Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Marek Zbigniew Gogacz | -- | 1557 | 2022-04-20 14:33:20 | | | |
| 2 | Dean Liu | -1 word(s) | 1556 | 2022-04-21 04:32:25 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Gogacz, M.; Kopeć, M.; Dłuski, D.; Winkler, I.; Kotarski, J.; Rechberger, T. Quality of Life Women Suffering from Endometriosis. Encyclopedia. Available online: https://encyclopedia.pub/entry/22023 (accessed on 25 June 2026).
Gogacz M, Kopeć M, Dłuski D, Winkler I, Kotarski J, Rechberger T. Quality of Life Women Suffering from Endometriosis. Encyclopedia. Available at: https://encyclopedia.pub/entry/22023. Accessed June 25, 2026.
Gogacz, Marek, Monika Kopeć, Dominik Dłuski, Izabela Winkler, Jan Kotarski, Tomasz Rechberger. "Quality of Life Women Suffering from Endometriosis" Encyclopedia, https://encyclopedia.pub/entry/22023 (accessed June 25, 2026).
Gogacz, M., Kopeć, M., Dłuski, D., Winkler, I., Kotarski, J., & Rechberger, T. (2022, April 20). Quality of Life Women Suffering from Endometriosis. In Encyclopedia. https://encyclopedia.pub/entry/22023
Gogacz, Marek, et al. "Quality of Life Women Suffering from Endometriosis." Encyclopedia. Web. 20 April, 2022.
Copy Citation
Quality of life is related to good health, family relations, feeling of self-esteem, and ability to cope with difficult situations. Endometriosis is a chronic condition which affects different areas of life.
mental health
sexual dysfunction
sexuality
1. Quality of Life
The term “quality of life” appeared in medical literature in the 1960s and has become increasingly popular in recent decades. It is often defined as sense of well-being, health, comfort, and happiness experienced by an individual or group. Basic indicators include wealth, employment, the environment, physical and mental health, education, recreation and leisure time, social belonging, religious beliefs, safety, security, and freedom. Although happiness is subjective and difficult to measure, the rest of the parameters may be estimated [1]. In health care, quality of life is often regarded in terms of how a certain disease/state affects a patient on an individual level [2]. There are various questionnaires and tests examining the quality of life in patients with endometriosis. The most frequently used include: EHP-30 (Endometriosis Health Profile-30 items), EHP-5 (Endometriosis Health Profile-5 items), SF-36 (Short Form-36), WHO QOF-100 (World Health Organization Quality of Life Questionnaire), and WHO QOL BREF (World Health Organization Quality of Life Assessment) [3].
One of the most cited components in literature referred to endometriosis and how it may affect the quality of women’s lives are social support, self-image, relationships, profession, access to treatment, and infertility. In the study performed by Muharam et al. (2022), scientists noticed that the lowest scores referred to emotional disturbances in relationship between mothers and their children. They also stressed the possibility of alcohol addiction occurrence, attention deficit, or hyperactivity disorders. Another factor correlated with the disease and quality of life was available treatment method, which might enable a control of powerlessness in a daily activity. The analysis also showed moderate correlation between the disease, self-imagine, and social support [4]. In the study conducted by Bień et al. (2020), acceptance of illness in patients who took part in the research has maintained on moderate level. A total of 9 out of 10 women assessed the treatment as expensive. Better scores in well-being were achieved by women with high education. In the questionnaire, patients highlighted general health and local environment as important factors that had an impact on quality of life. Women with endometriosis may manifest lower quality of life in comparison to healthy women with the same symptoms. An interesting topic seems to be how age affects the perception of illness and well-being. Bień et al. described that older patients indicated worsen quality of life. Morandi et al. expanded this issue and noticed similarities and differences on different age. Common aspects in all patients with endometriosis concerned marital relations, social life, illnesses, and mental health. For women between 25 and 34 years of age, the most important aspects that affected well-being were employment, financial situation for those who were above 35, and education below 24. The next aspect concerned perception of one’s own body. The scientists after the analysis of the work concluded that women with obesity scored the lowest points. They were less satisfied with themselves and their intimate life [5][6].
2. Physical and Mental Symptoms of Endometriosis
The quality of life of women suffering from endometriosis is influenced by many factors. The most significant is unpredictable pain, occurring periodically, with different degrees of severity, which causes about 38% reduction of work productivity [7][8][9]. Several working days missed generate direct and indirect costs comparable to diabetes, migraine, asthma, or rheumatoid arthritis [10][11]. Pokrzywinski et al. (2020) report in their study that employed women who suffer from endometriosis may be 16.5 (±11.4) h unable to work per week, whereas the household group were 8.3 (±8.7) h per week [12]. They reported negative career effects or low performance related to endometriosis. In many cases, this is not only abdominal pain but also pain during defecation and urination, making daily life difficult. It is associated with constant taking of analgesics and a feeling of living with a chronic disease [13][14][15] (Figure 1).
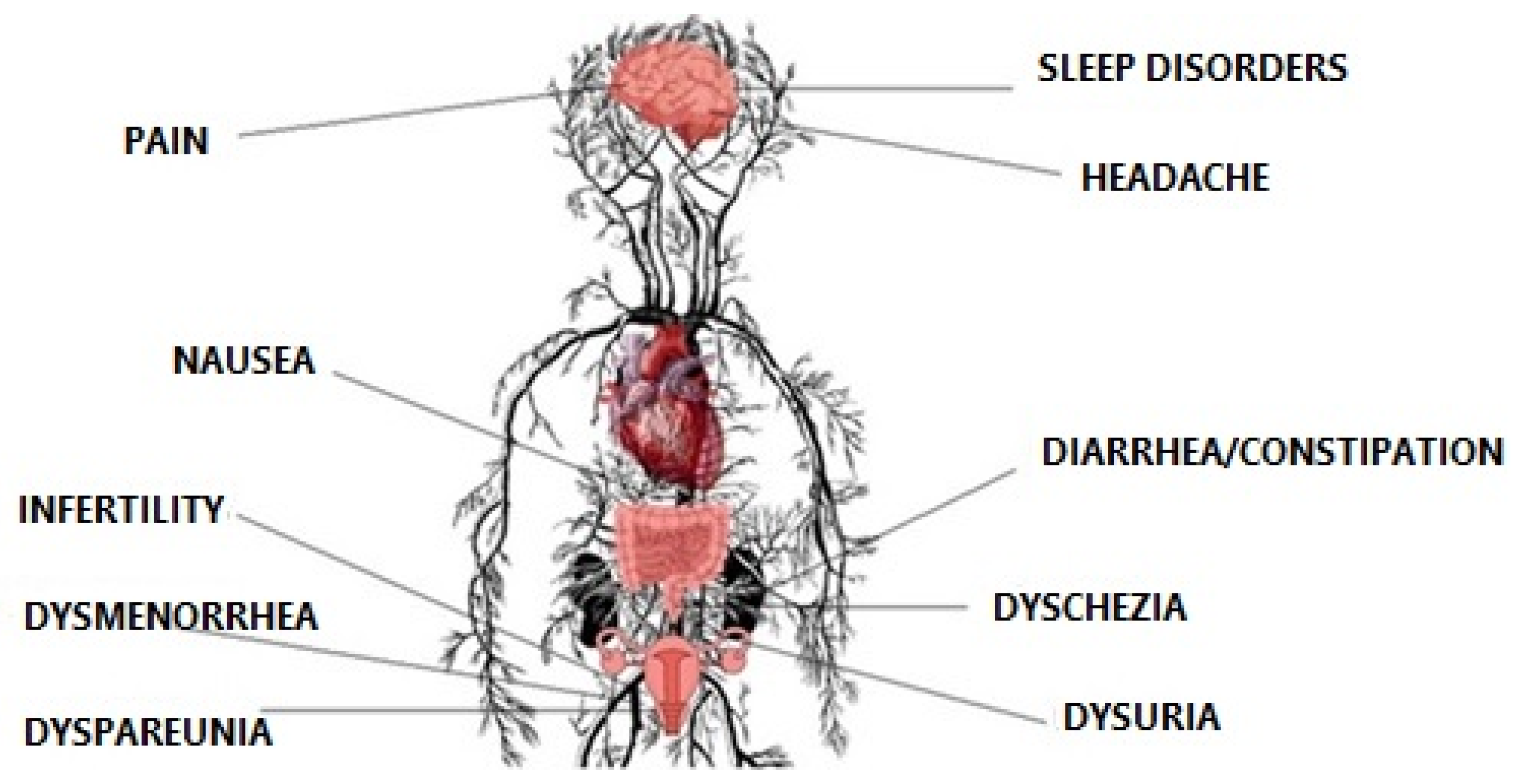
Figure 1. Physical symptoms of endometriosis.
Some women may additionally feel fear of pain occurrence, strong need to control it, intrusive worry thoughts, catastrophizing, self-blame, and ruminations [16] (Figure 2). Women with confirmed endometriosis experience significantly more symptoms of depression (standardized mean difference [SMD] of 0.71 (95% confidence interval [CI] 0.36–1.06)) and anxiety (SMD 0.60 (95% CI 0.35–0.84)) in comparison to healthy ones (SMD −0.01 (95% CI −0.17 to 0.15) for depression and SMD −0.02 (95% CI −0.22 to 0.18) for anxiety) [17]. Ceran et al. (2020) obtained comparable results in which a significant difference was found between the endometriosis and non-endometriosis groups regarding depression scores [18]. Autoimmune diseases, accompanying endometriosis, aggravate the somatic and mental condition of patients [19]. Other symptoms appear and other drugs are constantly taken. Verket et al. (2018) compared in their research the mean scores for SF-36 scales vitality, social functioning, and mental health between two groups of patients—with endometriosis and rheumatoid arthritis. Women with moderate to severe endometriosis scored only 33.4, 62.7, and 66.3 points whereas with rheumatoid arthritis 42.7, 68.8, and 72.6 points [20]. It is worth adding that individual conceptualization of pain in endometriosis may be affected by different social cultures in different races. Asian patients tend to normalize pain, while Caucasian patients are more likely to seek health care. The intensity of pain symptoms may be significantly lower in Chinese population than Russian or French. Moreover, Italian patients with endometriosis may suffer more from severe pelvic pain than Chinese women, suggesting a different cultural background [21][22].
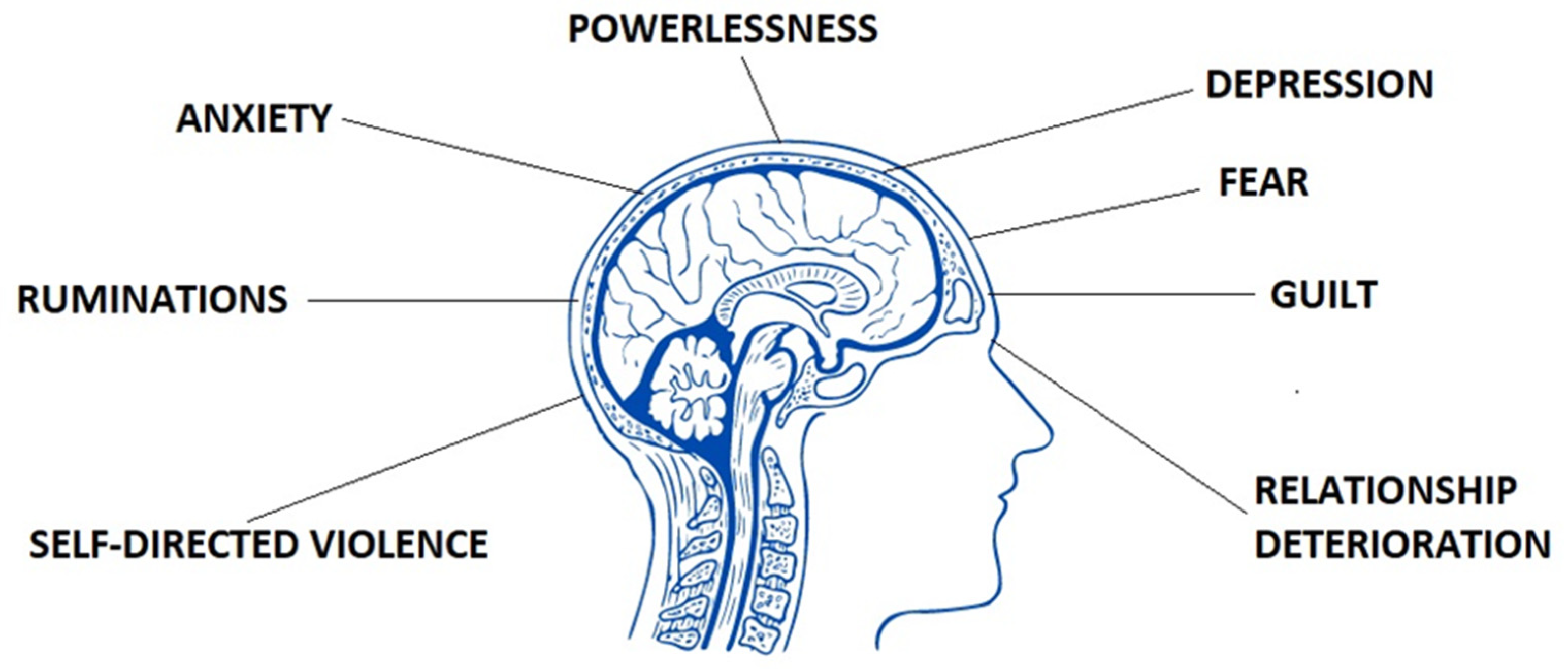
Figure 2. Mental states which may occur in women who suffer from endometriosis.
Patients with endometriosis treated surgically are exposed to stress related to hospitalization and the operation itself. Approximately 88% of the patients suffer from depression and anxiety [23][24]. What is more, they often suffer from poor quality of sleep. In the observational cross-sectional study conducted by Vannuccini et al. (2018) patients who filled the ‘Patient Health Questionnaire’ (PHQ) were affected in 59% by at least one psychiatric disorder. This observation correlated with pain symptoms (p = 0.0026). There was no correlation between the presence of psychiatric disorders and age, BMI, parity, infertility, need for surgery, number of interventions, localization of endometriotic lesions, and systemic comorbidities. Moreover, the research also revealed that patients with severe pain showed a higher incidence of multiple psychiatric disorders (p = 0.026) [25]. Due to the recurrent nature of the disease, they must be frequently operated on several times during their lifetime, which increases discomfort. In the case of endometriosis of the urinary system or lower part of the gastrointestinal system, some patients undergo extensive operations leading to significant mutilation, thus greatly lowering the comfort of life. The surgical procedure within the abdominal cavity also involves the risk of postoperative adhesions formation. This problem additionally complicates the course of the main disease and is a source of more pain [26].
3. Conclusions
Endometriosis affects almost every third woman at the reproductive age, especially between 25 and 29 years of age. Only 22.8% of them are asymptomatic. Some predisposing factors for endometriosis development may include low BMI, early menarche, and nulliparity. It is treated as a chronic illness, which is frequently accompanied by diseases from the autoimmune group. It has an impact on both mental and physical quality of life. The main symptom of the disease is chronic pain localized mainly in the pelvis minor [27][28][29]. The patients also complain of other burdensome symptoms. Painful defecation, regarded as a consequence of deep infiltration, is frequently pointed as positively correlated factor with the stage of the disease. Mental disturbances in the form of anxiety states and even depression with the mean age of 22.2 have been observed in women with the disease. Early screening for detection of the first signs of low mood leading to depression is highly advised. An additional problem, which leads to worsening the emotional condition of the patients, is infertility induced by the disease. It has been reported that almost every second woman with endometriosis cannot be a parent, which is indisputably one of the basic needs in human life. The phenomenon varies between 3.5% and 16.7% depending on the region of the world, women’s age, and comorbidities. It is caused not only by deterioration in the relationship with the partner and avoidance of sexual contacts due to pain, but also by the very course and complications of endometriosis at the molecular level. Based on the above observations, it is worthwhile to emphasize that women who suffer from endometriosis become pregnant later than unaffected ones, which may be associated with a higher risk of perinatal complications. Powerlessness and resigned attitude to life may also negatively affect relations with children, increasing the sense of lack of parental attention and their self-confidence. It is estimated that evolution of the disease has a negative influence on the quality of life in most of the patients. Over time and severity of the disease, women manifest more frequent fatigue in daily life, somatization, and stress.
Treatment of endometriosis, both pharmacological as well as surgical, can improve the patients’ quality of life. Pharmacotherapy significantly reduces the use of surgical procedures that deteriorate the ovarian reserve. Less invasive operative procedures are recommended. Due to 75.9% of women who report taking OTC, variety of pain sensations that do not correlate with the severity of the disease, the use of other nonconventional ways to alleviate the symptoms, such as psychotherapy, a healthy diet, physical activity, herbal therapies, and others, are recommended. The attitude of patients towards the disease and its course and acceptance of life with a chronic disease seems important. A better comprehension of all bio-psycho-social aspects implicated in women’s well-being and pain experience on endometriosis needs further research in the near future.
References
- Hanson, K.; Brikci, N.; Erlaanga, D. Quality of Life, the Degree to Which an Individual Is Healthy, Comfortable, and Able to Participate in or Enjoy Life Events. 2016. Available online: https://www.britannica.com/topic/quality-of-life (accessed on 31 March 2022).
- Pirie, K.; Peto, R.; Green, J.; Beral, V. Health and Happiness. Lancet 2016, 387, 1251.
- Yang, X.; Xu, X.; Lin, L.; Xu, K.; Xu, M.; Ye, J.; Shen, X. Sexual function in patients with endometriosis: A prospective case-control study in China. J. Int. Med. Res. 2021, 49, 3000605211004388.
- Muraham, R.; Amalia, T.; Pratama, G.; Harzif, A.K.; Agiananda, F.; Faidarti, M.; Azyati, M.; Sumapraja, K.; Winarto, H.; Wiweko, B.; et al. Chronic Pelvic Pain in Women with Endometriosis is Associated with Psychiatric Disorder and Quality of Life Deterioration. Int. J. Womens Health. 2022, 4, 131–138.
- Bień, A.; Rzońca, E.; Zarajczyk, M.; Wilkosz, K.; Wdowiak, A.; Iwanowicz-Palus, G. Quality of life in women with endometriosis: A cross-sectional survey. Qual. Life Res. 2020, 29, 2669–2677.
- Warzecha, D.; Szymusik, I.; Wielgos, M.; Pietrzak, B. The impact of Endometriosis on the Quality of Life and the Incidence of Depression—A Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 3641.
- Quinlivan, J.; van den Berg, M. Managing the stigma and women’s physical and emotional cost of endometriosis. J. Psychosom. Obstet. Gynecol. 2021, 42, 1–2.
- Andysz, A.; Jacukowicz, A.; Merecz-Kot, D.; Najder, A. Endometriosis—The challenge for occupational life of diagnosed women: A review of quantitative studies. Med. Pr. 2018, 69, 663–671.
- Sullivan-Myers, C.; Sherman, K.A.; Beath, A.P.; Duckworth, T.J.; Cooper, M.J.W. Delineating sociodemographic, medical and quality of life factors associated with psychological distress in individuals with endometriosis. Hum. Reprod. 2021, 36, 2170–2180.
- La Rosa, V.L.; De Franciscis, P.; Barra, F.; Schiattarella, A.; Török, P.; Shah, M.; Karaman, E.; Cerentini, M.T.; Di Guardo, F.; Gullo, G.; et al. Quality of life in women with endometriosis: A narrative overview. Minerva Med. 2020, 111, 68–78.
- Soliman, A.M.; Coyne, K.S.; Gries, K.S.; Castelli-Haley, J.; Snabes, M.C.; Surrey, E.S. The effect of endometriosis symptoms on absenteeism and presenteeism in the workplace and at home. J. Manag Care Spec. Pharm. 2017, 23, 745–754.
- Pokrzywinski, R.M.; Soliman, A.M.; Chen, J.; Snabes, M.C.; Agarwal, S.K.; Coddington, C.; Coyne, K.S. Psychometric assessment of the health-related productivity questionnaire (HRPQ) among women with endometriosis. Expert Rev. Pharmacoecon. Outcomes Res. 2020, 20, 531–539.
- Rossi, V.; Tripodi, F.; Simonelli, C.; Galizia, R.; Nimbi, F.M. Endometriosis-associated pain: A review of quality of life, sexual health and couple relationship. Minerva Obstet. Gynecol. 2021, 73, 536–552.
- Casalechi, M.; Vieira-Lopes, M.; Quessada, M.P.; Arão, T.C.; Reis, F.M. Endometriosis and related pelvic pain: Association with stress, anxiety and depressive symptoms. Minerva Obstet. Gynecol. 2021, 73, 283–289.
- Guidone, H.C. The Womb Wanders Not: Enhancing Endometriosis Education in a Culture of Menstrual Misinformation; Palgrave Macmillan: Singapore, 2020; Volume 22.
- Zarbo, C.; Brugnera, A.; Dessì, V.; Barbetta, P.; Candeloro, I.; Secomandi, R.; Betto, E.; Malandrino, C.; Bellia, A.; Trezzi, G.; et al. Cognitive and Personality Factors Implicated in Pain Experience in Women with Endometriosis: A Mixed-Method Study. Clin. J. Pain 2019, 35, 948–957.
- Van Barneveld, E.; Manders, J.; van Osch, F.H.M.; van Poll, M.; Visser, L.; van Hanegem, N.; Lim, A.C.; Bongers, M.Y.; Leue, C. Depression, Anxiety, and Correlating Factors in Endometriosis: A Systematic Review and Meta-Analysis. J. Womens Health 2022, 31, 219–230.
- Ceran, M.U.; Yilmaz, N.; Ugurlu, E.N.; Erkal, N.; Ozgu-Erdinc, A.S.; Tasci, Y.; Gulerman, H.C.; Engin-Ustun, Y. Psychological domain of quality of life, depression and anxiety levels in in vitro fertilization/intracytoplasmic sperm injection cycles of women with endometriosis: A prospective study. J. Psychosom. Obstet. Gynaecol. 2020, 1–8.
- Surrey, E.S.; Soliman, A.M.; Johnson, S.J.; Davis, M.; Castelli-Haley, J.; Snabes, M.C. Risk of developing comorbidities among women with endometriosis: A retrospective matched cohort study. J. Women’s Health 2018, 27, 1114–1123.
- Verket, N.J.; Uhlig, T.; Sandvik, L.; Andersen, M.H.; Tanbo, T.G.; Qvigstad, E. Health-related quality of life in women with endometriosis, compared with the general population and women with rheumatoid arthritis. Acta Obstet. Gynecol. Scand. 2018, 97, 1339–1348.
- Yudell, M.; Roberts, D.; DeSalle, R.; Tishkoff, S. Science and society. Taking race out of human genetics. Science 2016, 351, 564–565.
- Chapron, C.; Lang, J.H.; Leng, J.H.; Zhou, Y.; Zhang, X.; Xue, M.; Popov, A.; Romanov, V.; Maisonobe, P.; Cabri, P. Factors and regional differences associated with endometriosis: A multi-country, case-control study. Adv. Ther. 2016, 33, 1385–1407.
- Chen, H.; Vannuccini, S.; Capezzuoli, T.; Ceccaroni, M.; Mubiao, L.; Shuting, H.; Wu, Y.; Huang, H.; Petraglia, F. Comorbidities and Quality of Life in Women Undergoing First Surgery for Endometriosis: Differences between Chinese and Italian Population. Reprod. Sci. 2021, 28, 2359–2366.
- Yela, D.A.; Quagliato, I.P.; Benetti-Pinto, C.L. Quality of Life in Women with Deep Endometriosis: A Cross-Sectional Study. Rev. Bras. Ginecol. Obs. 2020, 42, 90–95.
- Vannuccini, S.; Lazzeri, L.; Orlandini, C.; Morgante, G.; Bifulco, G.; Fagiolini, A.; Petraglia, F. Mental health, pain symptoms and systemic comorbidities in women with endometriosis: A cross-sectional study. J. Psychosom. Obstet. Gynaecol. 2018, 39, 315–320.
- Vannuccini, S.; Reis, F.M.; Coutinho, L.M.; Lazzeri, L.; Centini, G.; Petraglia, F. Surgical treatment of endometriosis: Prognostic factors for better quality of life. Gynecol. Endocrinol. 2019, 35, 1010–1014.
- Florentino, A.V.A.; Pereira, A.M.G.; Martins, J.A.; Lopes, R.G.C.; Arruda, R.M. Quality of life assessment by the endometriosis health profile (EHP-30) questionnaire prior to treatment for ovarian endometriosis in Brazilian women. Rev. Bras. Ginecol. Obstet. 2019, 41, 548–554.
- Marinho, M.C.P.; Magalhaes, T.F.; Fernandes, L.F.C.; Augusto, K.L.; Brilhante, A.V.M.; Bezerra, L.R.P.S. Quality of Life in Women with Endometriosis: An Integrative Review. J. Women’s Health 2018, 27, 399–408.
- Rees, M.; Kiemle, G.; Slade, P. Psychological variables and quality of life in women with endometriosis. J. Psychosom. Obstet. Gynaecol. 2020, 1–8.
More
Information
Subjects:
Obstetrics & Gynaecology
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
861
Revisions:
2 times
(View History)
Update Date:
26 Apr 2022
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No