 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Jason Zhu | -- | 1434 | 2022-10-10 01:38:24 |
Video Upload Options
Vertebroplasty and kyphoplasty are similar medical spinal procedures in which bone cement is injected through a small hole in the skin (percutaneously) into a fractured vertebra with the goal of relieving back pain caused by vertebral compression fractures. It was found not to be effective in treating osteoporosis-related compression fractures of the spine. The people in both the experimental and placebo groups of the blinded study reported improvement in their pain, suggesting that the benefit noted in unblinded trials is related to the placebo effect. The cost of vertebroplasty in Europe as of 2010 was ~2,500 Euro. As of 2010 in the United States, when done as an outpatient, vertebroplasty costs around 3300 USD while kyphoplasty costs around 8100 USD and when done as an inpatient vertebroplasty cost ~11,000 USD and kyphoplasty 16,000 USD.
1. Effectiveness
The effectiveness of vertebroplasty is not supported as of 2018.[1] The only two randomized placebo controlled trials done as of 2014 found no benefit in those with osteoporosis-related fractures.[2] The subjects in these trials had primarily non-acute fractures and prior to the release of the results they were considered the most ideal people to receive the procedure. After trial results were released vertebroplasty advocates pointed out that people with acute vertebral fractures were not investigated.[3][4] A number of non-blinded trials suggested effectiveness, but the lack of blinding limits what can be concluded from the results and some have been criticized because of being funded by the manufacturer.[3] One analysis has attributed the difference to selection bias.[5]
Some have suggested that this procedure only be done in those with fractures less than 8 weeks old;[6] however, analysis of the two blinded trials appear not to support the procedure even in this acute subgroup.[7] Others consider the procedure only appropriate for those with other health problems making rest possibly detrimental, those with metastatic cancer as the cause of the spine fracture, or those who do not improve with conservative management.[8]
Evidence does not support a benefit of kyphoplasty over vertebroplasty with respect to pain, but the procedures may differ in restoring lost vertebral height, and in safety issues like cement extravasation (leakage).[3] As with vertebroplasty, several unblinded studies have suggested a benefit from balloon kyphoplasty.[9][10] (As of 2012), no blinded studies have been performed, and since the procedure is a derivative of vertebroplasty, the unsuccessful results of these blinded studies have cast doubt upon the benefit of kyphoplasty generally.[11]
Some vertebroplasty practitioners and some health care professional organizations continue to advocate for the procedure.[12][13] In 2010, the Board of Directors of the American Academy of Orthopaedic Surgeons released a statement recommending strongly against use of vertebroplasty for osteoporotic spinal compression fractures,[14] while the Australian Medical Services Advisory Committee considers both vertebroplasty and kyphoplasty only to be appropriate in those who have failed to improve after a trial of conservative treatment,[15] with conservative treatment (analgesics primarily) being effective in two-thirds of people.[16] The National Institute for Health and Care Excellence similarly states that the procedure in those with osteoporotic fractures is only recommended as an option if there is severe ongoing pain from a recent fracture even with optimal pain management.[17]
2. Adverse Effects
Some of the associated risks are from the leak of acrylic cement to outside of the vertebral body. Although severe complications are extremely rare, infection, bleeding, numbness, tingling, headache, and paralysis may ensue because of misplacement of the needle or cement. This particular risk is decreased by the use of X-ray or other radiological imaging to ensure proper placement of the cement.[18] In those who have fractures due to cancer, the risk of serious adverse events appears to be greater at 2%.[16]
The risk of new fractures following these procedures does not appear to be changed; however, evidence is limited,[11] and an increase risk as of 2012 is not ruled out.[19] Pulmonary cement embolism is reported to occur in approximately 2-26% of procedures.[20] It may occur with or without symptoms.[20] Typically, if there are no symptoms, there are no long term issues.[20] Symptoms do occur in about 1 in 2000 procedures.[15] Other adverse effects include spinal cord injury in 0.6 per 1000.[15]
3. Procedure
Vertebroplasty is typically performed by a spine surgeon or interventional radiologist. It is a minimally invasive procedure and patients usually go home the same or next day as the procedure. Patients are given local anesthesia and light sedation for the procedure, though it can be performed using only local anesthetic for patients with medical problems who cannot tolerate sedatives well.
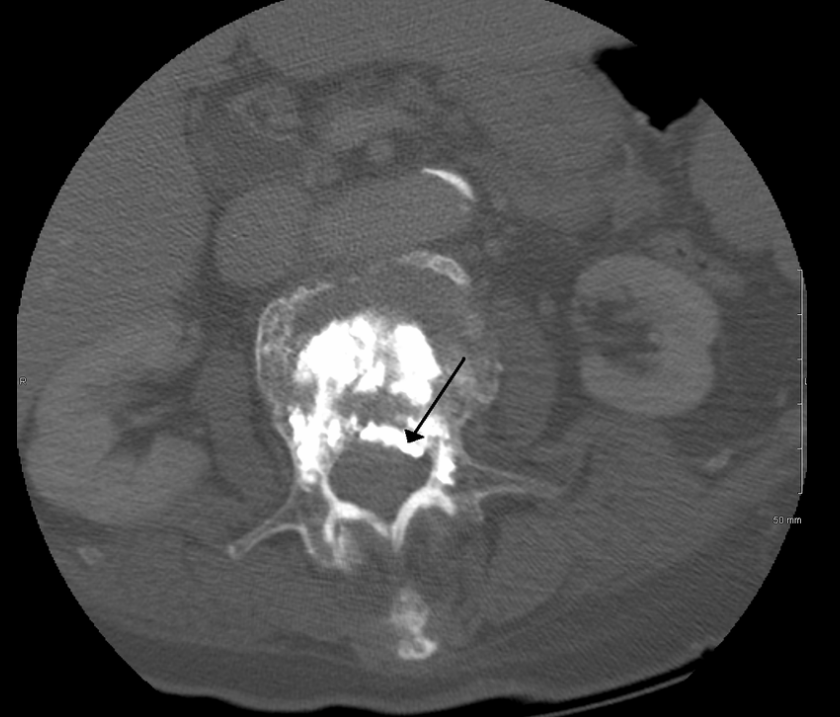
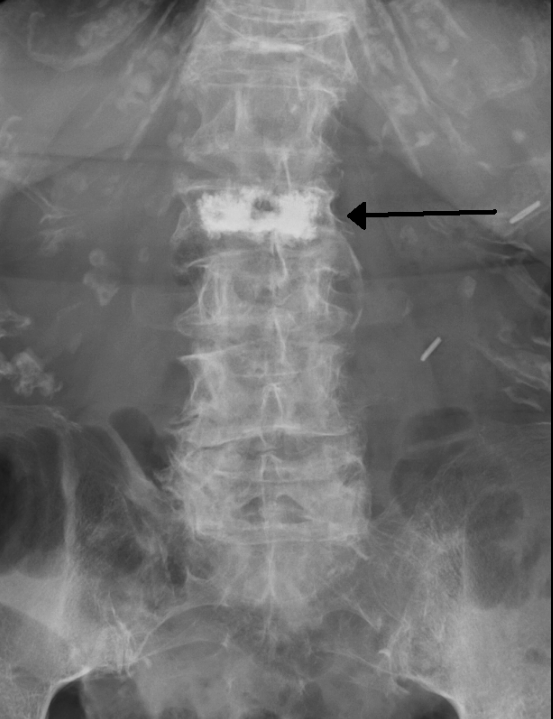
During the procedure, bone cement is injected with a biopsy needle into the collapsed or fractured vertebra. The needle is placed with fluoroscopic x-ray guidance. The cement (most commonly PMMA, although more modern cements are used as well) quickly hardens and forms a support structure within the vertebra that provide stabilization and strength. The needle makes a small puncture in the patient's skin that is easily covered with a small bandage after the procedure.[18]
3.1. Kyphoplasty
Kyphoplasty is a variation of a vertebroplasty which attempts to restore the height and angle of kyphosis of a fractured vertebra (of certain types), followed by its stabilization using injected bone cement. The procedure typically includes the use of a small balloon that is inflated in the vertebral body to create a void within the cancellous bone prior to cement delivery. Once the void is created, the procedure continues in a similar manner as a vertebroplasty, but the bone cement is typically delivered directly into the newly created void.[21]
In a 2011 review Medicare contractor NAS determined that there is no difference between vertebroplasty and kyphoplasty, stating, "No clear evidence demonstrates that one procedure is different from another in terms of short- or long-term efficacy, complications, mortality or any other parameter useful for differentiating coverage."[22]
4. Prevalence
In the United States in 2003 approximately 25,000 vertebroplasty procedures were paid for by medicare.[23] As of 2011/2012 this number may be as high as 70,000-100,000 per year.[24][25]
5. History
Vertebroplasty had been performed as an open procedure for many decades to secure pedicle screws and fill tumorous voids. However, the results were not always worth the risk involved with an open procedure, which was the reason for the development of percutaneous vertebroplasty.
The first percutaneous vertebroplasty was performed in 1984 at the University Hospital of Amiens, France to fill a vertebral void left after the removal of a benign spinal tumor. A report of this and 6 other patients was published in 1987 and it was introduced in the United States in the early 1990s. Initially, the treatment was used primarily for tumors in Europe and vertebral compression fractures in the United States, although the distinction has largely gone away since then.[26]
6. Society and Culture
6.1. Cost
The cost of vertebroplasty in Europe as of 2010 was ~2,500 Euro.[16] As of 2010 in the United States, when done as an outpatient, vertebroplasty costs around 3300 USD while kyphoplasty costs around 8100 USD and when done as an inpatient vertebroplasty cost ~11,000 USD and kyphoplasty 16,000 USD.[27] The cost difference is due to kyphoplasty being an in-patient procedure while vertebroplasty is outpatient, and due to the balloons used in the kyphoplasty procedure.[28] Medicare in 2011 spent about 1 billion USD on the procedures.[25] A 2013 study found that "the average adjusted costs for vertebroplasty patients within the first quarter and the first 2 years postsurgery were $14,585 and $44,496, respectively. The corresponding average adjusted costs for kyphoplasty patients were $15,117 and $41,339. There were no significant differences in adjusted costs in the first 9 months postsurgery, but kyphoplasty patients were associated with significantly lower adjusted treatment costs by 6.8-7.9% in the remaining periods through 2 years postsurgery."[29]
6.2. Medicare Response
In response to the NEJM articles and a medical record review showing misuse of vertebroplasty and kyphoplasty, US Medicare contractor Noridian Administrative Services (NAS) conducted a literature review and formed a policy regarding reimbursement of the procedures. NAS states that in order to be reimbursable, a procedure must meet certain criteria, including, 1) a detailed and extensively documented medical record showing pain caused by a fracture, 2) radiographic confirmation of a fracture, 3) that other treatment plans were attempted for a reasonable amount of time, 4) that the procedure is not performed in the emergency department, and 5) that at least 1 year of follow-up is planned for, among others. The policy, as referenced, applies only to the region covered by Noridian and not all of Medicare's coverage area. It became effective on 20 June 2011.[22]
References
- Buchbinder, R; Johnston, RV; Rischin, KJ; Homik, J; Jones, CA; Golmohammadi, K; Kallmes, DF (4 April 2018). "Percutaneous vertebroplasty for osteoporotic vertebral compression fracture.". The Cochrane Database of Systematic Reviews 4: CD006349. doi:10.1002/14651858.CD006349.pub3. PMID 29618171. https://dx.doi.org/10.1002%2F14651858.CD006349.pub3
- Buchbinder, R; Golmohammadi, K; Johnston, RV; Owen, RJ; Homik, J; Jones, A; Dhillon, SS; Kallmes, DF et al. (30 April 2015). "Percutaneous vertebroplasty for osteoporotic vertebral compression fracture.". The Cochrane Database of Systematic Reviews 4: CD006349. doi:10.1002/14651858.CD006349.pub2. PMID 25923524. https://dx.doi.org/10.1002%2F14651858.CD006349.pub2
- Robinson, Y; Olerud, C (May 2012). "Vertebroplasty and kyphoplasty--a systematic review of cement augmentation techniques for osteoporotic vertebral compression fractures compared to standard medical therapy.". Maturitas 72 (1): 42–9. doi:10.1016/j.maturitas.2012.02.010. PMID 22425141. https://dx.doi.org/10.1016%2Fj.maturitas.2012.02.010
- Gangi, A; Clark, WA (August 2010). "Have recent vertebroplasty trials changed the indications for vertebroplasty?". Cardiovascular and interventional radiology 33 (4): 677–80. doi:10.1007/s00270-010-9901-3. PMID 20523998. https://dx.doi.org/10.1007%2Fs00270-010-9901-3
- McCullough, BJ; Comstock, BA; Deyo, RA; Kreuter, W; Jarvik, JG (Sep 9, 2013). "Major Medical Outcomes With Spinal Augmentation vs Conservative Therapy.". JAMA Internal Medicine 173 (16): 1514–21. doi:10.1001/jamainternmed.2013.8725. PMID 23836009. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=4023124
- Clark, WA; Diamond, TH; McNeil, HP; Gonski, PN; Schlaphoff, GP; Rouse, JC (2010-03-15). "Vertebroplasty for painful acute osteoporotic vertebral fractures: recent Medical Journal of Australia editorial is not relevant to the patient group that we treat with vertebroplasty.". The Medical Journal of Australia 192 (6): 334–7. PMID 20230351. http://www.ncbi.nlm.nih.gov/pubmed/20230351
- Staples, MP; Kallmes, DF; Comstock, BA; Jarvik, JG; Osborne, RH; Heagerty, PJ; Buchbinder, R (Jul 12, 2011). "Effectiveness of vertebroplasty using individual patient data from two randomised placebo controlled trials: meta-analysis.". BMJ (Clinical research ed.) 343: d3952. doi:10.1136/bmj.d3952. PMID 21750078. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=3133975
- Itshayek, E; Miller, P; Barzilay, Y; Hasharoni, A; Kaplan, L; Fraifeld, S; Cohen, JE (June 2012). "Vertebral augmentation in the treatment of vertebral compression fractures: review and new insights from recent studies.". Journal of Clinical Neuroscience 19 (6): 786–91. doi:10.1016/j.jocn.2011.12.015. PMID 22595547. https://dx.doi.org/10.1016%2Fj.jocn.2011.12.015
- "A randomized trial of vertebroplasty for osteoporotic spinal fractures". N. Engl. J. Med. 361 (6): 569–79. August 2009. doi:10.1056/NEJMoa0900563. PMID 19657122. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2930487
- "A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures". N. Engl. J. Med. 361 (6): 557–68. August 2009. doi:10.1056/NEJMoa0900429. PMID 19657121. https://dx.doi.org/10.1056%2FNEJMoa0900429
- Zou, J; Mei, X; Zhu, X; Shi, Q; Yang, H (Jul–Aug 2012). "The long-term incidence of subsequent vertebral body fracture after vertebral augmentation therapy: a systemic review and meta-analysis.". Pain physician 15 (4): E515-22. PMID 22828697. http://www.ncbi.nlm.nih.gov/pubmed/22828697
- Moan R. continues over value of vertebroplasty. Diagnostic Imaging. 2010;32(2) 5. http://www.searchmedica.com/resource.html?rurl=http%3A%2F%2Fwww.diagnosticimaging.com%2Fdisplay%2Farticle%2F113619%2F1533095&q=vertebroplasty&c=ra&ss=diagnosticImagingLink&p=Convera&fr=true&ds=0&srid=1Debate
- Jensen, ME; McGraw, JK; Cardella, JF; Hirsch, JA (July 2009). "Position statement on percutaneous vertebral augmentation: a consensus statement developed by the American Society of Interventional and Therapeutic Neuroradiology, Society of Interventional Radiology, American Association of Neurological Surgeons/Congress of Neurological Surgeons, and American Society of Spine Radiology.". Journal of vascular and interventional radiology : JVIR 20 (7 Suppl): S326-31. doi:10.1016/j.jvir.2009.04.022. PMID 19560019. https://dx.doi.org/10.1016%2Fj.jvir.2009.04.022
- Esses, Stephen I. (September 2010), The Treatment of Symptomatic Osteoporotic Spinal Compression Fractures: Guideline and Evidence Report, American Academy of Orthopaedic Surgeons, http://www.aaos.org/Research/guidelines/SCFguideline.pdf
- Review of interim funded service: Vertebroplasty and New review of Kyphoplasty. Medical Services Advisory Committee. April 2011. ISBN 9781742414560. http://www.msac.gov.au/internet/msac/publishing.nsf/Content/0A8B7AF67EA9D41FCA25766A000DBBEA/$File/27.1%20Assessment%20report%20for%20public%20release%2019-11-11.pdf.
- Montagu, A; Speirs, A; Baldock, J; Corbett, J; Gosney, M (July 2012). "A review of vertebroplasty for osteoporotic and malignant vertebral compression fractures.". Age and Ageing 41 (4): 450–5. doi:10.1093/ageing/afs024. PMID 22417981. https://dx.doi.org/10.1093%2Fageing%2Fafs024
- "Percutaneous vertebroplasty and percutaneous balloon kyphoplasty for treating osteoporotic vertebral compression fractures". April 2013. p. 3. https://www.nice.org.uk/guidance/ta279/resources/guidance-percutaneous-vertebroplasty-and-percutaneous-balloon-kyphoplasty-for-treating-osteoporotic-vertebral-compression-fractures-pdf. Retrieved 17 March 2015.
- Nicole Berardoni M.D, Paul Lynch M.D, and Tory McJunkin M.D. "Vertebroplasty and Kyphoplasty" 2008. Accessed 7 Aug 2009. http://www.arizonapain.com/Vertebroplasty-W.html
- Bliemel, C; Oberkircher, L; Buecking, B; Timmesfeld, N; Ruchholtz, S; Krueger, A (April 2012). "Higher incidence of new vertebral fractures following percutaneous vertebroplasty and kyphoplasty--fact or fiction?". Acta orthopaedica Belgica 78 (2): 220–9. PMID 22696994. http://www.ncbi.nlm.nih.gov/pubmed/22696994
- Wang, LJ; Yang, HL; Shi, YX; Jiang, WM; Chen, L (August 2012). "Pulmonary cement embolism associated with percutaneous vertebroplasty or kyphoplasty: a systematic review.". Orthopaedic surgery 4 (3): 182–9. doi:10.1111/j.1757-7861.2012.00193.x. PMID 22927153. https://dx.doi.org/10.1111%2Fj.1757-7861.2012.00193.x
- Wardlaw, Douglas; Van Meirhaeghe, Jan (2012), "Balloon kyphoplasty in patients with osteoporotic vertebral compression fractures" (in English), Expert Review of Medical Devices 9 (4): 423–436, doi:10.1586/erd.12.27, PMID 22905846, https://dx.doi.org/10.1586/erd.12.27
- Noridian Administrative Services, LLC. "Local Coverage Determination (LCD) for Vertebroplasty, Vertebral Augmentation; Percutaneous (L24383)". Centers for Medicare and Medicaid Services. United States Department of Health and Human Services. http://www.cms.gov/medicare-coverage-database/details/lcd-details.aspx?LCDId=24383&ContrNum=03102. Retrieved 18 October 2011.
- Morrison, WB; Parker, L; Frangos, AJ; Carrino, JA (April 2007). "Vertebroplasty in the United States: guidance method and provider distribution, 2001-2003.". Radiology 243 (1): 166–70. doi:10.1148/radiol.2431060045. PMID 17392252. https://dx.doi.org/10.1148%2Fradiol.2431060045
- "Should You Consider Vertebroplasty? Here’s What the Research Suggests". Mar 1, 2012. http://www.johnshopkinshealthalerts.com/alerts/osteoporosis/benefits-vertebroplasty_6034-1.html. Retrieved 13 January 2013.
- REDBERG, Rita (May 25, 2011). "Squandering Medicare’s Money". New York Times. https://www.nytimes.com/2011/05/26/opinion/26redberg.html?_r=0. Retrieved 18 January 2013.
- Mathis, John M.; Deramond, Hervé; Belkoff, Stephen M., eds (2006) [First edition published 2002]. Percutaneous Vertebroplasty and Kyphoplasty (2nd ed.). Springer Science+Business Media. pp. 3–5. ISBN 0-387-29078-8.
- Mehio, AK; Lerner, JH; Engelhart, LM; Kozma, CM; Slaton, TL; Edwards, NC; Lawler, GJ (August 2011). "Comparative hospital economics and patient presentation: vertebroplasty and kyphoplasty for the treatment of vertebral compression fracture.". AJNR. American journal of neuroradiology 32 (7): 1290–4. doi:10.3174/ajnr.A2502. PMID 21546460. https://dx.doi.org/10.3174%2Fajnr.A2502
- Cloft, HJ; Jensen, ME (February 2007). "Kyphoplasty: an assessment of a new technology.". AJNR. American journal of neuroradiology 28 (2): 200–3. PMID 17296979. http://www.ncbi.nlm.nih.gov/pubmed/17296979
- Ong, KL; Lau, E; Kemner, JE; Kurtz, SM (April 2013). "Two-year cost comparison of vertebroplasty and kyphoplasty for the treatment of vertebral compression fractures: are initial surgical costs misleading?". Osteoporosis international : a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA 24 (4): 1437–45. doi:10.1007/s00198-012-2100-0. PMID 22872070. https://dx.doi.org/10.1007%2Fs00198-012-2100-0

