Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Ebtesam Abdullah Al-Suhaimi | -- | 1461 | 2022-07-11 20:58:21 | | | |
| 2 | Rita Xu | Meta information modification | 1461 | 2022-07-12 03:35:39 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Aljafary, M.A.; Al-Suhaimi, E.A. Adiponectin System (Rescue Hormone). Encyclopedia. Available online: https://encyclopedia.pub/entry/25022 (accessed on 08 August 2026).
Aljafary MA, Al-Suhaimi EA. Adiponectin System (Rescue Hormone). Encyclopedia. Available at: https://encyclopedia.pub/entry/25022. Accessed August 08, 2026.
Aljafary, Meneerah Abdulrahman, Ebtesam Abdullah Al-Suhaimi. "Adiponectin System (Rescue Hormone)" Encyclopedia, https://encyclopedia.pub/entry/25022 (accessed August 08, 2026).
Aljafary, M.A., & Al-Suhaimi, E.A. (2022, July 11). Adiponectin System (Rescue Hormone). In Encyclopedia. https://encyclopedia.pub/entry/25022
Aljafary, Meneerah Abdulrahman and Ebtesam Abdullah Al-Suhaimi. "Adiponectin System (Rescue Hormone)." Encyclopedia. Web. 11 July, 2022.
Copy Citation
The adipose tissue, regardless of its role in generating and storing energy, acts as a key player as an endocrine tissue, producing a wide scale of cytokines/hormones called adipokines. Adipokines such as leptin, resistin, visfatin and osteopontin own pro-inflammatory effects on the cardiovascular system in some cases. In contrast, some adipokines have cardioprotective and anti-inflammatory impacts including adiponectin, omentin, and apelin.
adiponectin
hormone
receptor
1. Introduction
Adiponectin is a protein hormone discovered in 1995 comprised of 244 amino acids with a molecular weight of 28 kDa. It has a single-chain trimer structure which is a changeable N-terminal, a collagen domain, and a C-terminal round area similar to the immune complement C1. Three globular areas are located by the End-N, and C ends are linked by the Pro104-Tyr109 point. This single-chain trimer is concealed by a gong-formed shell. This structure is similar to the membrane construction of some proteins of the immune complement system, particularly C1q family and the three-dimensional shape of the tumor necrosis factor (TNF) family. The globular part is similar to the C1q-TNF superfamily, with difference in sequences of their amino acids [1].
Adiponectin exists in the blood as a dimer [2]; it also has a trimer form or protein molecule of large molecular weight hexamers and multimer (90, 180, and >400 kDa). The longitudinal structure of adiponectin is not commonly present in healthy status because of their thermodynamic instability [1][2]. Adiponectin has been related to many physiological functions such as immune response and inflammation, insulin sensitivity, energy regulation, and lipid metabolism [3]. Adiponectin is a hormone derived from adipocytes; it is found in many oligomeric forms in the plasma and has been found to be beneficial in cases of heart ischemia-reperfusion injury [4]. It has been reported that obesity affects glucose and lipid metabolism, in addition to being responsible for the alteration of heart structure and function. An increase in inflammatory cytokines is also caused by obesity. Adipokines are cytokines released by the adipocytes and have been found to have both anti-inflammatory and pro-inflammatory affects. Adiponectin, omentin, apelin, and secreted frizzled-related protein (Sfrp-5) possess anti-inflammatory and cardioprotective effects, while leptin, visfatin, tumor necrosis factor (TNF), resistin, osteopontin, and retinol-binding protein4 (RBP-4) have pro-inflammatory effects on the cardiovascular system, and preliminary findings link cardiovascular diseases to unhealthy metabolism [5]. Plasma concentration parameters of adiponectin and resistin measured in echocardiographic examination of coronary artery disease (CAD) patients were found to be related to cardiac remodeling and dysfunction [6]. Changes of the heart muscle, functional and morphological, have been noticed to be more significant in patients with chronic heart failure in addition to metabolic syndrome (MS) (combination of diabetes, obesity, and hypertension), than patients without MS [7]. A study of 47 polycystic ovary syndrome (PCOS) cases and 35 healthy subjects assessed the relation between an early diagnosis marker of atherosclerosis known as carotid intima-media thickness (CIMT), and an adipokine initially secreted from visceral adipose tissue known as omentin-1. It was found that an increase in CIMT was linked to cardiovascular risk in patients with PCOS, and serum omentin-1 was independently linked with age, as it was uncovered in early PCOS cases that it is acting as a protective acute-phase reactant [8]. Epicardial adipose tissue (EAT) has been noticed to regulate adipogenesis, insulin resistance, renin angiotensin-aldosterone system (RAAS), cardiac remodeling and output, by which it facilitates physiological and pathophysiological processes of coronary failure. Through paracrine, endocrine and vasocrine pathways, EAT secretes a wide range of adipokines, adrenomedullin, miRNA and adiponectin related to the progress of cardiovascular disease via intracellular and extracellular mechanisms [9].
2. Physiology and Pathophysiology of Adiponectin on the Cardiovascular System
The role of adipose tissue as an endocrine organ is clearly indicated by the secretion of adiponectin and other adipokines, affecting the cardiovascular system at both cellular and molecular levels; it is now known to have anti-apoptotic, anti-inflammatory, and antioxidant roles, hence reducing the pathogenic effects of cardiovascular disease (CVD), therefore it is described as a “rescue hormone”. Adiponectin piles up in the sub-endothelium of heart arteries in humans whenever it suppresses the adhering of monocytes to endothelial cells and finally reduces the migration and proliferation of smooth muscles of blood vessels that promote atherosclerosis [10]. The circulating levels of adiponectin in addition to the expressed adiponectin in adipose tissue have been seen to be elevated in advanced CVD [11]. Accumulation of adiponectin was found in the heart after ischemic damage. Half-life of adiponectin was found to be longer in heart tissues than that of circulating plasma adiponectin [4].
Both hyperleptinemia and hypoadiponectinemia associated with obesity are important biomarkers to aid in the prediction of cardiovascular outcomes. The maintenance of proper cardiovascular functions is linked to normal levels of leptin and adiponectin. Cardiovascular disorders occur with insufficient adiponectin and leptin signaling, yet, in pathogenesis of cardiovascular disorders, elevated levels of both leptin and adiponectin are found [12]. Adiponectin is not only secreted by adipose tissue, but also by cardiomyocytes and connective tissue cells of the heart. Adiponectin is known to affect the cardiovascular system and its metabolism, as its decrease has been found to be a factor in the development of many cardiovascular diseases [13]. Furthermore, adiponectin has high plasma concentrations possessing anti-fibrotic, antioxidant and anti-inflammatory effects which regulate glucose levels and insulin sensitivity. Weight loss has been found to increase adiponectin levels, which in turn increases insulin sensitivity. Therefore, new drugs for cancer and cardiovascular diseases may use the adiponectin pathway, as they are diseases affected by insulin resistance [14]. The degree of vascular endothelial injury of patients with both diabetes mellitus (DM) and coronary heart disease, has been observed to be closely related to serum adiponectin, C-reactive protein levels, and insulin resistance [15].
In a study about family history of type 2 diabetes mellitus (FH-DM), 332 Japanese women aged 18–24 years were involved, and it was suggested that microvascular dysfunction may contribute to elevation of blood pressure, as FH-DM was linked to hypertension [16]. Mid-regional pro-adrenomedullin (MR-proADM) has vasodilatory effects but also is associated with cardiovascular mortality. The study noticed that MR-proADM was associated with (abdominal) obesity, through selected adipokines (retinol-binding protein-4, adiponectin, chemerin, and leptin), and subclinical inflammatory biomarkers (interleukin-1 receptor antagonist, interleukin-6, interleukin-22, myeloperoxidase, and high-sensitivity C-reactive protein) [17].
RBP4 is an adipocytokine involved in atherosclerosis, while the adiponectin plays a unique effect as an anti-inflammatory adipocytokine. Ref. [18] recruited 168 patients aged 88 with peripheral artery disease (PAD) to study their potential prognostic function in major adverse cardiovascular events (MACE). It was found that an increase in RBP4 and decrease in adiponectin serum concentrations are independently linked with PAD appearance. Furthermore, RBP4 is an autonomous predictor for MACE happening in PAD’s patients.
Figure 1 explains adiponectin sources and lists the physiological functions, while Figure 2 includes the general pathological roles of adiponectin.
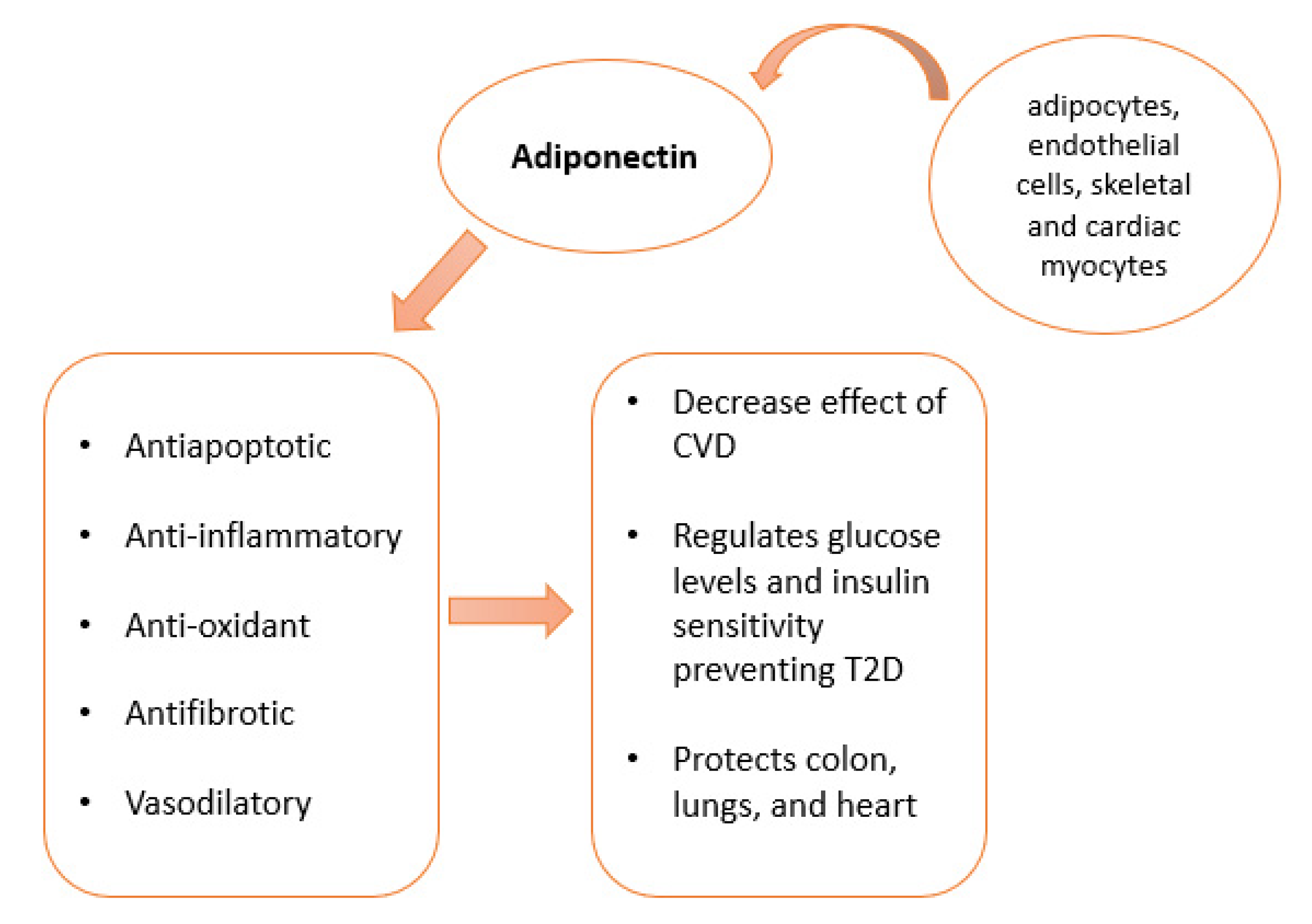
Figure 1. Adiponectin sources: Adiponectin is produced by adipocytes, endothelial and skeletal cells. Cardiac myocytes are also able to produce adiponectin. Its functions include antiapoptotic, anti-inflammatory, antioxidant, and anti-fibrotic effects. Adiponectin protects against CDV, controls glucose and insulin, and protects against heart, lung, and colon diseases.
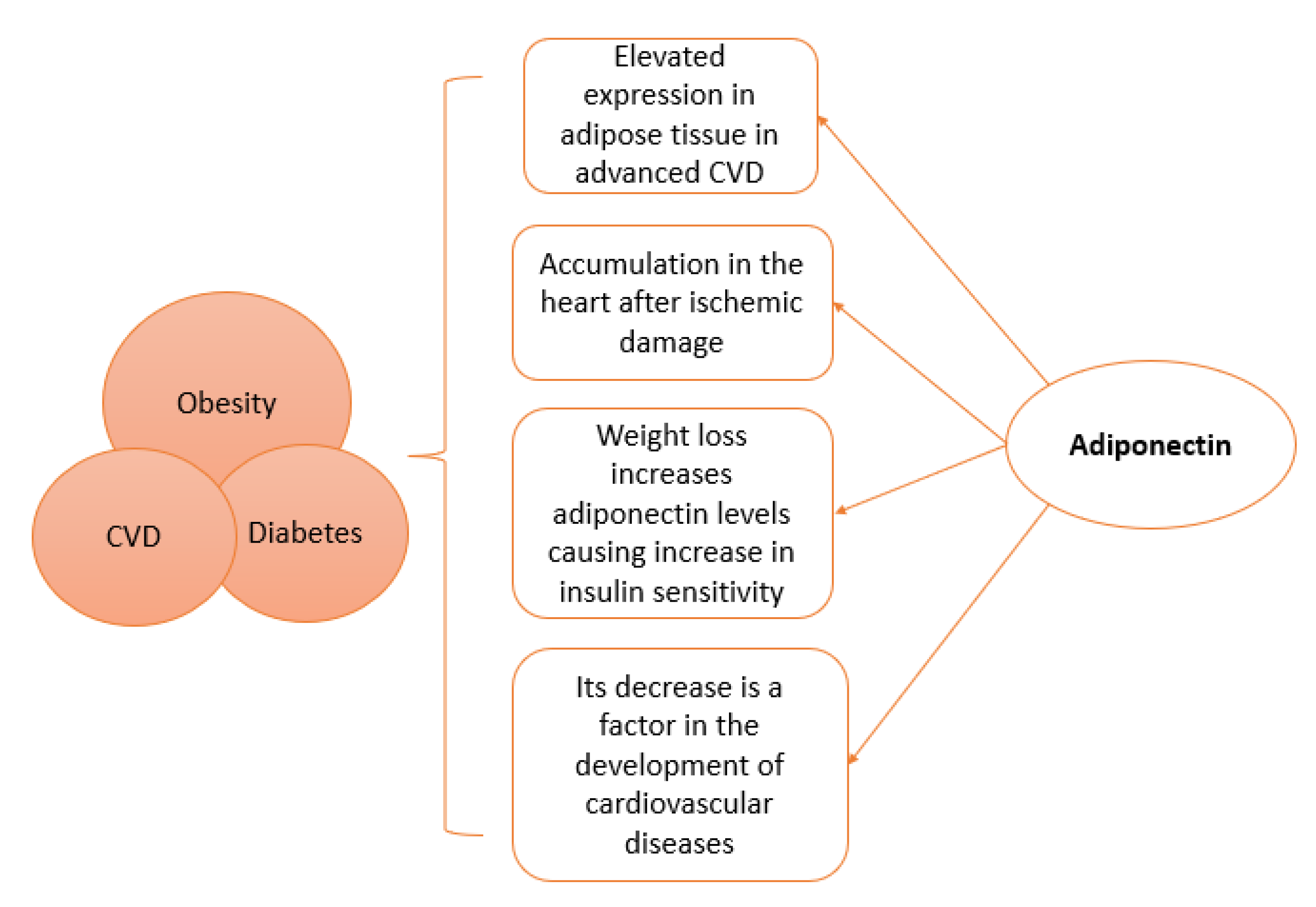
Figure 2. Physiological and pathological links of adiponectin to Obesity, Cardiovascular disease (CVD), and Diabetes.
3. Paradoxal Effect of Adiponectin
In general, the clinical importance of adiponectin as a biomarker is still greatly promising, particularly for metabolic and cardiovascular syndromes [19][20]. However, clinical explanations of blood adiponectin concentrations should be tested according to certain factors like patient’s history of CVD, gender [11][21], hypertension [22] age, and hemoglobin levels [23]. Basic science research has demonstrated useful effects of adiponectin molecule on glucose balance, apoptosis, ROS stress, chronically low-grade inflammation, and atherosclerosis, cardiac systolic, hypertension, etc. However, ref. [21] found that human research indicated that adiponectin is just a marker for glucose homeostasis, without immediate action related to the risk of type 2 DM and cardiovascular disorders. However, adiponectin has a paradox effect, the part played by adiponectin on the risk of mortality. Instead of the reversed relationship, there is a positive link between adiponectin and mortality average in several clinical cases including DM. The biology implied that this paradoxical effect is not clear. Without strong results, this may refer to adiponectin resistance and the confusing function of natriuretic peptides. Genetically, there is a direct function of adiponectin in increasing the risk of death. Since there is no creditable and robust evidence, additional studies are therefore required to uncover the clever roles of adiponectin on healthy cardio metabolism and its paradoxical role with death rate. For further explanation, plasma total adiponectin and high-molecular weight polymeric adiponectin are robustly positively associated with insulin sensitivity. However, ref. [24] demonstrated paradoxical hyperadiponectinemia in patients with acute insulin resistance because of a genetic defect in insulin receptors. This reveals one or both possible mechanisms: (1) key physiological function of insulin receptors in regulating production of adiponectin and (2) absence or dysfunction of insulin receptors affect adiponectin concentrations. Hyperadiponectinemia solved equally with decrease in antibodies of insulin receptors and dissolution of insulin resistance clinically. Figure 3 lists paradoxical effect of adiponectin
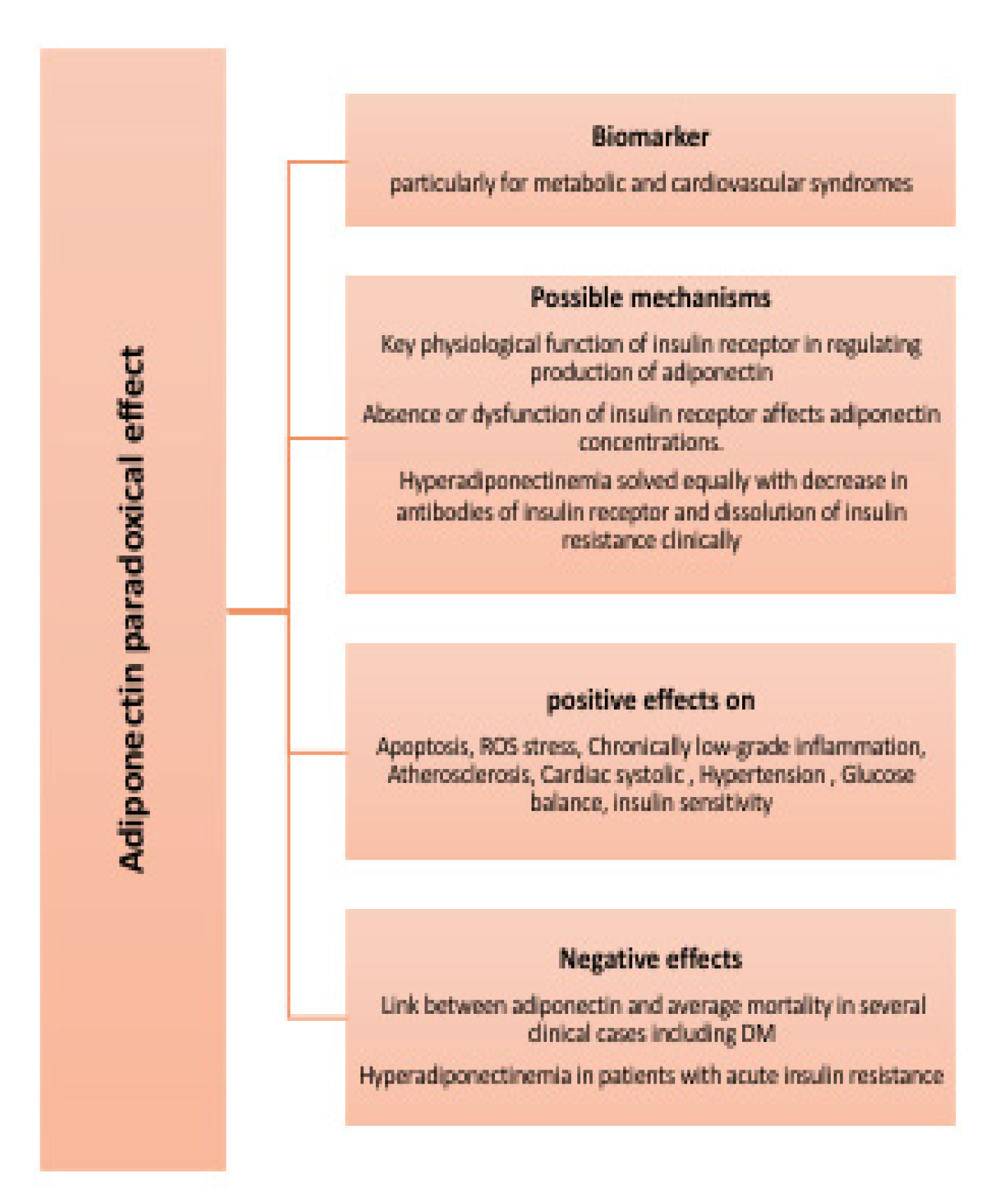
Figure 3. Paradoxical effect of adiponectin.
References
- Hamdy, O.; Porramatikul, S.; Al-Ozairi, E. Metabolic obesity: The paradox between visceral and subcutaneous fat. Curr. Diabetes Rev. 2006, 2, 367–373.
- Fisman, E.Z.; Tenenbaum, A. Adiponectin: A manifold therapeutic target for metabolic syndrome, diabetes, and coronary disease? Cardiovasc. Diabetol. 2014, 13, 103.
- Khoramipour, K.; Chamari, K.; Hekmatikar, A.; Ziyaiyan, A.; Taherkhani, S.; Elguindy, N.; Bragazzi, N. Adiponectin: Structure, Physiological Functions, Role in Diseases, and Effects of Nutrition. Nutrients 2021, 13, 1180.
- Shibata, R.; Sato, K.; Kumada, M.; Izumiya, Y.; Sonoda, M.; Kihara, S.; Ouchi, N.; Walsh, K. Adiponectin accumulates in myocardial tissue that has been damaged by ischemia-reperfusion injury via leakage from the vascular compartment. Cardiovasc. Res. 2007, 74, 471–479.
- Farkhondeh, T.; Llorens, S.; Pourbagher-Shahri, A.M.; Ashrafizadeh, M.; Talebi, M.; Shakibaei, M.; Samarghandian, S. An Overview of the Role of Adipokines in Cardiometabolic Diseases. Molecules 2020, 25, 5218.
- Puchałowicz, K.; Kłoda, K.; Dziedziejko, V.; Rać, M.; Wojtarowicz, A.; Chlubek, D.; Safranow, K. Association of Adiponectin, Leptin and Resistin Plasma Concentrations with Echocardiographic Parameters in Patients with Coronary Artery Disease. Diagnostics 2021, 11, 1774.
- Fedorova, T.; Semenenko, N.; Tazina, S.; Mamonov, A.; Sotnikova, T. Metabolic syndrome and chronic heart failure: A modern aspect of the problem. Bangladesh J. Med. Sci. 2022, 21, 105–113.
- Tosun, Ş.A.; Gurbuz, T.; Cebi, A.; Tosun, A.; Gokmen, O.; Usta, M. Association of increased levels of omentin-1 and carotid intima-media thickness with early signs of cardiovascular risk in patients with polycystic ovary syndrome: A prospective case control study. J. Obstet. Gynaecol. Res. 2021, 48, 169–177.
- Song, Y.; Song, F.; Wu, C.; Hong, Y.-X.; Li, G. The roles of epicardial adipose tissue in heart failure. Heart Fail. Rev. 2020, 27, 369–377.
- Kumada, M.; Kihara, S.; Sumitsuji, S.; Kawamoto, T.; Matsumoto, S.; Ouchi, N.; Arita, Y.; Okamoto, Y.; Shimomura, I.; Hiraoka, H.; et al. Coronary artery disease. Association of hypoadiponectinemia with coronary artery disease in men. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 85–89.
- Woodward, L.; Akoumianakis, I.; Antoniades, C. Unravelling the adiponectin paradox: Novel roles of adiponectin in the regulation of cardiovascular disease. J. Cereb. Blood Flow Metab. 2016, 174, 4007–4020.
- Zhao, S.; Kusminski, C.M.; Scherer, P.E. Adiponectin, Leptin and Cardiovascular Disorders. Circ. Res. 2021, 128, 136–149.
- Mado, H.; Szczurek, W.; Gąsior, M.; Szyguła-Jurkiewicz, B. Adiponectin in heart failure. Futur. Cardiol. 2021, 17, 757–764.
- Diep Nguyen, T.M. Adiponectin: Role in physiology and pathophysiology. Int. J. Prev. Med. 2020, 11, 136.
- Xu, W.; Tian, M.; Zhou, Y. The relationship between insulin resistance, adiponectin and C-reactive protein and vascular endothelial injury in diabetic patients with coronary heart disease. Exp. Ther. Med. 2018, 16, 2022–2026.
- Honda, M.; Tsuboi, A.; Minato-Inokawa, S.; Kitaoka, K.; Takeuchi, M.; Yano, M.; Kurata, M.; Wu, B.; Kazumi, T.; Fukuo, K. Association of family history of type 2 diabetes with blood pressure and resting heart rate in young normal weight Japanese women. Diabetol. Int. 2021, 13, 220–225.
- Gar, C.; Thorand, B.; Herder, C.; Sujana, C.; Heier, M.; Meisinger, C.; Peters, A.; Koenig, W.; Rathmann, W.; Roden, M.; et al. Association of circulating MR-proADM with all-cause and cardiovascular mortality in the general population: Results from the KORA F4 cohort study. PLoS ONE 2022, 17, e0262330.
- Kadoglou, N.P.E.; Korakas, E.; Karkos, C.; Maratou, E.; Kanonidis, I.; Plotas, P.; Papanas, N.; Moutsatsou, P.; Ikonomidis, I.; Lambadiari, V. The prognostic role of RBP-4 and adiponectin in patients with peripheral arterial disease undergoing lower limb endovascular revascularization. Cardiovasc. Diabetol. 2021, 20, 221.
- Hao, G.; Li, W.; Guo, R.; Yang, J.-G.; Wang, Y.; Tian, Y.; Liu, M.-Y.; Peng, Y.-G.; Wang, Z.-W. Serum total adiponectin level and the risk of cardiovascular disease in general population: A meta-analysis of 17 prospective studies. Atherosclerosis 2013, 228, 29–35.
- Lawlor, D.A.; Smith, G.D.; Ebrahim, S.; Thompson, C.; Sattar, N. Plasma Adiponectin Levels Are Associated with Insulin Resistance, But Do Not Predict Future Risk of Coronary Heart Disease in Women. J. Clin. Endocrinol. Metab. 2005, 90, 5677–5683.
- Menzaghi, C.; Trischitta, V. The Adiponectin Paradox for All-Cause and Cardiovascular Mortality. Diabetes 2017, 67, 12–22.
- Rojas, E.; Rodríguez-Molina, D.; Bolli, P.; Israili, Z.H.; Faria, J.; Fidilio, E.; Bermúdez, V.; Velasco, M. The Role of Adiponectin in Endothelial Dysfunction and Hypertension. Curr. Hypertens. Rep. 2014, 16, 463.
- Kalaycıoğlu, E.; Çetin, M.; Özyıldız, A.G.; Kırış, T.; Turan, T. Is Adiponectin Elevation Associated with Left Atrial Remodeling and Impaired Mechanical Functions? (a Speckle Tracking Study). Kardiologiia 2021, 61, 65–70.
- Semple, R.K.; Halberg, N.H.; Burling, K.; Soos, M.A.; Schraw, T.; Luan, J.; Cochran, E.K.; Dunger, D.B.; Wareham, N.J.; Scherer, P.E.; et al. Paradoxical Elevation of High–Molecular Weight Adiponectin in Acquired Extreme Insulin Resistance Due to Insulin Receptor Antibodies. Diabetes 2007, 56, 1712–1717.
More
Information
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
1.4K
Entry Collection:
Biopharmaceuticals Technology
Revisions:
2 times
(View History)
Update Date:
12 Jul 2022
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No