 +1 credit
+1 credit
Video Upload Options
Respirators, also known as respiratory protective equipment (RPE) or respiratory protective devices (RPD), are used in some workplaces to protect workers from air contaminants. Initially, respirator effectiveness was tested in laboratories, but in the late 1960s it was found that these tests gave misleading results regarding the level of protection provided. In the 1970s, workplace-based respirator testing became routine in industrialized countries, leading to a dramatic reduction in the claimed efficacy of many respirator types and new guidelines on how to select the appropriate respirator for a given environment.
1. Background
File:Respirator Certification - As Vital as the Air We Breathe.webm The invention of the first personal sampling pump[1][2] in 1958 made it possible to simultaneously measure the concentrations of air pollution outside and inside a respirator mask. This was the first attempt to measure the effectiveness of respiratory protective equipment. Until the 1970s experts mistakenly believed that the protective properties of a respirator in the laboratory were not significantly different from its properties in the workplace. There were therefore no measurements of the effectiveness of respirators under production conditions, and the regions where different types of respirators could be safely used were established on the basis of laboratory tests only.
This picture began to change when it was realized in the 1960's that workers using approved respirators were still being exposed to high levels of harmful contaminants.[3] Workplace studies have since shown that the effectiveness of respirators of all designs is much lower in real-world tests than in the laboratory. Under workplace conditions, employees must perform a variety of movements that testers in the lab do not. When the facepiece of the respirator is tightly fitted, these movements cause gaps to form between the mask and the face, decreasing the efficiency of the mask due to leakage of unfiltered air through the gaps. In addition, a small number of testers can not simulate all the variety of shapes and sizes of faces, and a 20-minute certification lab test[4] cannot simulate all the variety of movements performed in workplaces. Testers may also be more careful about putting on and using their masks than an ordinary worker.
2. Evolution of Workplace-Based Testing Standards
2.1. Initial Workplace-Based Tests of Effectiveness in the 1970s and 1980s
A groundbreaking study in 1974 on the effectiveness of respirators used by miners simultaneously measured dust concentrations with personal samplers worn by individual miners, and using two dust collectors, without the mask.[5] The researchers also measured the percentage of time that the miners used their respirators by attaching two thermistors to each minor (one in the facepiece, the other on the belt). Heat detection in the expired air was a sign of wearing a mask. The study defined a new measure, the "effective protection factor", that described the protection offered under real-world conditions, and reported the range of effective protection factors in four different mines.
In the steel fabrication industry, individuals performing sandblasting wore various types of hoods, usually supplied with air. Studies in 1975 found that the concentration of dust under these hoods exceeded the maximum permissible value, although air-supplied hoods offered better protection than non-air-supplied hoods.[6] Even when sandblasting was not occurring, the level of silica dust in the atmosphere far exceeded safe levels, meaning that time workers spent outside the hood on breaks led to exposure.
In copper smelters, three commonly used types of negative pressure filtering respirators with elastomeric half-masks were examined for their ability to protect workers against concentrations of sulfur dioxide in 1976.[7] The different respirator designs showed large variations in protectiveness, partially attributable to the comfort of the respirator design: the more comfortable masks were adjusted more tightly and were therefore more effective.
A 1979 study of the effectiveness of self-contained breathing apparatus (SCBA) in protecting firefighters against inhalation of carbon monoxide showed that intermittent usage of these respirators made them ineffective.[8] Even continuous usage of SCBAs did not provide complete protection. This SCBA design had an air supply into the mask that supplied air "on-demand" (i.e. allowing negative pressure under the mask during inhalation). US and EU legislation now requires the use of breathing apparatus with the "pressure-demand" mode of air supply (i.e. with positive pressure under the mask during inhalation) for firefighters.
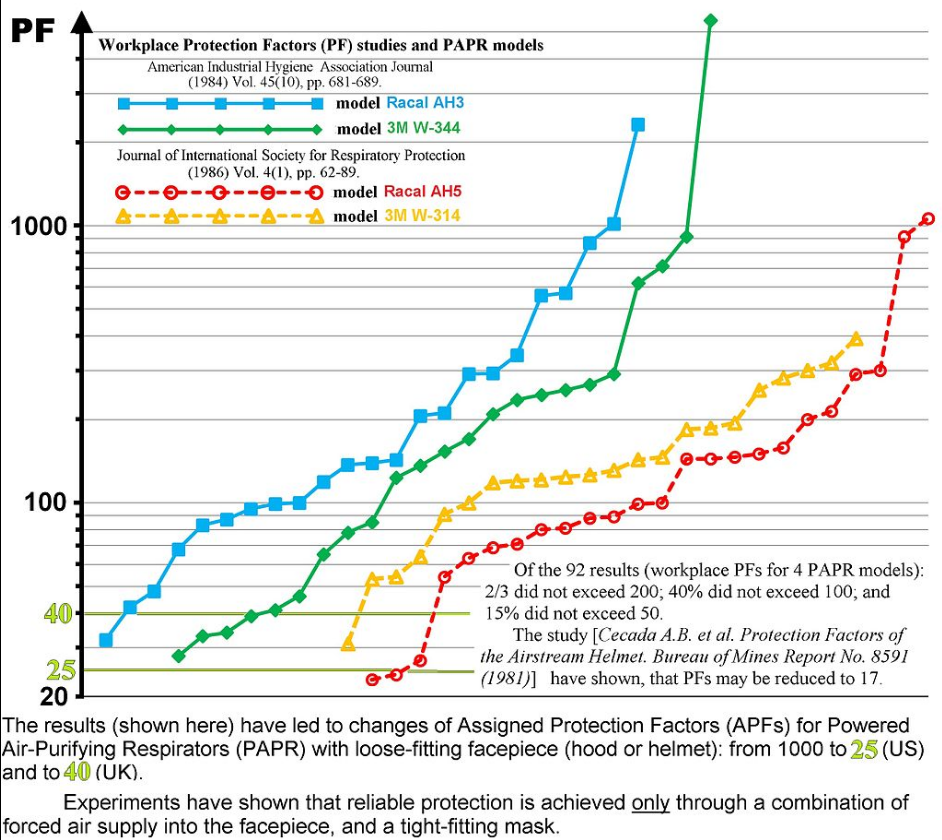
Studies also found that worker-to-worker variation in the use of respirators can have very large effects on the protection achieved. A 1980 study on inhalation exposure of cadmium workers identified a single worker who always used his respirator correctly. The protection factor for this worker was found to be 26 times higher than that for the average worker.[9] In a study in coal mines, miners frequently removed their respirators in conditions where they perceived the dust level to be low, greatly reducing efficacy.[10] In another study, respirators with an expected protection factor of 1000 in fact had protection factors ranging from 15 to 216.[11] Factors affecting the level of protection achieved include the snugness of the fit of the respirator to the worker's face,[12] and air movement in the environment.[13]
2.2. New Measures of Efficacy
As researchers repeatedly found[14][15][16] that the level of protection actually experienced in the workplace was much lower than the protection factors assigned to the devices after laboratory testing, it was proposed that a new expected protection factor scale should be developed, such that the real effectiveness was higher than the "expected effectiveness" with a probability of at least 90%.[14]
The significant differences between real and laboratory-measured effectiveness prompted the National Institute for Occupational Safety and Health (NIOSH) to release two informational messages on respirators in 1982, warning consumers about the unexpectedly low effectiveness of respirators.[17] After extensive discussion, six new definitions of respirator protection factors were agreed upon.[18] For example, the assigned protection factor (APF) of a respirator is the minimum protection factor the respirator must provide under the following circumstances: the respirator will be used by trained and taught workers, after individual selection of masks to fit the face of an employee, and will be used without interruption in the polluted atmosphere.[19] The actual protection experienced by a worker may be significantly lower than this and protection may vary from worker to worker.[20]
2.3. Respirator Efficacy at Chernobyl

The Chernobyl nuclear accident in 1986 led to an urgent need for protection of workers from radioactive aerosols. Approximately 300,000 negative pressure filtering facepieces of the model "Lepestok" were sent to Chernobyl in June 1986.[21] These respirators were considered to be very effective (the declared protection factor for the most common model was 200). However, the individuals who used these respirators were exposed to excessive contamination. Just as in the case of the studies noted above, the declared protection factor was very different from the actual protection factor under real-world conditions.[22] As seen in other workplace tests, the passage of unfiltered air through the gap between the mask and face undermined the efficiency of the respirator.[23][24][25] However, these discoveries did not lead to a change in assessments of the effectiveness of respirators in the USSR.
2.4. Alternatives to Respirator Use
Workplace-based testing has led to extensively revised standards for the use of different designs of respirators,[26][27] and has forced manufacturers to pay more attention to methods of hazard reduction such as sealing, ventilation, and automation, and to improvements in technology. For example, the National Institute for Occupational Safety and Health (USA) has provided recommendations for reducing dust concentrations in coal mines[28] and other mines[29]. Field measurements showed that respirators are the least reliable means of protection, with unstable and unpredictable efficacy.
Respirators are not convenient; they create discomfort and inhibit communication.[30] The reduction of the field of view due to respirator use leads to an increase in the risk of accidents. Respirators also reinforce overheating at high air temperature.[31] In real-world conditions, these deficiencies often lead to workers removing their respirators periodically, further reducing the efficacy of the respirator. In addition, respirators only protect workers against harmful substances entering the body through the respiratory system, whereas pollutants frequently also enter the body through the skin.[32][33] Respirators thus cannot be used as substitutes for other measures that reduce the impact of air pollution on workers. However, if the respiratory system is the main way that harmful substances enter the body, and if other means of protection do not reduce the impact to an acceptable value, respirators may be a useful supplement. To maximize effectiveness, the type of respirator should be selected for the specific situation, masks should be chosen for employees personally, and workers should be trained to use the respirator effectively.
3. Reduction in Permissible Exposure Limits
Legislation in industrialized countries establishes limitations on the use of all types of respirators, taking into account the results of field trials of efficacy. The permissible exposure limit [PEL] for several types of respirators was reduced. For example, for negative pressure air-purifying respirators with full face mask and high-efficiency filters, the limits were reduced from 500 PEL to 50 PEL (USA[14]), and from 900 OEL to 40 OEL (UK[31]); for powered air-purifying respirators with a loose-fitting facepiece (hood or helmet), limits were reduced from 1000 PEL to 25 PEL (USA[15]); for powered air-purifying respirators with half mask, limits were reduced from 500 PEL to 50 PEL (USA[14]); for supplied air respirators with full face mask and continuous air supply mode, limits were reduced from 100 OEL to 40 OEL (UK[34]); for self-contained breathing apparatus respirators with air supply on demand, limits were reduced from 100 PEL to 50 PEL (USA). Filtering facepieces and negative pressure half-mask respirators were limited to 10 PEL in the USA.[35]
| Respirator type, country | Requirements for protection factor for certification (2013) | Permissible exposure limits prior to workplace testing (year) | Permissible exposure limits after workplace testing (2013) | Minimum values of measured workplace protection factors |
|---|---|---|---|---|
| PAPR with helmet, USA | > 250 000[4] | up to 1000 PEL | up to 25 PEL[27] | 28, 42 ... |
| Negative pressure air-purifying respirator with full face mask, USA | > 250 000[4] | up to 100 PEL (1980) | up to 50 PEL[27] | 11, 16, 17 ... |
| Negative pressure air-purifying respirator with full face mask, UK | > 2000 (for gases) or >1000 (for aerosols) | up to 900 OEL (1980) | up to 40 OEL | |
| Negative pressure air-purifying respirator with half mask facepiece, USA | > 25 000[4] | up to 10 PEL (since the 1960s[27]) | 2.2, 2.8, 4 ... | |
| Self-contained breathing apparatus with air supply on demand, USA | > 250 000[4] | up to 1000 PEL (1992) | up to 50 PEL[27] | Monitoring showed low efficiency for carbon monoxide exposure |
The National Institute for Occupational Safety and Health of the USA now requires the manufacturers of high-performance RPE to perform testing at representative workplaces as a requirement for certification.[36]
References
- Sherwood, Robert (1966). "On the Interpretation of Air Sampling for Radioactive Particles" (in en). American Industrial Hygiene Association Journal 27 (2): 98–109. doi:10.1080/00028896609342800. ISSN 1542-8117. PMID 5954012. http://www.tandfonline.com/toc/aiha20/27/2. Retrieved 10 July 2016.
- Sherwood, Robert; Greenhalgh, D.M.S. (1960). "A Personal Air Sampler" (in en). The Annals of Occupational Hygiene 2 (2): 127–132. doi:10.1093/annhyg/2.2.127. ISSN 0003-4878. http://annhyg.oxfordjournals.org/content/2/2/. Retrieved 10 July 2016.
- Cralley, Lesly; Cralley, Lester (1985). "..". Patty's Industrial Hygiene and Toxicology. 3A (2 ed.). New York: Willey-Interscience. pp. 677–678. ISBN:0 471-86137-5.
- NIOSH standard 42 Code of Federal Register Part 84 "Respiratory Protective Devices" http://cfr.regstoday.com/42cfr84.aspx
- Harris, H.E.; DeSieghardt, W.C.; Burgess, W. A.; Reist, Parker (1974). "Respirator Usage and Effectiveness in Bituminous Coal Mining Operations" (in en). American Industrial Hygiene Association Journal 35 (3): 159–164. doi:10.1080/0002889748507018. ISSN 1542-8117. PMID 4522752. https://www.tandfonline.com/doi/abs/10.1080/0002889748507018. Retrieved 10 July 2016.
- Behzad, Samimi; Neilson, Arthur; Weill, Hans; Ziskind, Morton (1975). "The Efficiency of Protective Hoods Used by Sandblasters to Reduce Silica Dust Exposure" (in en). American Industrial Hygiene Association Journal 36 (2): 140–148. doi:10.1080/0002889758507222. ISSN 1542-8117. PMID 167570. https://www.tandfonline.com/doi/abs/10.1080/0002889758507222. Retrieved 10 July 2016.
- Moore, David; Smith, Thomas (1976). "Measurement of protection factors of chemical cartridge, half-mask respirators under working conditions in a copper smelter" (in en). American Industrial Hygiene Association Journal 37 (8): 453–458. doi:10.1080/0002889768507495. ISSN 1542-8117. PMID 970320. https://www.tandfonline.com/doi/abs/10.1080/0002889768507495. Retrieved 10 July 2016.
- Levin, Marshal (1979). "Respirator use and protection from exposure to carbon monoxide" (in en). American Industrial Hygiene Association Journal 40 (9): 832–834. doi:10.1080/15298667991430361. ISSN 1542-8117. PMID 517443. https://www.tandfonline.com/doi/abs/10.1080/15298667991430361. Retrieved 10 July 2016.
- Smith, Thomas; Ferrel, Willard; Varner, Michael; Putnam, Robert (1980). "Inhalation exposure of cadmium workers: effects of respirator usage" (in en). American Industrial Hygiene Association Journal 41 (9): 624–629. doi:10.1080/15298668091425400. ISSN 1542-8117. http://www.tandfonline.com/toc/aiha20/41/9. Retrieved 10 July 2016.
- Howie, Robin M.; Walton, W.H. (1981). "Practical Aspects of the Use of Respirators in the British Coal Mines". in Brian Ballantyne & Paul Schwabe (in en). Respiratory Protection. Principles and Applications. London, New York: Chapman & Hall. pp. 287–298. ISBN 978-0412227509.
- Myers, Warren; Peach, M.J. III (1983). "Performance measurements on a powered air-purifying respirator made during actual field use in a silica bagging operation" (in en). The Annals of Occupational Hygiene 27 (3): 251–259. doi:10.1093/annhyg/27.3.251. ISSN 0003-4878. https://www.tandfonline.com/doi/abs/10.1080/15298668391405670. Retrieved 10 July 2016.
- Que Hee, Shane; Lawrence, Philip (1983). "Inhalation Exposure of Lead in Brass Foundry Workers: The Evaluation of the Effectiveness of a Powered Air-Purifying Respirator and Engineering Controls" (in en). American Industrial Hygiene Association Journal 44 (10): 746–751. doi:10.1080/15298668391405670. ISSN 1542-8117. PMID 6650396. http://www.tandfonline.com/toc/aiha20/44/10. Retrieved 10 July 2016.
- Cecala, Andrew B.; Volkwein, Jon C.; Thomas, Edward D.; Charles W. Urban (1981) (in en). Protection Factors of the Airstream Helmet. Bureau of Mines Report No. 8591. p. 10.
- Lenhart, Steven; Campbel, Donald (1984). "Assigned protection factors for two respirators types based upon workplace performance testing" (in en). The Annals of Occupational Hygiene 28 (2): 173–182. doi:10.1093/annhyg/28.2.173. ISSN 0003-4878. PMID 6476685. http://annhyg.oxfordjournals.org/content/28/2/. Retrieved 10 July 2016.
- Myers, Warren; Peach III, Michael; Cutright, Ken; Iskander, Wafik (1984). "Workplace Protection Factor Measurements on Powered Air-Purifying Respirators at a Secondary Lead Smelter: Results and Discussion" (in en). American Industrial Hygiene Association Journal 45 (10): 681–688. doi:10.1080/15298668491400449. ISSN 1542-8117. PMID 6496315. https://www.tandfonline.com/doi/abs/10.1080/15298668491400449. Retrieved 10 July 2016.
- Myers, Warren; Peach III, Michael; Cutright, Ken; Iskander, Wafik (1986). "Field Test of Powered Air-Purifying Respirators at a Battery Manufacturing Facility" (in en). Journal of the International Society for Respiratory Protection 4 (1): 62–89. ISSN 0892-6298. http://www.isrp.com.
- Nancy J. Bollinger, Robert H. Schutz, ed (1987) (in en). NIOSH Guide to Industrial Respiratory Protection. DHHS (NIOSH) Publication No 87-116. Cincinnati, Ohio: National Institute for Occupational Safety and Health. p. 305. doi:10.26616/NIOSHPUB87116. https://www.cdc.gov/niosh/docs/87-116/.
- Miller, Donald (1987) (in en). NIOSH Respirator Decision Logic. DHHS (NIOSH) Publication No. 87-108. National Institute for Occupational Safety and Health. p. 61. doi:10.26616/NIOSHPUB87108. https://www.cdc.gov/niosh/docs/87-108/. Retrieved 16 July 2016.
- Occupational Safety and Health Administration, US Department of Labor (2009). "Assigned Protection Factors for the Revised Respiratory Protection Standard". https://www.osha.gov/Publications/3352-APF-respirators.pdf.
- Zhuang, Ziqing; Coffey, Christopher; Campbell, Donald; Lawrence, Robert; Myers, Warren (2003). "Correlation Between Quantitative Fit Factors and Workplace Protection Factors Measured in Actual Workplace Environments at a Steel Foundry" (in en). American Industrial Hygiene Association Journal 64 (6): 730–738. doi:10.1080/15428110308984867. ISSN 1542-8117. http://www.tandfonline.com/toc/aiha20/64/6. Retrieved 10 July 2016.
- Petryanov, Igor et al. (2015) (in ru). ["Lepestok". Filterring facepieces] (2 ed.). Moscow: Nauka. p. 320. ISBN 978-5-02-039145-1.
- Hoover, Mark D.; Lackey, Jack R.; Vargo, George J. (2001). "Results and Discussion" (in en). Independent Evaluation of The Lepestok Filtering Facepiece Respirator. PNNL-13581; LRRI-20001202. Albuquerque, NM: Lovelace Respiratory Research Institute, Pacific Northwest National Laboratory (U.S. Department of Energy). pp. 13–20. http://www.pnl.gov/main/publications/external/technical_reports/pnnl-13581.pdf. Retrieved 16 July 2016.
- Ogorodnikov, Boris; Pasukhin, Edward (2006). "[Respiratory protective devices"] (in ru). [Radioactive aerosols of the object "Ukryttya" (a review). Part 5. Means for sampling and analyses of aerosols. Radioactive aerosols in lungs]. Preprint 06-6. Chernobyl: National Academy of Sciences of Ukraine. Institute for safety problems of nuclear power plants. pp. 10–28. http://www.iaea.org/inis/collection/NCLCollectionStore/_Public/39/116/39116456.pdf. Retrieved 16 July 2016.
- Galushkin, B.A.; Gorbunov, S.V. (1990). "[The efficiency of a filtering matherial ФПП-15-1.5]". in Victor Kashcheev (in ru). [Abstracts of the III All-Union Conference "Experimental physiology, hygiene and personal protection of the person"]. Moscow: The Ministry of Health of the USSR, Institute of Biophysics. pp. 12–13.
- Galushkin, B.A.; Gorbunov, S.V. (1990). "[Experimental studies to determine the protection factor of the filtering facepiece respirator "Lepestok-200" during emergency operations at the Chernobyl nuclear power plant ]". in Victor Kashcheev (in ru). [Abstracts of the III All-Union Conference "Experimental physiology, hygiene and personal protection of the person"]. Moscow: The Ministry of Health of the USSR, Institute of Biophysics. pp. 11–12.
- Technical Committee PH/4, Respiratory protection, ed (1997) (in en). British Standard BS 4275:1997 "Guide to implementing an effective respiratory protective device programme" (3 ed.). 389 Chiswick High Road, London: British Standards Institution. ISBN 0-580-28915 X.
- OSHA standard 29 CFR 1910.134 "Respiratory Protection" http://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=STANDARDS&p_id=12716
- Colinet, Jay F.; Rider, James P.; Listak, Jeffrey M. (2010) (in en). Best Practices for Dust Control in Coal Mining. Information Circular 9517. DHHS (NIOSH) Publication No. 2010–110. John A. Organiscak, and Anita L. Wolfe. Pittsburgh, PA - Spokane, WA: National Institute for Occupational Safety and Health. p. 84. https://www.cdc.gov/niosh/mining/works/coversheet861.html. Retrieved 16 July 2016.
- Cecala, Andrew B.; O’Brien, Andrew D.; Schall, Joseph (2012) (in en). Dust Control Handbook for Industrial Minerals Mining and Processing. Report of Investigations 9689. DHHS (NIOSH) Publication No. 2012–112. Jay F. Colinet, William R. Fox, Robert J. Franta, Jerry Joy, Wm. Randolph Reed, Patrick W. Reeser, John R. Rounds, Mark J. Schultz. Pittsburgh, PA; Spokane, WA: National Institute for Occupational Safety and Health. p. 314. https://www.cdc.gov/niosh/mining/works/coversheet1765.html. Retrieved 16 July 2016.
- Janssen, Larry; Bidwell, Jeanne (2007). "Performance of a Full Facepiece, Air-Purifying Respirator Against Lead Aerosols in a Workplace Environment" (in en). Journal of Occupational and Environmental Hygiene 4 (2): 123–128. doi:10.1080/15459620601128845. ISSN 1545-9632. http://www.tandfonline.com/toc/uoeh20/4/2. Retrieved 15 July 2016.
- Ming-Tsang, Wu (2002). "Assessment of the Effectiveness of Respirator Usage in Coke Oven Workers" (in en). American Industrial Hygiene Association Journal 63 (1): 72–75. doi:10.1080/1542811020898469. ISSN 1542-8117. http://www.tandfonline.com/toc/aiha20/63/1. Retrieved 10 July 2016.
- Chang, Fu-Kuei; Chen, Mei-Lien; Cheng, Shu-Fang; Shih, Tung-Sheng; Mao, I-Fang (2007). "Evaluation of dermal absorption and protective effectiveness of respirators for xylene in spray painters" (in en). International Archives of Occupational and Environmental Health 81 (2): 145–150. doi:10.1007/s00420-007-0197-9. ISSN 0340-0131. PMID 17492305. https://link.springer.com/journal/420/81/2/page/1. Retrieved 16 July 2016.
- Lof, Agneta; Brohede, Christina; Gullstrand, Elisabeth; Lindstrom, Karin; Sollenberg, Jan; Wrangskog, Kent; Hagberg, Mats; Hedman, Birgitta Kolmodin (1993). "The effectiveness of respirators measured during styrene exposure in a plastic boat factory" (in en). International Archives of Occupational and Environmental Health 65 (1): 29–34. doi:10.1007/BF00586055. ISSN 0340-0131. PMID 8354572. https://link.springer.com/journal/420/65/1/page/1. Retrieved 16 July 2016.
- Clayton, Mike; Bancroft, B.; Rajan-Sithamparanadarajah, Bob (2002). "A Review of Assigned Protection Factors of Various Types and Classes of Respiratory Protective Equipment with Reference to their Measured Breathing Resistances" (in en). The Annals of Occupational Hygiene 46 (6): 537–547. doi:10.1093/annhyg/46.6.537. ISSN 0003-4878. http://annhyg.oxfordjournals.org/content/46/6/. Retrieved 10 July 2016.
- Bollinger, Nancy; Campbell, Donald; Coffey, Christopher (2004). "III. Respirator Selection Logic Sequence" (in en). NIOSH Respirator Selection Logic. DHHS (NIOSH) Publication No. 2005-100. NIOSH Respirator Policy Group; Heinz Ahlers, Roland BerryAnn, Frank Hearl, Richard Metzler, Teresa Seitz, Douglas Trout and Ralph Zumwalde. Cincinnati, OH: The National Institute for Occupational Safety and Health (NIOSH). pp. 3–16. https://www.cdc.gov/niosh/docs/2005-100/.
- Johnson, Alan; Myers, Warren; Colton, Craig; Birkner, J.S.; Campbell, C.E. (1992). "Review of respirator performance testing in the workplace: issues and concerns" (in en). American Industrial Hygiene Association Journal 53 (11): 705–712. doi:10.1080/15298669291360409. ISSN 1542-8117. PMID 1442561. http://www.tandfonline.com/toc/aiha20/53/11. Retrieved 10 July 2016.

