pept. Sci. 2022.
- Travis, S.M.; Anderson, N.N.; Forsyth, W.R.; Espiritu, C.; Conway, B.D.; Greenberg, E.P.; McCray, P.B., Jr.; Lehrer, R.I.; Welsh, M.J.; Tack, B.F. Bactericidal activity of mammalian cathelicidin-derived peptides. Infect. Immun. 2000, 68, 2748–2755.
- Hancock, R.E.; Sahl, H.G. Antimicrobial and host-defense peptides as new anti-infective therapeutic strategies. Nat. Biotechnol. 2006, 24, 1551–1557.
- Kumar, P.; Kizhakkedathu, J.N.; Straus, S.K. Antimicrobial Peptides: Diversity, Mechanism of Action and Strategies to Improve the Activity and Biocompatibility In Vivo. Biomolecules 2018, 8, 4.
- Silva, T.; Gomes, M.S. Immuno-Stimulatory Peptides as a Potential Adjunct Therapy against Intra-Macrophagic Pathogens. Molecules 2017, 22, 1297.
- Dürr, U.H.; Sudheendra, U.S.; Ramamoorthy, A. LL-37, the only human member of the cathelicidin family of antimicrobial peptides. Biochim. Biophys. Acta 2006, 1758, 1408–1425.
- Yang, B.; Good, D.; Mosaiab, T.; Liu, W.; Ni, G.; Kaur, J.; Liu, X.; Jessop, C.; Yang, L.; Fadhil, R.; et al. Significance of LL-37 on Immunomodulation and Disease Outcome. Biomed Res. Int. 2020, 2020, 8349712.
- Liu, P.T.; Stenger, S.; Li, H.; Wenzel, L.; Tan, B.H.; Krutzik, S.R.; Ochoa, M.T.; Schauber, J.; Wu, K.; Meinken, C.; et al. Toll-like Receptor Triggering of a Vitamin D-Mediated Human Antimicrobial Response. Science 2006, 311, 1770–1773.
- Mily, A.; Rekha, R.S.; Kamal, S.M.M.; Arifuzzaman, A.S.M.; Rahim, Z.; Khan, L.; Haq, M.A.; Zaman, K.; Bergman, P.; Brighenti, S.; et al. Significant Effects of Oral Phenylbutyrate and Vitamin D3 Adjunctive Therapy in Pulmonary Tuberculosis: A Randomized Controlled Trial. PLoS ONE 2015, 10, e0138340.
- Torres-Juarez, F.; Cardenas-Vargas, A.; Montoya-Rosales, A.; González-Curiel, I.; Garcia-Hernandez, M.H.; Enciso-Moreno, J.A.; Hancock, R.E.W.; Rivas-Santiago, B. LL-37 Immunomodulatory Activity during Mycobacterium tuberculosis Infection in Macrophages. Infect. Immun. 2015, 83, 4495–4503.
- Cobongela, S.; Makatini, M.M.; Mdluli, P.S.; Sibuyi, N. Acyldepsipeptide Analogues: A Future Generation Antibiotics for Tuberculosis Treatment. Pharmaceutics 2022, 14, 1956.
- Desvignes, L.; Wolf, A.J.; Ernst, J.D. Dynamic Roles of Type I and Type II IFNs in Early Infection with Mycobacterium tuberculosis. J. Immunol. 2012, 188, 6205–6215.
- Petruccioli, E.; Scriba, T.J.; Petrone, L.; Hatherill, M.; Cirillo, D.M.; Joosten, S.A.; Ottenhoff, T.H.; Denkinger, C.M.; Goletti, D. Correlates of Tuberculosis Risk: Predictive Biomarkers for Progression to Active Tuberculosis. Eur. Respir. J. 2016, 48, 1751–1763.
- Berns, S.A.; Isakova, J.A.; Pekhtereva, P.I. Therapeutic Potential of Interferon-Gamma in Tuberculosis. Admet Dmpk 2022, 10, 63–73.
- Ernst, J.D. The Immunological Life Cycle of Tuberculosis. Nat. Rev. Immunol. 2012, 12, 581–591.
- Hickman-Davis, J.M.; Fang, F.C.; Nathan, C.; Shepherd, V.L.; Voelker, D.R.; Wright, J.R. Lung surfactant and reactive oxygen-nitrogen species: Antimicrobial activity and host-pathogen interactions. Am. J. Physiol. Lung Cell. Mol. Physiol. 2001, 281, L517–L523.
- Fortes, A.; Pereira, K.; Antas, P.R.Z.; Franken, C.L.M.C.; Dalcolmo, M.; Ribeiro-Carvalho, M.M.; Cunha, K.S.; Geluk, A.; Kritski, A.; Kolk, A.; et al. Detection of in Vitro Interferon-Gamma and Serum Tumour Necrosis Factor-Alpha in Multidrug-Resistant Tuberculosis Patients. Clin. Exp. Immunol. 2005, 141, 541–548.
- Brooks, B.M.; Hart, C.A.; Coleman, J.W. Differential Effects of Beta-Lactams on Human IFN-Gamma Activity. J. Antimicrob. Chemother. 2005, 56, 1122–1125.
- Gao, X.-F.; Yang, Z.-W.; Li, J. Adjunctive Therapy with Interferon-Gamma for the Treatment of Pulmonary Tuberculosis: A Systematic Review. Int. J. Infect. Dis. 2011, 15, 594–600.
- Condos, R.; Rom, W.N.; Schluger, N.W. Treatment of Multidrug-Resistant Pulmonary Tuberculosis with Interferon-Gamma via Aerosol. Lancet 1997, 349, 1513–1515.
- Park, S.-K.; Cho, S.; Lee, I.-H.; Jeon, D.-S.; Hong, S.-H.; Smego, R.A.; Cho, S.-N. Subcutaneously Administered Interferon-Gamma for the Treatment of Multidrug-Resistant Pulmonary Tuberculosis. Int. J. Infect. Dis. 2007, 11, 434–440.
- Suárez-Méndez, R.; García-García, I.; Fernández-Olivera, N.; Valdés-Quintana, M.; Milanés-Virelles, M.T.; Carbonell, D.; Machado-Molina, D.; Valenzuela-Silva, C.M.; López-Saura, P.A. Adjuvant interferon gamma in patients with drug-resistant pulmonary tuberculosis: A pilot study. BMC Infect. Dis. 2004, 4, 44.
- Raad, I.; Hachem, R.; Leeds, N.; Sawaya, R.; Salem, Z.; Atweh, S. Use of Adjunctive Treatment with Interferon-Gamma in an Immunocompromised Patient Who Had Refractory Multidrug-Resistant Tuberculosis of the Brain. Clin. Infect. Dis. 1996, 22, 572–574.
- Pisarenko, M.S. Peculiarities of IFN-g secretion in drug-resistant pulmonary tuberculosis. Fundam. Res. 2013, 9, 444–447.
- Khan, T.A.; Mazhar, H.; Saleha, S.; Tipu, H.N.; Muhammad, N.; Abbas, M.N. Interferon-Gamma Improves Macrophages Function against M. Tuberculosis in Multidrug-Resistant Tuberculosis Patients. Chemother. Res. Pr. 2016, 2016, 7295390.
- Ballini, A.; De Frenza, G.; Cantore, S.; Papa, F.; Grano, M.; Mastrangelo, F.; Tetè, S.; Grassi, F.R. In vitro stem cell cultures from human dental pulp and periodontal ligament: New prospects in dentistry. Int. J. Immunopathol. Pharmacol. 2007, 20, 9–16.
- Charitos, I.A.; Ballini, A.; Cantore, S.; Boccellino, M.; Di Domenico, M.; Borsani, E.; Nocini, R.; Di Cosola, M.; Santacroce, L.; Bottalico, L. Stem Cells: A Historical Review about Biological, Religious, and Ethical Issues. Stem. Cells Int. 2021, 2021, 9978837.
- Raghuvanshi, S.; Sharma, P.; Singh, S.; Van Kaer, L.; Das, G. Mycobacterium tuberculosis evades host immunity by recruiting mesenchymal stem cells. Proc. Natl. Acad. Sci. USA 2010, 107, 21653–21658.
- Das, B.; Kashino, S.S.; Pulu, I.; Kalita, D.; Swami, V.; Yeger, H.; Felsher, D.W.; Campos-Neto, A. CD271(+) bone marrow mesenchymal stem cells may provide a niche for dormant Mycobacterium tuberculosis. Sci. Transl. Med. 2013, 5, 170ra13.
- Zhang, X.; Huang, F.; Li, W.; Dang, J.L.; Yuan, J.; Wang, J.; Zeng, D.L.; Sun, C.X.; Liu, Y.Y.; Ao, Q.; et al. Human Gingiva-Derived Mesenchymal Stem Cells Modulate Monocytes/Macrophages and Alleviate Atherosclerosis. Front. Immunol. 2018, 9, 878.
- Zhang, X.; Xie, Q.; Ye, Z.; Li, Y.; Che, Z.; Huang, M.; Zeng, J. Mesenchymal Stem Cells and Tuberculosis: Clinical Challenges and Opportunities. Front. Immunol. 2021, 12, 695278.
- Maslennikov, A.A.; Obolonkova, N.I.; Belgorod State National Research University. Efficiency of ingaron in the treatment of patients with destructive pulmonary bacteriologicaly proven tuberculosis. Res. Result 2016, 2, 10–16.
More
Information
Subjects:
Infectious Diseases
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
967
Revisions:
2 times
(View History)
Update Date:
01 Nov 2022
Table of Contents




Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No