 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Beatrix Zheng | -- | 4979 | 2022-10-14 01:38:26 |
Video Upload Options
The respirable fraction of lunar dusts may be toxic to humans. NASA has therefore determined that an exposure standard is necessary to limit the amount of respirable airborne lunar dusts to which astronauts will be exposed. The nominal toxicity that is expected from ordinary mineral dust may be increased for lunar dusts due to the large and chemically reactive surfaces of the dust grains. Human exposures to mineral dusts during industrial operations and from volcanic eruptions give researchers some sense of the relative toxicity of lunar dust, although the Earth-based analogs have serious limitations. Animal and cellular studies provide further evidence that mineral dusts can be somewhat toxic. Earth-based research of mineral dust has shown that freshly fractured surfaces are chemically reactive and can elicit an increased toxic response. Since lunar dust is formed in space vacuum from highly energetic processes, the grain surfaces can be expected to be indefinitely reactive on the lunar surface. NASA predicts that this chemical reactivity will change once the dust is brought into a habitable environment. Dust from lunar soil that was carried into spacecraft during the Apollo missions proved to be a nuisance. The lack of gravity, or the existence of microgravity, increases the time during which dust remains airborne, thereby increasing the probability that these dust particles will be inhaled. Lunar dust particles that are generated by impaction in a deep vacuum have complex shapes and highly reactive surfaces that are coated with a thin layer of vapor-deposited mineral phase. Airborne mineral dust in a variety of forms has been shown to present a serious health hazard to ground-based workers. Crew members who will be at a lunar outpost can be directly exposed to lunar dust in several ways. After crew members perform spacewalks or EVAs, they will introduce into the habitat a large quantity of dust that will have collected on spacesuits and boots. Cleaning of the suits between EVAs and changing of the Environmental Control Life Support System (ECLSS) filters are other operations that could result in direct exposure to lunar dusts. In addition, if the final spacesuit design is based on the current spacesuit design, EVAs may cause dermal injuries, and the introduction of lunar dusts into the suits' interior, which may enhance skin abrasions. When the crew leaves the lunar surface and returns to microgravity, the dust that is introduced into the crew return vehicle will "float," thus increasing the opportunity for ocular and respiratory injury.
1. Introduction
In 2004, George W. Bush unveiled a plan directing NASA to return humans to the Moon by the year 2015, and to use the lunar outpost as a stepping-stone for future human trips to Mars and beyond.[1] To meet this objective, NASA will build an outpost on the lunar surface near the south pole for long-duration human habitation and research. Because of the various activities that will require the astronauts to go in and out of this habitat on numerous spacewalks (EVAs), the living quarters at the lunar outpost are expected to be contaminated by lunar dust.
The president's Vision for Space Exploration and charge to return to the Moon resulted in questions about health hazards from exposure to lunar dust. Lunar dust resides in near-vacuum conditions, so the grain surfaces are covered in "unsatisfied" chemical bonds, thus making them very reactive.[2] When the reactive dust is inhaled, it can be expected to react with pulmonary surfactant and cells. The fine, respirable lunar dust could thus be toxic if the astronauts are exposed to it during mission operations at a lunar base. Although a few early attempts were made to understand the toxicity of the lunar dust that was obtained by the Apollo astronauts or the Luna probes, no scientifically defensible toxicological studies have been performed on authentic lunar dust.
Awareness of the toxicity of terrestrial dusts has increased greatly since the original Apollo flights, which occurred circa 1970, in which the crew members were exposed to lunar dust for a relatively brief time. The first National Ambient Air Quality Standard (NAAQS) was issued by the Environmental Protection Agency (EPA) in 1971 and was indexed to total suspended particles (TSP) on a mass per unit volume basis. In 1987, this NAAQS was refined to include only particles that were of less than 10 μm in aerodynamic diameter (PM10) because this was the size that was most likely to reach the bronchial tree and deeper into the lung. Finally, in 1997, the EPA Administrator issued standards for particles that were less than 2.5 μm in aerodynamic diameter (PM2.5) based primarily on epidemiological associations of increased mortality, exacerbation of asthma, and increased hospital admissions for cardiopulmonary symptoms. None of these standards specified the composition of the particles. In fact, the last standard was a bit contentious because mechanisms of toxic action were not understood.[3]
In a review article, Schlesinger et al. list the properties of particulate matter that might elicit adverse effects.[4] The properties that seem pertinent to lunar dust include: size distribution, mass concentration, particle surface area, number concentration, acidity, particle surface chemistry, particle reactivity, metal content, water solubility, and geometric form. In attempting to consider each of these properties, one property emerges as the most difficult to study; particle surface chemistry may be difficult to understand because the environment on the lunar surface is unlike any on Earth, and is likely to alter the surface of dust grains in a way that will render them highly reactive. Recreating the processes that could affect grain surface reactivity on the moon is difficult in an Earth-bound laboratory. Freshly fractured quartz is distinctly more toxic to the rat respiratory system than aged quartz.[5] Quartz and lunar dust may have similar toxic properties, but breaking of surface bonds on mineral substrates has been shown to increase the toxicity of the well-studied mineral quartz.
The site at which various sizes of particles are deposited is critical to an understanding of any aspect of their toxic action. The fractional regional deposition of particles shows that between 10 and 1 μm, the portion of particles that is deposited in the upper airways falls off from 80% to 20%, whereas the pulmonary deposition increases from near zero to about 20%. Pulmonary deposition, after falling off near 1 μm, peaks again near 40% for particles of 0.03 μm, whereas upper airway deposition remains low until a new peak deposition is found at less than 0.01 μm. The portion and pattern of deposition can be modified under conditions of reduced gravity; however, human data during flights of the gravity research aircraft show that particles in the 0.5 to 1 μm range are deposited less in the respiratory system at lunar gravity than at Earth gravity. This finding is consistent with the reduced sedimentation of the particles when the gravity is less. However, a larger portion of the particles is deposited peripherally in reduced gravity.[6]
The first encounter in which a particle deposits in the distal airways occurs with the broncho-alveolar lining fluid (BALF). The thickness of this fluid in the lung varies as the alveolar sacs expand and contract, but lies in the range of 0.1 to 0.9 μm.[7] In the case of biological particles such as bacteria, this fluid opsonizes the particles to facilitate ingestion by macrophages. A similar process has been demonstrated for nonbiological carbonaceous particles.[8] This process removes some components of the BALF that participate in opsonization, and it is postulated that this might enhance the toxicity of particles with a surface chemistry that is capable of selectively removing opsonizing components. The agglomeration of the grains is also affected by the interactions between the BALF and the grains. Preliminary data on authentic lunar dust has shown that in aqueous suspension, lunar particles agglomerate rapidly. Artificial surfactant has been found to greatly reduce this particulate agglomeration.
Particles that are deposited in the pulmonary region are eliminated according to their surface area and chemical composition. If a particle is relatively soluble, its dissolution products end up in the bloodstream. Relatively insoluble particles are ingested by macrophages and removed by mucociliary clearance or the lymphatic system, or they persist in the interstitial areas of the lung. Ultrafine particles (<0.1 μm) that deposit in the upper airways have been shown, under some conditions, to translocate to the brain,[9] whereas similar particles reaching the pulmonary regions can translocate to adjacent organs such as the liver.[10]
The effects of particles on the respiratory system include de novo causation of clinical disease as well as exacerbation of existing disease. If particulate inhalation is to directly cause disease, the exposure levels typically must be at levels that are encountered in industrial settings. For example, silicosis is a well-known disease of persons working for years in conditions in which dust containing quartz is inhaled. Epidemiological studies show that ambient dust levels such as those that are encountered in some cities can exacerbate respiratory conditions such as asthma and chronic obstructive pulmonary disease. At certain times, sand dust that originates in Asia or Arizona, for example, has been associated with exacerbation of allergenic respiratory inflammation.[11]
Of particular concern in addition to the respiratory system is the ability of small particles to affect the cardiovascular system. Epidemiological studies suggest that exposure to ambient particulate matter increases the incidence of angina, arrhythmia, and myocardial infarctions. The increased acute mortality that is associated with particle "events" is attributed to cardiovascular disease.[12] Clinical studies involving concentrated ambient air particulate have shown increased blood fibrinogen and reduced heart-rate variability;[13] exposure to ultrafine particles causes "blunted" repolarization response following exercise.[14] The role of C-reactive protein in mediating the effect of ambient particle exposures on the causation of CAD has been reviewed.[15] Batalha [16] has drawn attention to the ability of particles to elicit vasoconstriction of small pulmonary arteries. Although the mechanistic details have not been fully elucidated, the evidence favors a strong link between exposure to particulates and to both acute and chronic heart disease.[12] There is some evidence from the Apollo missions that, in susceptible individuals, lunar dust exposure may lead to cardiovascular effects that are similar to those produced through exposure to air pollution.[17]
The fact that no accepted health standards or policies exist concerning exposure limits to lunar dust is a critical challenge to the design of vehicle systems in the CxP. The multi-center Lunar Airborne Dust Toxicology Assessment Group (LADTAG) was formed and responded to a request from the Office of the Chief Health and Medical Officer to "… develop recommendations for defining risk criteria for human lunar dust exposure and a plan for the subsequent development of a lunar dust permissible exposure limit." The LADTAG is composed of technical experts in lunar geology, inhalation toxicology, biomedicine, cellular chemistry, and biology from within the agency as well as of leading U.S. experts in these fields. Based on the opinions that were expressed by the LADTAG experts, NASA scientists will develop and execute a plan to build a database on which a defensible exposure standard can be set.[18]
LADTAG experts recommend that the toxicity of lunar dust on the lungs (pulmonary toxicity), eyes (ocular toxicity), and skin (dermal toxicity) be investigated, and that this investigation is to be conducted by the Lunar Dust Toxicity Research Project (LDTRP) using various assays including in vivo and in vitro methods. In an initial LADTAG workshop that was held in 2005, experts noted that they were unable to reconcile individual expert opinions to set an inhalation standard. The array of opinions from these experts spanned a 300-fold range (i.e., 0.01 to 3 mg/m3). The members of the LADTAG concluded that research is necessary to narrow this wide uncertainty range, the lower end of which cannot be met by known methods of environmental control, and that there is an urgency to determine the standard so that environmental systems for the lunar vehicle can be appropriately designed. Therefore, in keeping with the LADTAG experts' recommendations, members of the LDTRP have reviewed first-hand accounts of Apollo astronauts who were exposed to lunar dust during their missions as well as of terrestrial-based human exposures to dust generated in the mining industry and to volcanic ash. In accordance with the LADTAG recommendations to increase our evidence base, the LDTRP is conducting studies of Apollo spacesuits, filters, vacuum bags, and rock-collection boxes. These studies will enable us to focus our understanding of the grain-size distribution that is present in the lunar surface samples and in the habitat, but the dust surfaces are expected to be fully passivated.
2. Ground-based Evidence
Ground-based evidence includes data that are derived from people who are exposed occupationally to mineral dusts in industrial settings, from people who live in close proximity to active volcanoes and have been exposed to volcanic ash, and from animals and cells that are in controlled experimental studies. Mechanistic insights also guide our thinking concerning the potential toxicity of lunar dusts.
2.1. Human Exposures During Industrial Operations
Workers in the mining industry are often exposed to dust from freshly fractured mineral deposits. When these workers use inadequate, or lack, respiratory protection completely, the consequences are devastating. A prime example of this is the Hawks Nest mining activity in West Virginia beginning in 1927. During the boring of a tunnel, deposits of silica were identified and mined; however, the workers did not use respiratory protection during the operations. Estimates of the proportion of workers who died, often within a few years, are typically about 30% of the 2,000 exposed workers.[19] This rapidly lethal form of silicosis has been called "acute silicosis," which is characterized by alveolar proteinosis and interstitial inflammation.[20] The respiratory effects are not exactly like those one would expect from simple silicosis, a disease that usually requires decades to develop after prolonged exposure to lower concentrations of silica dust. The latter disease is characterized by silicotic nodules that are clearly distinct from surrounding tissue and often surrounded by an inflammatory response.[20]
2.2. Humans and Laboratory Animals Exposed to Volcanic Ash
Volcanic ash originates from processes resulting in explosive eruptions into the atmosphere or pyroclastic flows oozing from the surface and discharging ash as they cool, or some combination thereof. Under any plausible condition, the ash will have had hours to days to react with the oxygen and water vapor of the atmosphere to passivate all surfaces before being inhaled by humans. The mineral composition of ash is determined by the composition of the magma. The particle size, mineral composition, and form of the minerals vary considerably from volcano to volcano as well as from one eruption to another eruption of the same volcano.
Shortly after Mount St. Helens erupted in 1980, a number of experts began to investigate the effects of volcanic ash on those who had been exposed to the dust.[21] The crystalline silica content of this dust ranged from 3% to 7%. The primary acute effects were reflected in increased emergency room visits for asthma, bronchitis, and eye discomfort.[22] The ash was noted to exacerbate chronic respiratory conditions. The increase in hospital admissions lasted approximately 3 weeks,[23] and immune parameters were affected even 1 year later.[24] The British West Indian Montserrat volcano began erupting in 1995, causing an ash fall from pyroclastic flows that contained 10% to 24% crystalline silica.[25] Recorded incidences of childhood wheezing increased as a result of relatively intense exposures to the ash.[26] To our knowledge, sustained long-term health effects have not been reported in association with exposures to volcanic ash, although there is speculation that the high cristobalite content of the Montserrat ash could lead to silicosis many years later.
Animal studies that focused on the biological effects of chronic inhalation exposure to Mount St. Helens volcanic ash or quartz, under controlled laboratory conditions, indicate significant dose-response to both materials.[27] The quartz that came from the volcano was found to be markedly toxic and fibrogenic; by contrast, the volcanic ash was much less toxic.[28][29] Similar results were noted in other animal studies,[30][31][32] suggesting that quartz is a much more potent pulmonary toxicant than volcanic ash.[29][31][32] However, the presence of volcanic ash in the inhaled air did increase the "histamine sensitivity" of the epithelial irritant receptors [30] as well as inhibit the ability of alveolar macrophages to protect against infection.[5]
The toxicity of volcanic ashes has been evaluated in rats that were dosed once by intratracheal instillation.[33] Ashes that were obtained from the San Francisco volcano field in Arizona (lunar dust simulant) and from a Hawaiian volcano (martian dust simulant) were compared to the toxicity of titanium dioxide and quartz. Lungs of mice that have been harvested 90 days after receiving a dose of 1 mg of lunar simulant showed chronic inflammation, septal thickening, and some fibrosis. No changes were seen at the low dose of 0.1 mg/mouse.[33] The martian dust simulant elicited a response that was similar to that of the lunar simulant, except that there was an inflammatory and fibrotic response even at a dose of 0.1 mg/mouse. The response of the mouse lungs to 0.1-mg quartz was comparable to the response to the martian dust simulant. In another study, the effect of these same simulants was assessed on human alveolar macrophages.[34] The lunar dust simulant was comparable in cell viability reduction and apoptosis induction to the TiO2 (titanium dioxide) negative control. Both were less toxic than the quartz positive control. Both simulants showed a dose-dependent increase in cytotoxicity.
2.3. Surface Activation and Trace Impurities Increase Toxicity
Inhalation of freshly ground quartz, when compared to inhalation of aged quartz, results in a significant increase in animal lung injury.[33][35] Freshly ground quartz has increased reactive silicon-based oxygen radicals, and animals that are exposed to freshly ground quartz have been found to have decreased concentrations of antioxidant enzymes.[5][36] Activated quartz particles decay with age in ambient air.[36] Quartz dusts containing surface iron as an impurity have been shown to deplete cellular glutathione, contributing to the oxidative damage that is caused by particle and cell-derived ROS.[37] Castranova et al.[38] suggest that freshly ground quartz dust that is contaminated with trace levels of iron may be more pathogenic than quartz dust alone.
Crystalline silica exposure studies indicate that the generation of oxidants and nitric oxide, which play an important role in the initiation of silicosis,[39] has been shown to cause pulmonary inflammation in rats.[40] Other studies indicate that the mode of action of crystalline silica cytotoxicity and pathogenicity lies in the ability of the mineral to induce lipid peroxidation.[41] Respiratory exposure to freshly ground silica causes greater generation of ROS from macrophages than exposure to aged silica, which is one piece of evidence that proves that freshly fractured silica is more toxic than aged silica.[40][42]
Further evidence linking increased toxicity to surface activation must await data that show that lunar dust that is activated by methods other than grinding adversely affects cells. NASA has been able to demonstrate that dust that is activated by processes that are analogous to those that are understood to be present at the lunar surface (i.e., ultraviolet [UV] irradiation in a vacuum) are able to produce more ROS in aqueous solution than dust that is not activated by these processes (Wallace, unpublished data). In addition, mineral coupons that are activated by proton and alpha-particle bombardment that is analogous to the solar wind show increased ROS (Kuhlman, unpublished data). NASA was expected to assess the impact of these activation techniques on cellular systems by early 2009.
2.4. Mechanistic Understandings
Lunar geologists state (Category I22 evidence) that iron is present in lunar dust, especially in the fraction of its smallest particles (nano-Fe), and that it can be postulated that a reaction involving iron could be important for activated lunar dust when it comes in contact with the mucous lining of the respiratory system. A good model of the issues and problems that are associated with testing surface-activated dust can be found in the studies of freshly fractured silica, which is highly toxic to the respiratory system via oxidative damage, and perhaps also in the testing of volcanic ash. The problem of the enhancement of toxicity in quartz by freshly fractured surfaces has been extensively investigated in animal and cellular systems.[40][43][44][45] Fracturing silica cleaves the Si-O bonds, leaving Si and SiO radicals, which, in turn, produce OH radicals in an aqueous environment. Aged crystalline silica still produces radicals, but at a much lower level, perhaps by the Fenton reaction that occurs between iron and H2O2 that is generated by macrophage phagocytosis of the particles.[43]
2.5. Passivation of Reactive Surfaces as Dust Surfaces Age
Since surface activation, which is produced primarily by grinding, is known to increase the toxicity of various mineral dusts, it is critical to ask how quickly surface activation disappears once the dust encounters an oxygen- and water-vapor-rich environment. Vallyathan et al.[42] demonstrated a bimodal decay by measuring the rate of disappearance of hydroxyl radical formation in an aqueous medium from silicon-based radicals on the surface of ground silica, when that ground silica was kept in air until the time of assay. The half-life of the fast decay was approximately 30 hours, whereas even after 4 weeks approximately 20% of the original activity that was induced by grinding was present on the surface of the quartz. This is similar to the ability of the 24-hour half-life in air of freshly fractured quartz to produce OH radicals.[43] Although quartz is not lunar dust and grinding is merely a surrogate for activation of dust at the lunar surface, the longevity of the surface reactivity requires careful attention to better understand how surface-activated lunar dust becomes passivated in a habitable environment.
3. Space Flight Evidence
Samples of lunar dust that have been returned to Earth have enabled NASA to learn the mineralogical properties of the dust at several lunar landing sites. First and foremost, one must keep in mind that the properties of the lunar dust may vary considerably depending on location; hence, lunar dusts may show a range of toxicity. Initially, NASA assessed the expected nature of dust at the proposed South Pole landing site on the rim of Shackleton crater.
All space flight evidence pertaining to the effect of lunar dust on astronauts is anecdotal (Category III). The post-flight debriefing reports of the Apollo astronauts serve as a base of evidence.[46] Although the astronauts attempted to remove the lunar dust before they reentered the command module (CM) by brushing the spacesuits or vacuuming, a significant amount of dust was returned to the spacecraft, which caused various problems. For instance, astronaut Harrison Schmitt complained of "hay fever" effects caused by the dust,[46] and the abrasive nature of the material was found to cause problems with various joints and seals of the spacecraft and spacesuits.[47] In these reports, the Apollo crews provided several accounts of problems with lunar dust exposure as follows:
- During Apollo 11, crew members reported: "Particles covered everything and a stain remained even after our best attempts to brush it off"; a "[d]istinct pungent odor like gunpowder [was] noted when helmet [was] removed"; and "[t]exture like graphite".[46]
- During Apollo 12, regarding dust in the lunar module (LM), the crew members noted several issues: "Both LM and CM contaminated with lunar dust"; "[LM] was filthy dirty and had so much dust that when I took my helmet off, I was almost blinded. Junk immediately got into my eyes"; and "[t]he whole thing was just a cloud of fine dust floating around in there." After the LM docked to the CM, dust infiltrated the CM. Crew members gave the following account of this period of contamination: "On the way back in the CM the system could not handle the dust, so it was continuously spread inside the spacecraft by the system"; "[w]e chose to remain in the suit loop as much as possible because of the dust and debris floating around"; and "[t]o keep our eyes from burning and our noses from inhaling these small particles, we left our helmet sitting on top of our heads".[46]
- By contrast, the Apollo 14 crew members stated: "Dust was not a problem for us in the cabin"; and "[t]he dust control procedures were effective".[46]
- The Apollo 15 crew members stated: "Cabin smelled like gunpowder when we first came into LM from EVA"; "[p]article matter floated around in spacecraft"; "[l]unar dust is 'soluble' in water"; and "[t]he vacuum cleaner did a good job of clearing the dust from the LM".[46]
- Apollo 16 crew members provided the following accounts: "The LM was extremely clean until the first EVA and then it was extremely dirty"; "I question whether the vacuum cleaner ever worked properly"; and "I thought it was quite a hazard over there floating through the LM with all the dust and debris. A number of times I got my eyes full of dust and particles. I felt like my right eye was scratched slightly once".[46]
- The Apollo 17 crew members recalled: "You knew [that] you were in a very heavily infiltrated atmosphere in the LM because of the lunar dust"; "[t]he dust clearing was remarkable considering the amount of dust we had"; "[a]lthough there was a lot of irritation to my sinuses and nostrils soon after taking the helmet off, by 2 hours that had decreased considerably"; "I did all the transfer with my helmet off and I am sorry I did because the dust really bothered my eyes and throat. I was tasting it and eating it"; and "[w]hen I climbed in the tunnel I could tell there was a lot of dust in the LM and you could smell it".[46]
NASA crew surgeon (Category IV), Dr. Bill Carpentier,[48] observed his own, as well as Apollo mission crew members', post-flight allergic-type responses. Dr. Carpentier recalls an increase in eosinophil and basophil blood cell counts after the crew members were exposed to lunar dust, which may have indicated an allergic response.
Although no substantive evidence exists that astronaut performance was impaired by lunar dust,[47] one can imagine that if a crew member were "almost blinded" and had to "remain in the suit loop as much as possible because of the dust and debris floating around," the dust did have some impact on performance.
Dust from the lunar soil that was carried into the spacecraft during the Apollo missions proved to be a significant, intermittent problem. With the return to the moon and planned long-duration stays on the lunar surface, the dust toxicity and contamination problems are potentially much more serious than those that were experienced during the Apollo missions. Physical evidence also suggests that lunar dust could be a health hazard at a lunar outpost. Gravity at one-sixth that of the gravitational force of the Earth increases the time in which dust remains airborne, thereby increasing the probability that these dust particles will be inhaled.
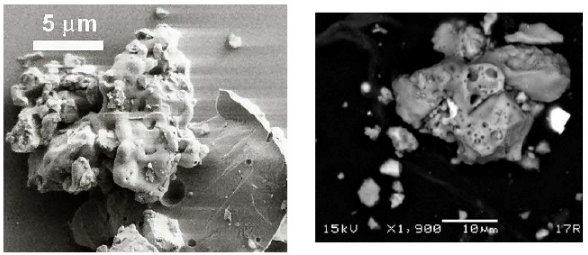
Some examples of lunar dust grains are provided in figure 13-1.
4. Exploration Mission Operational Scenarios
Multiple, probable scenarios exist in which crew members could be exposed to lunar dust during both lunar sortie and lunar outpost missions. Further, there are opportunities for crew members to be directly exposed to lunar dust after they perform EVAs. Post EVA, lunar crew members will introduce into the habitat and lunar lander the dust that has collected on their spacesuits and boots. Cleaning of the suits between EVAs may also directly expose crew members to lunar dust. For crew members, changing of Environmental Control and Life Support System filters is yet another potential route of direct exposure to lunar dusts. These episodic periods of increased lunar dust exposure must be taken into account when long-term exposure limits are calculated. As missions become longer, the greater dose and/or duration of lunar dust exposure will increase the potential human health risk. When a crew returns to microgravity, if lunar dust is introduced into the crew return vehicle, there will be an increased opportunity for ocular exposure if particles of dust are floating throughout the cabin. EVAs cause dermal injuries when suits that are based on the current design are used, and the introduction of lunar dusts may enhance injuries that will be sustained from contact with the EVA suit. In addition, NASA is considering the use of a rover design that will allow shirtsleeve operation of the vehicle. Thus, the rover, which must be kept in an interior space to be entered without a spacesuit, may also bring dust into the habitat.
5. Conclusion
The evidence base shows that prolonged exposure to respirable lunar dust could be detrimental to human health. Lunar dust is known to have a large surface area (i.e., it is porous), and a substantial portion is in the respirable range. The surface of the lunar dust particles is known to be chemically activated by processes ongoing at the surface of the moon. Predictions are that this reactivity will disappear on entry into the habitable volume; however, it is not known how quickly the passivation of chemical reactivity will occur, nor is it known how toxic the deactivated dust may prove to be. Although many Apollo astronauts seemed to tolerate lunar dust, their exposure times were brief and time (duration) exposure factors need to be determined. Other Apollo crew members and ground support personnel noted that the lunar dust was a sensory irritant. Finally, the size characteristics of the dust that actually was present in the atmosphere of the lunar lander have never been determined. Obtaining data will help NASA understand the size distribution of the particles that are expected to be found in future lunar habitats. It is important to design experiments that will close or, at a minimum, narrow knowledge gaps so that a scientifically defensible exposure standard can be set by NASA for protection of crew health.
References
- "Bush outlines plan for 2015 moon landing". chinadaily.com.cn. http://www.chinadaily.com.cn/en/doc/2004-01/15/content_299037.htm. Retrieved 17 August 2013.
- Taylor, L; James, J (2006). "Potential toxicity of lunar dust". Lunar and Planetary Institute. http://www.lpi.usra.edu/meetings/roundtable2006/pdf/1008.pdf.
- ((National Research Council, Committee on Research Priorities for Airborne Particulate Matter, Board on Environmental Studies and Toxicology, Commission on Life Sciences, Commission on Geosciences, Environment, and Resources)) (1998). Research priorities for airborne particulate matter ([Online-Ausg.]. ed.). Washington, D.C.: National Academy Press. ISBN 978-0-309-06094-3.
- Schlesinger, RB; Kunzli, N; Hidy, GM; Gotschi, T; Jerrett, M (February 2006). "The health relevance of ambient particulate matter characteristics: coherence of toxicological and epidemiological inferences.". Inhalation Toxicology 18 (2): 95–125. doi:10.1080/08958370500306016. PMID 16393926. https://dx.doi.org/10.1080%2F08958370500306016
- Vallyathan, V; Castranova, V; Pack, D; Leonard, S; Shumaker, J; Hubbs, AF; Shoemaker, DA; Ramsey, DM et al. (September 1995). "Freshly fractured quartz inhalation leads to enhanced lung injury and inflammation. Potential role of free radicals.". American Journal of Respiratory and Critical Care Medicine 152 (3): 1003–9. doi:10.1164/ajrccm.152.3.7663775. PMID 7663775. https://dx.doi.org/10.1164%2Fajrccm.152.3.7663775
- Darquenne, C; Prisk, GK (August 2008). "Deposition of inhaled particles in the human lung is more peripheral in lunar than in normal gravity.". European Journal of Applied Physiology 103 (6): 687–95. doi:10.1007/s00421-008-0766-y. PMID 18488244. https://dx.doi.org/10.1007%2Fs00421-008-0766-y
- Bastacky, J; Lee, CY; Goerke, J; Koushafar, H; Yager, D; Kenaga, L; Speed, TP; Chen, Y et al. (November 1995). "Alveolar lining layer is thin and continuous: low-temperature scanning electron microscopy of rat lung". Journal of Applied Physiology 79 (5): 1615–28. doi:10.1152/jappl.1995.79.5.1615. PMID 8594022. https://dx.doi.org/10.1152%2Fjappl.1995.79.5.1615
- Kendall, Michaela; Brown, Leslie; Trought, Katherine (1 January 2004). "Molecular Adsorption at Particle Surfaces: A PM Toxicity Mediation Mechanism". Inhalation Toxicology 16 (s1): 99–105. doi:10.1080/08958370490443187. PMID 15204798. https://dx.doi.org/10.1080%2F08958370490443187
- Oberdörster, G; Sharp, Z; Atudorei, V; Elder, A; Gelein, R; Kreyling, W; Cox, C (June 2004). "Translocation of inhaled ultrafine particles to the brain". Inhalation Toxicology 16 (6–7): 437–45. doi:10.1080/08958370490439597. PMID 15204759. https://dx.doi.org/10.1080%2F08958370490439597
- Oberdörster, G; Sharp, Z; Atudorei, V; Elder, A; Gelein, R; Lunts, A; Kreyling, W; Cox, C (25 October 2002). "Extrapulmonary translocation of ultrafine carbon particles following whole-body inhalation exposure of rats.". Journal of Toxicology and Environmental Health. Part A 65 (20): 1531–43. doi:10.1080/00984100290071658. PMID 12396867. https://dx.doi.org/10.1080%2F00984100290071658
- Ichinose, T; Yoshida, S; Sadakane, K; Takano, H; Yanagisawa, R; Inoue, K; Nishikawa, M; Mori, I et al. (May 2008). "Effects of asian sand dust, Arizona sand dust, amorphous silica and aluminum oxide on allergic inflammation in the murine lung.". Inhalation Toxicology 20 (7): 685–94. doi:10.1080/08958370801935133. PMID 18464056. https://dx.doi.org/10.1080%2F08958370801935133
- ((National Research Council of the National Academies, Committee on Research Priorities for Airborne Particulate Matter, Board on Environmental Studies and Toxicology, Division on Earth and Life Studies)) (2004). Research Priorities for Airborne Particulate Matter, Vol IV. Washington, D.C.: National Academies Press. ISBN 978-0-309-09199-2.
- Devlin, RB; Ghio, AJ; Kehrl, H; Sanders, G; Cascio, W (May 2003). "Elderly humans exposed to concentrated air pollution particles have decreased heart rate variability.". European Respiratory Journal. Supplement 40: 76s–80s. doi:10.1183/09031936.03.00402403. PMID 12762579. https://dx.doi.org/10.1183%2F09031936.03.00402403
- Frampton, MW; Zareba, W; Daigle, CC; Oberdorster, G; Utell, MJ (2002). "Inhalation of ultrafine particles alters myocardial repolarization in humans [abstr"]. American Journal of Respiratory and Critical Care Medicine 165: B16. http://cfpub.epa.gov/si/si_public_record_Report.cfm?dirEntryID=79291.
- Sandhu, RS; Petroni, DH; George, WJ (June–July 2005). "Ambient particulate matter, C-reactive protein, and coronary artery disease". Inhalation Toxicology 17 (7–8): 409–13. doi:10.1080/08958370590929538. PMID 16020037. https://dx.doi.org/10.1080%2F08958370590929538
- Batalha, JRF (2002). "Concentrated ambient air particles induce vasoconstriction of small pulmonary arteries in rats". Environmental Health Perspectives 110 (10): 1191–1197. doi:10.1289/ehp.5484. PMID 12460797. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1241105
- Rowe, W (2000). "Moon dust may simulate vascular hazards of urban pollution". Journal of the British Interplanetary Society 60: 133–136. Bibcode: 2007JBIS...60..133R. http://adsabs.harvard.edu/abs/2007JBIS...60..133R
- Khan-Mayberry, NN (2008). "The lunar environment : determining the health effects of exposure to moon dusts". Acta Astronautica 63 (7–10): 99–105. doi:10.1016/j.actaastro.2008.03.015. Bibcode: 2008AcAau..63.1006K. https://ntrs.nasa.gov/archive/nasa/casi.ntrs.nasa.gov/20070006527_2007005296.pdf.
- Cherniack, M (1986). The Hawk's Nest incident: America's worst industrial disaster. New Haven, Conn.: Yale University Press. ISBN 978-0300044850. https://archive.org/details/hawksnestinciden0000cher.
- Driscol, K; Guthrie, G (1997). "Crystaline silica and silicosis". in Sipes, I. Toxicology of the respiratory system. (1st ed.). NY: Elsevier Science, Inc.. ISBN 978-0080429731.
- Bernstein, RS; Baxter, PJ; Falk, H; Ing, R; Foster, L; Frost, F (March 1986). "Immediate public health concerns and actions in volcanic eruptions: lessons from the Mount St. Helens eruptions, May 18-October 18, 1980". American Journal of Public Health 76 (3 Suppl): 25–37. doi:10.2105/ajph.76.suppl.25. PMID 3946727. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1651693
- Baxter, PJ; Ing, R; Falk, H; French, J; Stein, GF; Bernstein, RS; Merchant, JA; Allard, J (4 December 1981). "Mount St Helens eruptions, May 18 to June 12, 1980. An overview of the acute health impact.". JAMA: The Journal of the American Medical Association 246 (22): 2585–9. doi:10.1001/jama.1981.03320220035021. PMID 7029020. https://dx.doi.org/10.1001%2Fjama.1981.03320220035021
- Nania, J; Bruya, TE (April 1982). "In the wake of Mount St Helens.". Annals of Emergency Medicine 11 (4): 184–91. doi:10.1016/S0196-0644(82)80495-2. PMID 7073033. https://dx.doi.org/10.1016%2FS0196-0644%2882%2980495-2
- Olenchock, SA; Mull, JC; Mentnech, MS; Lewis, DM; Bernstein, RS (March 1983). "Changes in humoral immunologic parameters after exposure to volcanic ash.". Journal of Toxicology and Environmental Health 11 (3): 395–404. doi:10.1080/15287398309530353. PMID 6601725. https://dx.doi.org/10.1080%2F15287398309530353
- Baxter, P. J.; Bonadonna, C; Dupree, R; Hards, VL; Kohn, SC; Murphey, MD; Nichols, A; Nicholson, RA et al. (19 February 1999). "Cristobalite in Volcanic Ash of the Soufriere Hills Volcano, Montserrat, British West Indies". Science 283 (5405): 1142–1145. doi:10.1126/science.283.5405.1142. PMID 10024235. Bibcode: 1999Sci...283.1142B. https://dx.doi.org/10.1126%2Fscience.283.5405.1142
- Forbes, L; Jarvis, D; Potts, J; Baxter, PJ (March 2003). "Volcanic ash and respiratory symptoms in children on the island of Montserrat, British West Indies.". Occupational and Environmental Medicine 60 (3): 207–11. doi:10.1136/oem.60.3.207. PMID 12598669. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1740482
- Wehner, AP; Dagle, GE; Clark, ML; Buschbom, RL (August 1986). "Lung changes in rats following inhalation exposure to volcanic ash for two years". Environmental Research 40 (2): 499–517. doi:10.1016/S0013-9351(86)80125-6. PMID 3732218. Bibcode: 1986ER.....40..499W. https://dx.doi.org/10.1016%2FS0013-9351%2886%2980125-6
- Martin, TR; Ayars, G; Butler, J; Altman, LC (November 1984). "The comparative toxicity of volcanic ash and quartz. Effects on cells derived from the human lung.". The American Review of Respiratory Disease 130 (5): 778–82. doi:10.1164/arrd.1984.130.5.778. PMID 6093654. https://dx.doi.org/10.1164%2Farrd.1984.130.5.778
- Martin, TR; Wehner, AP; Butler, J (March 1986). "Evaluation of physical health effects due to volcanic hazards: the use of experimental systems to estimate the pulmonary toxicity of volcanic ash". American Journal of Public Health 76 (3 Suppl): 59–65. doi:10.2105/ajph.76.suppl.59. PMID 3080911. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1651697
- Wiester, MJ; Setzer, CJ; Barry, BE; Mercer, RR; Grady, MA (February 1985). "Inhalation studies of Mt. St. Helens volcanic ash in animals: respiratory mechanics, airway reactivity and deposition". Environmental Research 36 (1): 230–40. doi:10.1016/0013-9351(85)90020-9. PMID 3967640. Bibcode: 1985ER.....36..230W. https://dx.doi.org/10.1016%2F0013-9351%2885%2990020-9
- Raub, JA; Hatch, GE; Mercer, RR; Grady, M; Hu, PC (June 1985). "Inhalation studies of Mt. St. Helens volcanic ash in animals. II. Lung function, biochemistry, and histology". Environmental Research 37 (1): 72–83. doi:10.1016/0013-9351(85)90050-7. PMID 3996343. Bibcode: 1985ER.....37...72R. https://dx.doi.org/10.1016%2F0013-9351%2885%2990050-7
- Beck, BD; Brain, JD; Bohannon, DE (November 1981). "The pulmonary toxicity of an ash sample from the MT. St. Helens Volcano.". Experimental Lung Research 2 (4): 289–301. doi:10.3109/01902148109052324. PMID 7318780. https://dx.doi.org/10.3109%2F01902148109052324
- Lam, CW; James, JT; McCluskey, R; Cowper, S; Balis, J; Muro-Cacho, C (September 2002). "Pulmonary toxicity of simulated lunar and Martian dusts in mice: I. Histopathology 7 and 90 days after intratracheal instillation.". Inhalation Toxicology 14 (9): 901–16. doi:10.1080/08958370290084683. PMID 12396402. https://zenodo.org/record/1234453.
- null
- Shoemaker, DA; Pretty, JR; Ramsey, DM; McLaurin, JL; Khan, A; Teass, AW; Castranova, V; Pailes, WH et al. (1995). "Particle activity and in vivo pulmonary response to freshly milled and aged alpha-quartz.". Scandinavian Journal of Work, Environment & Health 21 Suppl 2: 15–8. PMID 8929681. http://www.ncbi.nlm.nih.gov/pubmed/8929681
- Dalal, NS; Shi, XL; Vallyathan, V (1990). "ESR spin trapping and cytotoxicity investigations of freshly fractured quartz: mechanism of acute silicosis". Free Radical Research Communications 9 (3–6): 259–66. doi:10.3109/10715769009145684. PMID 2167264. https://dx.doi.org/10.3109%2F10715769009145684
- Fenoglio, I; Fonsato, S; Fubini, B (1 October 2003). "Reaction of cysteine and glutathione (GSH) at the freshly fractured quartz surface: a possible role in silica-related diseases?". Free Radical Biology & Medicine 35 (7): 752–62. doi:10.1016/S0891-5849(03)00398-8. PMID 14583339. https://dx.doi.org/10.1016%2FS0891-5849%2803%2900398-8
- Castranova, V; Vallyathan, V; Ramsey, DM; McLaurin, JL; Pack, D; Leonard, S; Barger, MW; Ma, JY et al. (September 1997). "Augmentation of pulmonary reactions to quartz inhalation by trace amounts of iron-containing particles". Environmental Health Perspectives 105 Suppl 5: 1319–24. doi:10.2307/3433554. PMID 9400745. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1470157
- Castranova, V; Porter, D; Millecchia, L; Ma, JY; Hubbs, AF; Teass, A (May–June 2002). "Effect of inhaled crystalline silica in a rat model: time course of pulmonary reactions". Molecular and Cellular Biochemistry 234-235 (1–2): 177–84. doi:10.1007/978-1-4615-1087-1_20. PMID 12162431. https://dx.doi.org/10.1007%2F978-1-4615-1087-1_20
- Porter, DW; Barger, M; Robinson, VA; Leonard, SS; Landsittel, D; Castranova, V (14 June 2002). "Comparison of low doses of aged and freshly fractured silica on pulmonary inflammation and damage in the rat". Toxicology 175 (1–3): 63–71. doi:10.1016/S0300-483X(02)00061-6. PMID 12049836. https://dx.doi.org/10.1016%2FS0300-483X%2802%2900061-6
- Vallyathan, V (December 1994). "Generation of oxygen radicals by minerals and its correlation to cytotoxicity". Environmental Health Perspectives 102 Suppl 10: 111–5. doi:10.2307/3432226. PMID 7705284. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1566993
- Vallyathan, V; Shi, XL; Dalal, NS; Irr, W; Castranova, V (November 1988). "Generation of free radicals from freshly fractured silica dust. Potential role in acute silica-induced lung injury.". The American Review of Respiratory Disease 138 (5): 1213–9. doi:10.1164/ajrccm/138.5.1213. PMID 2849348. Archived from the original on 2011-10-21. https://web.archive.org/web/20111021071713/http://cdc.gov/niosh/nas/RDRP/appendices/chapter3/a3-70.pdf.
- Castranova, V (1 October 2004). "Signaling pathways controlling the production of inflammatory mediators in response to crystalline silica exposure: role of reactive oxygen/nitrogen species.". Free Radical Biology & Medicine 37 (7): 916–25. doi:10.1016/j.freeradbiomed.2004.05.032. PMID 15336307. https://dx.doi.org/10.1016%2Fj.freeradbiomed.2004.05.032
- Ding, M; Shi, X; Dong, Z; Chen, F; Lu, Y; Castranova, V; Vallyathan, V (22 October 1999). "Freshly fractured crystalline silica induces activator protein-1 activation through ERKs and p38 MAPK.". The Journal of Biological Chemistry 274 (43): 30611–6. doi:10.1074/jbc.274.43.30611. PMID 10521445. https://dx.doi.org/10.1074%2Fjbc.274.43.30611
- Vallyathan, V; Kang, JH; Van Dyke, K; Dalal, NS; Castranova, V (July 1991). "Response of alveolar macrophages to in vitro exposure to freshly fractured versus aged silica dust: the ability of Prosil 28, an organosilane material, to coat silica and reduce its biological reactivity.". Journal of Toxicology and Environmental Health 33 (3): 303–15. doi:10.1080/15287399109531529. PMID 1649918. https://dx.doi.org/10.1080%2F15287399109531529
- Portree, DW; Trevino, RC (1997). "Walking to Olympus: An EVA chronology". Monographs in aerospace history series #7. Washington, DC: NASA History Office, NASA Headquarters.
- Wagner, SA (2006). "The Apollo experience lessons learned for Constellation lunar dust management". TP-2006-213726. Johnson Space Center, Houston. http://www.hq.nasa.gov/alsj/TP-2006-213726.pdf.
- Scheuring, Richard A.; Jones, Jeffrey A.; Novak, Joseph D.; Polk, James D.; Gillis, David B.; Schmid, Josef; Duncan, James M.; Davis, Jeffrey R. (1 October 2008). "The Apollo Medical Operations Project: Recommendations to improve crew health and performance for future exploration missions and lunar surface operations". Acta Astronautica 63 (7–10): 980–987. doi:10.1016/j.actaastro.2007.12.065. Bibcode: 2008AcAau..63..980S. https://dx.doi.org/10.1016%2Fj.actaastro.2007.12.065

